


Abstract
Objectives: To find out new assessment tools for sitting, in patients with neurological and neuromuscular conditions, to be recommended for rehabilitation practice locally in Saudi Arabia and internationally.
Methods: Four databases were used: PubMed, Web of Science, Ovid Medline, and Cochrane. Inclusion criteria were articles published between the years 2009–2019; sitting, not standing or walking; assessment not intervention; published in English and studies on adults only. Exclusion criteria were any assessment that measures the standing/walking ability or has items for that, and studies that include pediatric or adolescent or both.
Results: Ten articles met our criteria including 464 patients and divided into 3 main neurological conditions (stroke, SCI, and MS). One assessment (Function in Sitting Test) showed promising potential being implemented with both stroke and multiple sclerosis, Cronbach’s alpha, α were 0.91 and 0.98 indicating high internal consistency. It was used with SCI patients, however, no access was available to include this study in this review.
Conclusion: This review indicates an extension of what was carried out by previous systematic reviews with neurological conditions. It seems that Function in Sitting Test is the most frequent assessment in this review with multiple neurological conditions (stroke, MS and SCI) with high internal consistency and high quality studies according to available data. However, this review showed that there is an absence of evidence for individuals with brain injury. Further work needs to be carried out to address such groups of patients to extend the choices that clinicians can use in rehabilitation sittings.
Setting balance is one of the most important factors in activities of daily living (ADL) performance; it allows patients to engage safely and effectively in selected tasks. Sitting components are varied in the literature between assessing the trunk control as a system that contributes to sitting and addressing the actual sitting attribute via objective measures of functional tasks. One systematic review highlighted this for neurological conditions e.g., (stroke, Parkinson disease and multiple scleroses).1 Another one discussed this for spinal cord injury conditions.2 Both found a total of 31 instruments, with no clear conclusion about an instrument that can be used with the various neurological conditions that address sitting only. Thus, our review is aiming to see if there are any new tools after previous published systematic reviews1 and2 for various neurological conditions and whether the neuromuscular condition has any assessments that capture sitting as a body function and structure impairment resulting from health condition according to the international classification of functioning model ICF.3 Primary investigator (WA) used to work in a rehabilitation sitting when this review was started and search term was run for the first time in September 2018. Therefore, finding new assessment tools for sitting, in patients with neurological or neuromuscular conditions was important for the practice. Furthermore, the result of this review would be an update recommendation, for colleagues who work in mixed in or outpatient units in rehabilitation practice. With various neurological conditions locally and internationally.
Methods
Eligibility criteria
Data were collected depending on the following inclusion criteria; population are adult with neurological impairment (stroke, TBI, SCI, MS, ALS, CP and N-TBI). Interventions included are assessment of sitting balance (objective and subjective). No comparison group has been chosen. Outcomes are psychometrics properties. Our review focuses on English language only (Table 1). Articles should be published between 2009–2019. Exclusion criteria are any assessment that measures the standing/walking ability or has items for that, and studies that include pediatric or adolescent or both. Pediatric or adolescent population have been excluded due to the primary investigator’s experience (WA), which was with adult only with different neurological conditions.
PICO components of the review.
Information sources
Studies included in this review were identified through 4 databases; PubMed, Web of Science, Ovid Medline and Cochrane. Other sources have been screened in order to find eligible studies. Our review focuses on English language only.
Search
We used the following keywords in order to find eligible studies: Adult with neurological impairment or stroke or spinal cord injury or SCI or multiple sclerosis or MS or traumatic brain injury or TBI or brain injury or BI or non-traumatic brain injury or N-TBI or Parkinson disease or brain tumours or central nervous system infection or cerebellar disease or Malformations and Developmental Anomalies or Neurodegenerative disease or Encephalopathies or Peripheral Neuropathies or myopathies or Neuromuscular Disorders and Assessment of sitting balance or evaluation of sitting balance or setting balance scale or measurement of sitting balance or dynamic sitting balance or static setting balance and Validity or reliability. The first run was on 28/9/2018 with a total of 977 articles and 42 duplicates. This was followed by another run on 13/9/2019 with 197 studies in total with no duplicates.
