


Abstract
Objectives: To investigate the levels of knowledge and attitudes toward epilepsy surgery among neurologists in Saudi Arabia and evaluate the factors that affect the physicians’ knowledge and attitudes.
Methods: A quantitative observational cross-sectional study conducted at King Saud University Medical City, Riyadh. The data were collected using a newly developed, self-administered online questionnaire. The questionnaire contained 3 sections: demographic information, knowledge, and attitudes which then sent to neurologist in Saudi Arabia from December 2016 to March 2017.
Results: A total of 106 neurologists met our inclusion criteria. Eighty percent of the participants had at least one epilepsy center in their city, and 78% indicated that they had access to adequate expertise and resources to enable the appropriate selection of epilepsy surgical candidates. Only 57.5% of the neurologists had a sufficient level of knowledge regarding epilepsy surgery. Neurologists with higher level of knowledge referred more patients to EMU and discussed epilepsy surgery more often with their patients. Overall, more than half of the neurologists (52.8%) had a positive attitude toward epilepsy surgery. There was a significantly positive correlation between the scores of knowledge and attitude (p<0.001).
Conclusion: Neurologists in Saudi Arabia appear to have moderate knowledge of and positive attitudes toward epilepsy surgery. The place of the last neurology certificate, type of practicing hospital, and access to expertise and resources, affected their knowledge. Adequate knowledge was positively correlated with attitude.
Epilepsy is one of the most common neurological disorders in Saudi Arabia, with an estimated prevalence of 6.54 per 1000 individuals.1 It is estimated that 20-40% of newly diagnosed patients are expected to fail seizure control with medical treatment.2 Refractory epilepsy is commonly defined as the failure to achieve freedom from seizures despite two or more antiepileptic drugs (AEDs).3 Patients with drug-resistant epilepsy (DRE) have a lower quality of life and face more social difficulties than patients with controlled epilepsy.4-6 More than half of the economic burden of epilepsy is accounted for by patients with refractory epilepsy.7 Epilepsy surgery is the best evidence-based treatment option for these patients with drug resistant focal epilepsy.8,9 The current guidelines for patient referral to epilepsy surgery were published in 2003 by the American Academy of Neurology.9 The benefits of epilepsy surgery may not only reduce the frequency of seizures but might also lower mortality and improve the quality of life.10 Despite its proven efficacy and favorable outcome, the average referral delay of an epilepsy surgery candidate is more than 20 years.11 This delay is predominately attributed to non-adherence to referral guidelines, which results from a lack of awareness and familiarity with them.12 Another factor that contributes to the delay is patients’ misbeliefs regarding the surgery’s risks and benefits, which are highly influenced by physicians’ lack of knowledge.13 Epilepsy surgery was introduced to Saudi Arabia in 1998.14 Several epilepsy surgery centers have subsequently been established across the country. A survey in 2013 showed that 56% of health-care professionals in Saudi Arabia were not aware that surgery was a treatment option for patients with epilepsy.15 Our aims in this study were to investigate the levels of knowledge and attitudes toward epilepsy surgery among neurologists in Saudi Arabia and evaluate the factors that affect the physicians’ knowledge and attitudes.
Methods
A quantitative observational crosssectional study was conducted at King Saud University Medical City (KSUMC), Riyadh, Kingdom of Saudi Arabia. Both adult and pediatric neurologists in Saudi Arabia were included in the study population. Institutional review board approval was granted prior to data collection. The questionnaire was then sent to adult and pediatric neurologist in Saudi Arabia from December 2016 to March 2017.
Questionnaire
An anonymous, self-administered online questionnaire was completed using the Google Documents platform. The questionnaire was developed by 3 neurologists (BJ, TM, and MHA) based on other studies that have measured knowledge, attitudes and perceptions towards epilepsy surgery.16-19 The questionnaire contained 3 sections: demographic information, knowledge, and attitudes. The demographic section included age, gender, training site (residency or fellowship training program), subspecialty, experience, and other questions regarding access and referral habits for epilepsy surgery and epilepsy monitoring unit (EMU). The knowledge section included 11 items that evaluated different aspects of epilepsy surgery knowledge. Each item had one correct answer, one or more incorrect answers, and an “I don’t know” option. A correct response was awarded one point, while any other response was awarded none. Individuals who scored 7 or more were considered to have sufficient knowledge. The attitude section contained 8 items, including both positive and negative attitude statements. These items used a 5-point Likert scale with options of strongly agree, somewhat agree, neither agree nor disagree, somewhat disagree, and strongly disagree, with the exception of one question, which assessed the frequency of discussing epilepsy surgery with patients. The responses were scored from 0 to 4 based on whether the attitude statement was positive or negative. Individuals who scored 25 or more were considered to have a positive attitude. The cutoff points for sufficient or insufficient knowledge and a positive or negative attitude were calculated based on the median score in each section. The questionnaire was subsequently sent to 3 consultants and academic staff in neurology for content validation. A pilot study of 10 neurologists was conducted to assess the clarity of the questions.
