


Abstract
In the present article, we described a case of treating intractable pain from failed back surgery syndrome (FBSS) and multiple sclerosis (MS) after implantation of spinal cord stimulation (SCS) in a patient. We are reporting a case where SCS has been used for treating a patient with both FBSS and MS.
Multiple Sclerosis (MS) is a chronic demyelinating autoimmune disease and the most frequently occurring type of neuronal demyelination. Multiple Sclerosis may show various neurological manifestations, including neuropathic pain, dysesthesia and paraesthesia in approximately 75% of the patients, based on the severity of nerve damage.1 The associated neuropathic pain accounts for 30% of all MS symptomatic medication. However, medical treatment is generally unresponsive or inadequate for the management of this pain.1
Failed back surgery syndrome is the most common indication for spinal cord stimulation (SCS). It is often characterised by disabled back or radicular limb pain following spinal surgery, with neuropathic and nociceptive components that are often insufficiently responsive to conventional therapies such as reoperation or medical treatment.2
Neuropathic pain may develop secondary to a primary lesion in the nervous system or due to nervous system dysfunction. Depending on the location of the lesion in the nervous system, it is classified as either central or peripheral neuropathic pain. Due to insufficient epidemiological research and follow-up, the exact prevalence of neuropathic pain remains unknown. However, it is estimated that approximately 1-1.5% of the population is affected by it.
Spinal cord laminae I, II and V receive information from nociceptive afferent fibres of the dorsal root ganglia.3 Although nociceptive information is transmitted to higher centres for processing, it can be modified at primary afferent nerve terminals and at the presynaptic junction of projection neurones in the dorsal horn of the spinal cord.
Spinal cord stimulation-induced analgesia involves neurophysiological and neurochemical mechanisms. Spinal cord stimulation activates the dorsal column and inhibitory interneurons that attenuate pain.3
Neurostimulation is a known effective treatment for neuropathic pain.1 Therefore, we aimed to determine whether SCS is successful in treating intractable pain in a patient with MS and FBSS.
Case Report
Patient information
A 59-year-old female patient was diagnosed with MS 13 years ago, which was confirmed radiologically (Figure 1). She had a paraesthesia on her both upper extremities and right leg. Right leg and back pain added to her initial complaints 10 years ago. Pain had a radicular character. She was diagnosed with right L4-5 intervertebral disc herniation. Patient underwent physical therapy and medical treatment for one year, but complaints were not resolved. Therefore, decision of surgery was made. Right L4-5 intervertebral discectomy was performed and complaints on right leg pain had resolved. A year later patient developed recurrent intervertebral disc herniation and segmental instability, thus posterior lumbar stabilisation and reccurent invertebral discectomy was performed. Patient’s complaints started to increase after a short period of alleviation and radicular pain got neuropathic character (numbness, tingling and stinging on the right leg). She presented with FBSS with maximum medical treatment (Nonsteroidal anti-inflammatory drugs [NSAID] and gabapentin for neuropathic pain) and interventional pain procedures (such as epiduroscopy and facet joint blockage several times during physical therapy), both of which were unsuccessful in alleviating her pain. The patient reported a pain degree of 10/10 on visual analogue scale (VAS). Her Oswestry disability index score was 92/100. Therefore, despite being under medical therapy for MS and FBSS, she suffered from severe disability. Since the patient’s pain was not alleviated with any medical and surgical treatment, it was thought that pain was related due to FBSS, MS, and SCS was decided (Table 1).

In T2 sagittal MRI scan, hyperintense MS plaque is seen at C3, C4 level (black arrow) (A). In T2 Flair axial brain MRI scan, many hyperintense MS plaques (black arrow) are seen (B).
Timeline of patient’s disease from initial and follow-up visits.
Clinical findings
Upon physical examination, it was reported that she had right leg and back pain for 10 years. Her right leg and arm muscle power levels were both 3/5 and right foot dorsiflexion motor power was −3/5. She demonstrated spasticity (1; on the modified Ashworth scale) and reduced sensation on the L5 and S1 dermatomes. Due to claudication, the patient could only walk a distance of approximately 50 metres. She was using betaferon (interferon beta-1b) for approximately 13 years. Her last MS attack was 5 years ago. She has a relapsing remitting form of MS.
Diagnostic assessment
Patient had multiple spinal cord and brain lesions as confirmed by magnetic resonance imaging (MRI) (Figure 1). The spinal cord lesions were considered to be the cause of her limb and back pain. Electromyography (EMG) was compatible with motor and sensory axonal neuropathy.
Therapeutic intervention
After psychometric analysis and multidisciplinary team discussion, we decided to implant the STIMWAVE spinal cord stimulator system. This system has 8 electrodes, 2 percutaneous leads, transmitter and a battery (but in this system battery is outside of the body). After minimal Th12 laminectomy, the leads were advanced through the epidural spaces. First lead tips were placed at the midline portion of the middle of the T9 vertebral body and second lead tips were placed at the upper endplate of the T8 vertebral body (Figure 2).