Study selection
For abstract screening stage, one reviewer (WA) screened all studies after removing duplicates. Another reviewer (HA) screened 5% of studies. Any disagreement was solved by discussion. Full text screening stage has been made independently by both reviewers until an agreement on study selection has been made.
Data collection process
After looking at examples of data extraction forms, we designed our form to be fitted with the review aim. One reviewer (WA) extracted the data and another reviewer (HA) checked the process.
Data items
Data was extracted on the following elements: condition, assessment, number of participants and validity and reliability elements (Cronbach alpha and Kappa if reported) and quality of evidence percentage.
Risk of bias in individual studies
Two reviewers (WA and HA) independently assessed the risk of bias. We used the quality assessment tool for reviewing studies with diverse designs (QATSDD).4 It is a tool that assesses studies of quantitative and qualitative design, using 16 criteria with 14 of the 16 for quantitative and qualitative and 2 for mixed-method studies. Each criterion has a 0-3 scale with 0 being not mentioned at all and 3 being complete illustration. An independent percentage has been calculated. The average percentage has been calculated and confirmed as the QATSDD percentage on quality of evidence. Any disagreement was solved until consensus has been reached.
Results
Study selection
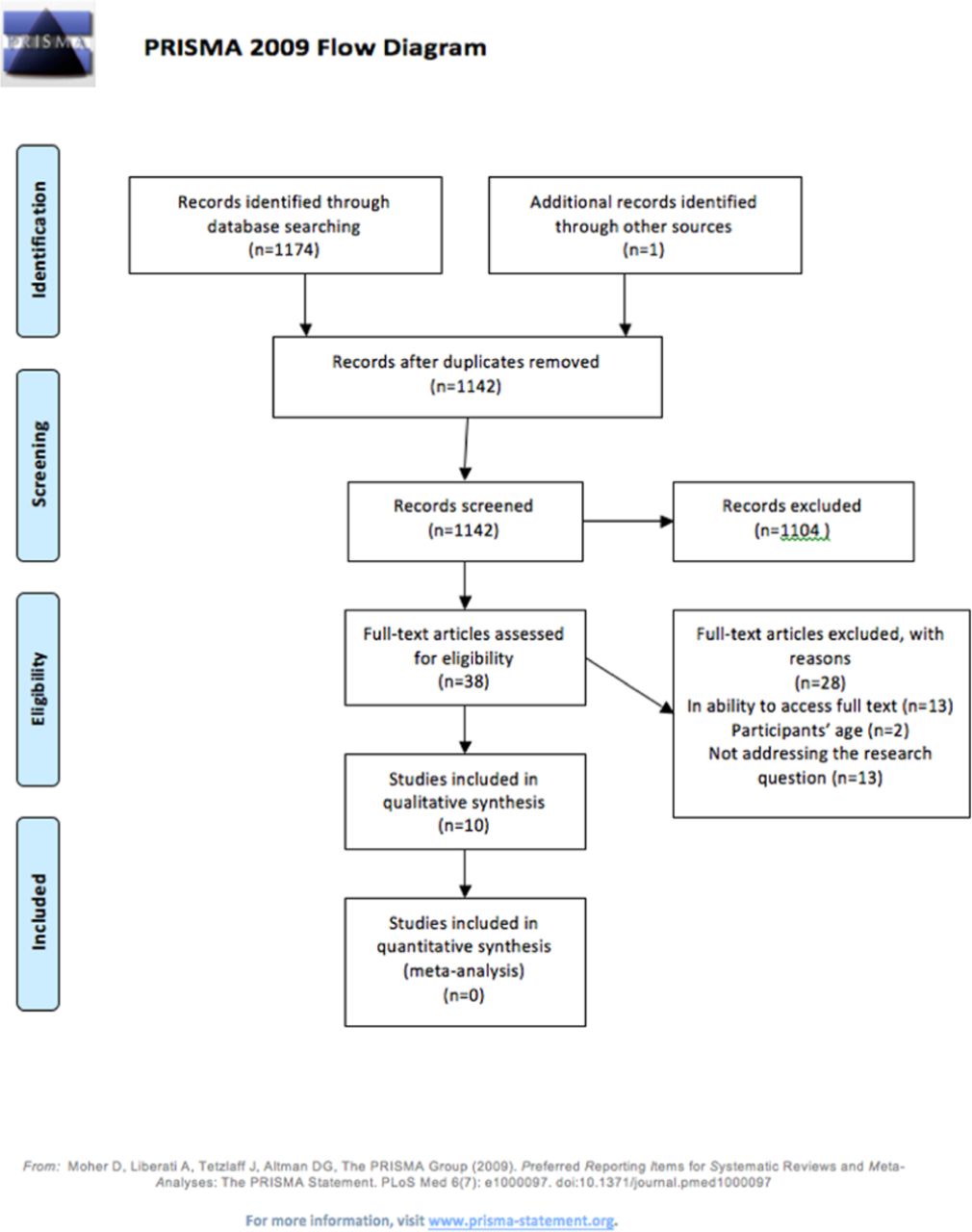