Participants
We calculated a required sample size of 96 (Za: 1.96 for 95% confidence level; proportion: 0.5; d: 0.1). The eligibility criteria required individuals to be certified neurologists working in Saudi Arabia. We excluded neurologist who do not manage patients with epilepsy. The questionnaire link was electronically sent to 200 neurologists chosen by convenient sampling. Data were collected in January 2017. The participants provided informed consent by clicking on “agree to participate” icon in the first page of the electronic survey.
Data analysis
Data were analyzed using the Statistical Package for the Social Sciences (IBM, Armonk, NY, USA), version 23. Descriptive data are reported as mean values, standard deviations, and percentages. Categorical variables were compared using the Chi-square test or Fisher’s exact test, as appropriate. Pearson correlation was used to assess the relationships between different variables. Only differences at p<0.05 were considered statistically significant.
Results
Study subjects. One hundred and six adult and pediatric neurologists met our inclusion criteria, Table 1 presents their demographics. Our sample consisted of different subspecialists, which primarily included adult general neurology (22.6%), pediatric neurology (32.1%), epilepsy (16.0%), stroke (12.3%), neuromuscular (6.6%), neuroimmunology (3.8%), clinical neurophysiology (2.8%), movement disorders (1.9%), neurocritical care (0.9%) and neuro-cognitive disorders (0.9%). Seventy-two percent ofthe participants were practicing in tertiary healthcare centers. Eighty percent of the participants had at least one epilepsy center in their city, and 78% indicated that they had access to adequate expertise and resources to enable the appropriate selection of epilepsy surgical candidates. More than half of the sample (57%) saw at least 20 patients with epilepsy each month. Approximately 45% of the participants had referred less than 3 patients to the Epilepsy Monitoring Unit (EMU) for pre-surgical workup in the previous year, 33% had referred 3-10 patients, and only 22% had referred more than 10 patients. With respect to epilepsy surgery referral, 68% of the neurologists had referred less than 3 patients, 20% had referred between 3 and 10 patients and only 12% had referred more than 10 patients in the previous year. Forty percent of the participants indicated that it requires less than 3 months for an epilepsy specialist to see their patients, 38% indicated that it requires 3-6 months, and 22% indicated that it requires more than 6 months. Approximately 27% of the neurologists indicated that it requires less than 3 months for their patients to be evaluated for epilepsy surgery (i.e., EMU, neuropsychology) in the center nearest to them, 35% indicated that it requires 3-6 months, and 38% indicated that it requires more than 6 months for this process.
Responses to the demographics section.
Knowledge
The majority of the participants (73%) stated that they are familiar with the overall content of the American Academy of Neurology clinical practice guidelines on temporal lobe and localized neocortical resections for epilepsy, whereas 67% believed that they have sufficient knowledge regarding epilepsy surgery. The results show that only 57.5% of the neurologists had a sufficient level of knowledge regarding epilepsy surgery, with a mean score of 6.76 out of 11 and a standard deviation of 2.29. The participants’ answers to the knowledge section are shown in Table 2. There was significant variability in the level of knowledge among the neurologists who obtained their last certificate of neurology from different areas (p=0.001): 71% of the neurologists who obtained it from North America had a sufficient level of knowledge, compared with 52% of the neurologists who obtained it from Saudi Arabia and only 10% of the neurologists who obtained it from other areas.
Responses to the knowledge section.
Neurologists with sufficient knowledge were likely to be University staff (p=0.026), have access to adequate expertise and resources (p=0.043), and refer more patients to EMU for pre-surgical work-up (p=0.019). A similar non-significant correlation existed with referral for epilepsy surgery. The neurologists with a high level of knowledge discussed epilepsy surgery more often with their patients (p=0.005). The neurologists with an insufficient level of knowledge tended to believe that surgery should be viewed as a last resort for patients with epilepsy (p<0.001). The neurologists with a sufficient level of knowledge toward epilepsy surgery agreed that it is an underutilized and cost-effective treatment, p=0.01 and p=0.041, respectively.