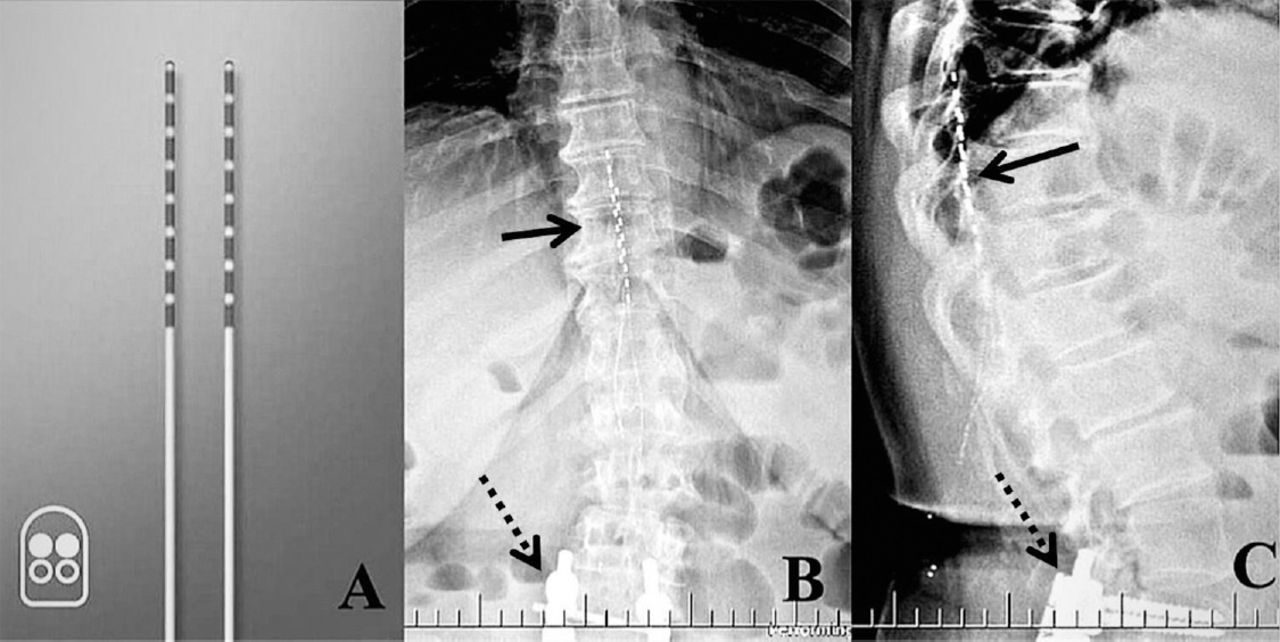
Stimwave spinal cord stimulator system (A). This system had 8 electrodes, 2 percutaneous leads and a transmitter. Postoperative anteroposterior (B) and lateral x-rays (C) show the electrodes of SCS (black arrow), previous screw system (dotted arrow).
Follow-up and outcomes
Significant improvement in pain was reported. Her pre-implantation VAS was 10 points and post-implantation VAS was 3. Her Oswestry disability index score was 92/100 and post-implantation was 36/100. She could perform and participate in her day-to-day activities. In addition, analgesic medication consumption was reduced, degree of spasticity decreased, and she reported good coverage of pain without complications.
Discussion
Spinal cord stimulation is approved by the United States of America’s Food and Drug Administration (FDA) as a medication of low back pain, chronic trunk and limb pain. Also it used in conditions such as failed-back syndrome, lumbar radiculopathy and complex regional pain syndrome (CPRS).4 As mentioned in the literature SCS in MS are insufficient, and nearly all of them were written few decades ago. According to Young et al,5 the lack of significant recovery in sensory, motor, or bladder functions were seen in 23 patients with MS. Those patients were under control for a period of 32 months.
Kumar et al6 reported one of the biggest longitudinal cohort study. All of the patients were reported in 2006’s article, 19 patients with MS, who have complaints of chronic pain in the lower extremity were trialed and 17 of them were implanted. The time mean of the follow-up was 97 months, 74,1% patients of the cohort retained notable pain improvement after implantation.6 Spinal cord stimulation has presented efficacious and cost-effective treatment for many chronic neuropathic pain conditions.7 The FBSS involves neuropathic and nociceptive pain elements.8 Healthcare providers have established many management options. Initial conservative management recommended from the guidelines. For neuropathic pain, oral amitriptyline, gabapentin, or pregabalin are prior treatment methods when pharmacological options are concerned.8 Spinal cord stimulation is highly recommended when conservative treatment does not bring pain relief regarding therapy-refractory FBSS.8 In the United States of America, FBSS is the most common indication for SCS.8
Interventional processes and multiple drugs are used for treating MS-associated pain and failed back pain.1 However, some patients do not experience adequate pain relief with these treatments. Spinal cord stimulation may be considered for these patients.
Developments in pain scores, functional outcomes, urodynamic function, and quality-of-life scores are the most frequently reported benefits of SCS treatment in both condition FBSS and MS.1 Previous publications have reported a complication rate of 36%, where lead migration is the most commonly reported complication.1
We made a search of published papers in English language in PubMED database up to March 2019 by using ‘Failed back surgery syndrome’, ‘Multiple sclerosis’, ‘Spinal cord stimulation’ as keywords. No patient has been described with presentation of FBSS and concomittant MS in neurosurgical literature so far. This is the first case demonsrating the use SCS in a patıent who presented wıth both FBSS and MS.6,9 In conclusion, we describe a successful case of treating intractable pain from FBSS and MS in a patient after implantation of SCS. Failed back surgery syndrome is the most common indication for SCS. Information regarding the effectiveness of SCS for MS pain is lacking in the literature. In our case, implantation of SCS in a patient with MS and FBSS produced a successful response to intractable pain.
Acknowledgements
The authors gratefully acknowledge ENAGO English Editing Company (https://www.enago.com/) for English language editing, the Radiology Department of Private MedicalPark Hospital Ankara, Turkey and the authors would like to thank Elif Gunaydin for reviewing the figure for clarity and correctness.
Footnotes
Disclosure. The authors declare no conflicting interests, support or funding from any drug company.
- Received December 26, 2018.
- Accepted March 10, 2019.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.