At first, we found 1175 records, then 1104 records were excluded, exclusion reasons were according to the inclusion and exclusion criteria set in the methodology section. Initially, 38 articles were eligible for full-text screening and among those, 28 were excluded as well according to the following reasons: 13 with no access, 6 had components other than sitting, such as walking or standing, 3 participants’ age, 2 inclusion of normal subjects, 4 assess sensory deficit rather than sitting components. Eventually, 10 out of the 38 were included in our review including 464 patients (Figure 1). Percentage of agreement was, abstract screening stage 82%, full-text screening 90% and any disagreement was resolved with discussion.
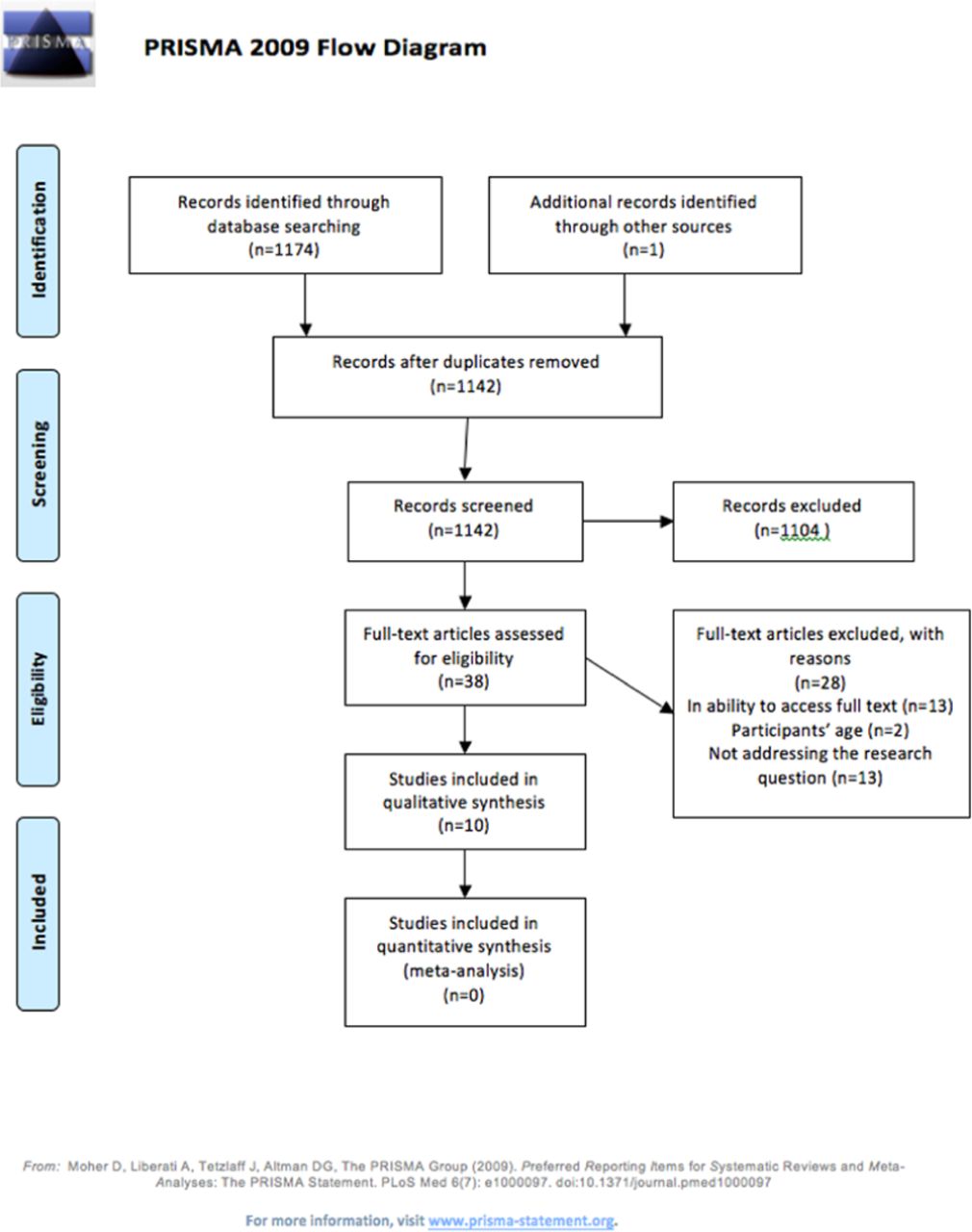
flow diagram of the process of choosing studies.
Summary of included studies
Six assessments have been found for spinal cord injury patients divided as the following; Motor Assessment Scale (MAS), item 3 ‘balanced sitting’ and Sitting balance score SBS,5 Brazilian version in Portuguese of the Thoracic-Lumbar Control Scale,6 Clinical trunk control test,7 Hand-Held Dynamometry in Individuals with Spinal Cord Injury,8 Dynamic sitting balance tests: Limits of stability. Dynamic sitting balance tests: sequential weight shifting9 and Sitting balance measure.10 Also, 3 assessments have been found for stroke patients; The Italian version of the Trunk Impairment Scale,11 Trunk Impairment Scale Norwegian version modified TIS-NV12 and Function in Sitting Test.13 Additionally, an assessment has been found for multiple sclerosis Function in sitting test (Table 2).14
Studies included in the review based on the condition.