Attitude
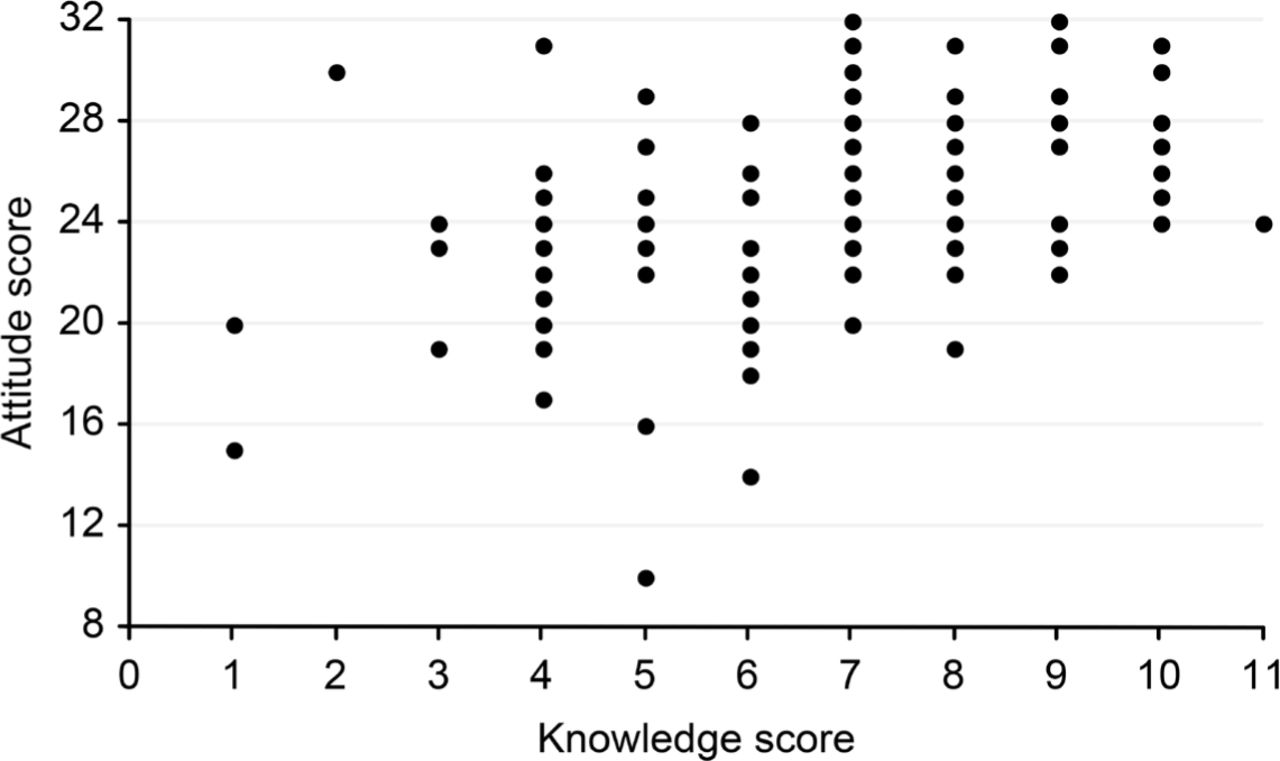
The vast majority of the respondents discuss epilepsy surgery with their patients (97.2%); however, only 48% discuss it frequently. When asked if surgery should be viewed as a last resort for patients with epilepsy, 34% of our sample agreed (Table 3). Ninety-one percent of the neurologists indicated that they would agree to have epilepsy surgery if it was indicated for them. A majority of the neurologists (85.8%) considered epilepsy surgery a cost-effective treatment method, and 90% indicated that it should be available in all tertiary hospitals. Overall, more than half of the neurologists (52.8%) had a positive attitude toward epilepsy surgery. Neurologists who trained abroad were more likely to have a positive attitude (p=0.02). As shown in Figure 1, there was a significantly positive correlation (r=0.437, p<0.001) between the scores of knowledge and attitude.
Responses to the attitude section.