It seems that clinical trunk control test has been reported as the highest percentage according to the QATSDD4 for SCI patients 89.58%. It is also reported with 177 sample size which is the highest sample size among all 10 articles included in this review. Alpha coefficient had a value of 0.979 indicating high internal consistency. The second assessment for SCI patients was Brazilian version in Portuguese of the Thoracic-Lumbar Control Scale. It has quality percentage of 88.58% according to the QATSDD.4 It included a sample size of 22 and its internal consistency was 0.934 indicating high internal consistency.
For stroke patients, Trunk Impairment Scale Norwegian version modified (TIS-NV) has been reported as the highest percentage according to the QATSDD4 in this group. Value was 88.09% including 50 sample size, Alpha coefficient had a value of 0.85 indicating good internal consistency. The second assessment for stroke patients was the Function in Sitting Test value was 83.33% including 31 patients, Alpha coefficient had a value of 0.98, indicating high internal consistency.
Although multiple sclerosis has reported one assessment (Function in sitting test),14 however it reported a high percentage 80.95% according to the QATSDD4 with a sample size of 20 patients, alpha coefficient had a value of 0.91, indicating high internal consistency.
One assessment (Function in Sitting Test) showed promising potential being implemented with both stroke13 and multiple sclerosis,14 Cronbach’s alpha, α were 0.91 and 0.98 indicating high internal consistency. It was used with SCI patients however no access was available to include this study in this review (Table 3).16
Studies characteristics (neurological condition, citation, measured aspects, participants, reliability elements and study quality percentage).