The correlation between knowledge and attitude scores.
Reliability of the scale
The internal consistency reliability of the overall scale was relatively acceptable (Cronbach a = 0.67). Both the knowledge and attitude sections were consistent, with a Cronbach a of 0.65 for knowledge and 0.69 for attitude.
Discussion
This study demonstrates that approximately half of neurologists in Saudi Arabia have adequate knowledge and positive attitudes toward epilepsy surgery. Several previous studies have evaluated neurologists’ knowledge of and attitudes toward epilepsy surgery. These studies have reported variable findings, many of which concur with our results.16-19
The response rate was 53%, which is higher than the average response rate for online surveys.20 With the high response rate from both adult and pediatric neurologists and the use of a reliable instrument, we believe that this study provides a reasonable perspective on the knowledge and attitudes toward epilepsy surgery in Saudi Arabia.
Although surgery is an effective evidence-based method to treat epilepsy, a substantial proportion (42.5%) of neurologists did not have a sufficient level of knowledge regarding it. This finding may be attributed to the low number of epilepsy surgery centers in Saudi Arabia. It may also be a result of the fast development of sub-specialized neurology clinics. One study showed that 65.4% of patients relied on their neurologist or neurosurgeon as the main source of information regarding epilepsy surgery.13 The presence of a sufficient level of knowledge varied based on different variables. More participants who obtained their most recent certificate in neurology from North America had sufficient knowledge, this is like due to the exposure to epilepsy surgery early in their careers as it is more developed in these countries. Individuals who work at university and other tertiary hospitals were more likely to have a sufficient level of knowledge regarding epilepsy surgery. This may be attributed to the fact that most of these hospitals are tertiary centers and provide scholarship programs that enable their neurologists to complete neurology residency training or fellowship abroad. Our study showed that individuals with adequate access to expertise and resources to enable the appropriate selection of epilepsy surgical candidates had more sufficient knowledge, which was expected because it makes them more engaged in and informed about the advances and achievements in this field. Neurologists with sufficient knowledge tended to discuss epilepsy surgery with their patients more frequently. We believe that their adequate knowledge regarding the substantial benefits of epilepsy surgery made them more comfortable proposing the surgical option to their patients. It is important to note that individuals with sufficient knowledge regarding surgery are more likely to develop positive attitudes, likely due to better understanding of indications, risks and benefits of the procedure. This relationship between knowledge and attitudes may also be because individuals with sufficient knowledge may refer more patients for evaluation for epilepsy surgery which results in positive feedback to the referring physicians who then can appreciate the benefits of surgery on their operated patients.
Neurologist in the Kingdom of Saudi Arabia listed the health system organization, patient fears, information and motivation for patients, availability of
education, and hospital organization and administration as the most important obstacles related to epilepsy surgery. Only one-third of the participants considered funding an issue. Interestingly, epilepsy surgery was not discussed frequently by 52% of the participants and not at all by 2.8%. In a previous study conducted by Hakimi et al19 the latter rate was higher at 11%. With regards to cost-effectiveness, 85.8% of our participants considered epilepsy surgery a cost-effective treatment, which is consistent with the results of a study done among Swedish neurologists (92%).18 In the present study, 34% of neurologists considered epilepsy surgery as the last resort, which may be attributed to the misunderstanding of DRE, as only 66% defined it as the failure of seizure control after 2 appropriately chosen AEDs. Among the limitations to consider is the accuracy of survey type assessments, although the content validity was assessed further validation testing of the questionnaire is required to determine its measurement properties. Participants who answered “I don’t know” were considered to lack knowledge. This might not represent their real world practice, as these individuals might actually seek out knowledge when handling certain cases to determine proper disposition of patients.
In conclusion, neurologists in Saudi Arabia appear to have positive attitudes toward epilepsy surgery despite a moderate level of knowledge as measured in this study. Different variables, including the place of the last neurology certificate, type of practicing hospital, and access to expertise and resources, affected their knowledge. Adequate knowledge was positively correlated with attitude.
Acknowledgment
We thank the neurologists who participated in this study. We acknowledge the efforts of the Neuroscience forum and Dr. Mohammed Jan in facilitating the data collection process. We also extend our gratitude to Dr. Abdullah AlRuwaite for his help in searching the literature. Finally, we would like to thank Nature Research Editing Service for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received April 19, 2019.
- Accepted September 26, 2019.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.