Study characteristics
Ten studies were eligible for inclusion in our review with a total number of 464 patients. Conditions can be divided as follows: 6 for spinal cord injury (based on 322 patients), 3 for stroke patients (based on 122 patients) and one article for multiple sclerosis (based on 20 patients). As a result, among 10 articles, 7 reported their Cronbach alpha found in the articles. The values varied from 0.85 to 0.98, which is good to excellent according to (Table 3).15
Risk of bias within studies
We used the Quality Assessment Tool for Reviewing Studies with Diverse Designs approach (QATSDD).4 Two reviewers (WA and HA) independently assessed the risk of bias. Average percentage between the 2 reviewers on quality of evidence was between 59.52-89.58%. Any disagreement was solved until consensus has been reached. Table 4 shows the average percentage given by both reviewers WA and HA.
Average percentage given by both reviewers WA and HA using The Quality Assessment Tool for Reviewing Studies with Diverse Designs approach.
Discussion
Summary of evidence
The intention of this review was to provide a variety and up to date assessments for the clinicians in everyday practice for multiple neurological conditions.
This review showed several studies that examined spinal cord injury and stroke as well as one study for multiple sclerosis. An assessment (Function in Sitting Test) showed promising potential being implemented with both stroke13 and multiple sclerosis14 Cronbach’s alpha, α were 0.91 and 0.98 indicating high internal consistency. Other advantages of this assessment were: its items were very simple and easy to be used by clinicians. In addition, it is available online with educational videos as well. Also, it was implemented for individuals with spinal cord injury, but no access was available.16
On the other hand, this review has shown that some cases such as brain injury showed lack of evidence. As a task, sitting is hard to be tested in patients with cognitive difficulties due to several complex demands. This could explain why there is no available evidence for this group, though it was demonstrated that stroke being a cortical lesion had three deferent studies in this review,11⇓–13 Moreover, there is a rich evidence with spinal cord injury subjects. Of these, the use of various objective assessments such as hand-held dynamometry8 and sitting platform,9 with 4 different objective assessments.5⇓–7,10 However, multiple sclerosis patients were assessed using function in sitting test14 which was validated in stroke patients too.13 Among the 10 included articles, 7 reported their Cronbach alpha found in the articles. The values varied from 0.85 to 0.98, which is good to excellent.
When it comes to the use of these assessments locally in Saudi Arabia for local patients, the conclusion would be different. It seems that these assessments need to be translated and adapted for local use. This would help in avoiding any challenges that might affect therapy provided to the patients.
Limitations
The current review was limited by the access provided by the Saudi Digital Library (SDL) and King Abdulaziz City for Science and Technology (KACST). Thirteen studies in this review have been excluded as there was no access to the full text. A recommendation for both SDL and KACST is to provide an access to more journals in order to facilitate high quality research in Saudi Arabia. There was an intention to register this systematic review in PROSPERO (International prospective register of systematic reviews).17 However, the website has been stated that “As PROSPERO is funded by the National Institute of Health Research (NIHR) registrations from the U.K are prioritised”. Thus, a fund from Saudi Arabia is recommended in order to have a collaboration with PROSPERO website to prioritise systematic review registration from Saudi Arabia.
Conclusions
This review indicates an extension of what was done by previous systematic reviews with neurological conditions. It seems that Function in Sitting Test is the most frequent assessment in this review with multiple neurological conditions (stroke, MS and SCI) with high internal consistency and high quality studies according to available data. However, this review showed that there is an absence of evidence for individuals with brain injury. Further work needs to be done to address such groups of patients to extend the choices that clinicians can use in rehabilitation sittings. Also, translating and adapting assessments found are recommended for researchers to draw a clear conclusion for each culture.
Copyright
Whenever a manuscript contains material (tables, figures, etc.) which is protected by copyright (previously published), it is the obligation of the author to obtain written permission from the holder of the copyright (usually the publisher) to reproduce the material in Saudi Medical Journal. This also applies if the material is the authors own work. Please submit copies of the material from the source in which it was first published.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received December 21, 2019.
- Accepted April 8, 2020.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.