


Abstract
Objectives: To perform screening of dysphagia in Montenegrin multiple sclerosis (MS) patients. Dysphagia is often neglected problem in patients with MS.
Methods: We included 104 patients with relapsing-remitting MS who completed 3 questionnaires: dysphagia in multiple sclerosis (DYMUS), eating assessment tool-10 (EAT-10) and swallowing disturbance questionnaire (SDQ). Our study was performed in the clinic for neurology of the Clinical Center of Montenegro (Podgorica, Montenegro) and Polyclinic Neuron (Bijelo Polje, Montenegro) between November 2020 and December 2020.
Results: Self-reported prevalence of this symptom in our group was simmilar to previously reported results. We did not find correlation between DYMUS and expanded disability status scale (EDSS), as it was reported before. Time spent from disease onset to diagnosis is strongly correlated with reported SDQ results. The population of dysphagia-patients is statistically significantly older compared to the non-dysphagia patients, and statistically higher mean values in this population of our subjects were proven on all 3 questionnaires used.
Conclusion: The importance of this issue is not just because it warns of potientially malnutrion in MS patients, but also important factor in therapy choosing algorithm in the era of orally used immunomodulatory drugs.
Multiple sclerosis (MS) is as a chronic neurological disease that can affect the swallowing process owing to demyelination of the myelin sheath.1 Dysphagia in MS occurs as a combination of damages in several structures, such as the corticobulbar nerve tract, cerebellum, brainstem, and lower cranial nerves.2 Mild swallowing problems are frequently overlooked by both physicians and patients among a broad array of neurological symptoms of MS. However, considering the possible complications of dysphagia (aspiration pneumonia, dehydration, malnutrition, and reduced quality of life), it is very important to pay close attention to this issue.3 A great number of researchers are working on screening tools for early diagnosis and identification of MS patients who are at risk of dysphagia, because earlier detection has the potential to lower costs and improve outcomes.4 The creation of multidisciplinary teams (ENT specialists, gastroenterologists, and neurologists) for treatment and monitoring of dysphagia leads to earlier identification of this problem in MS patients. The significance of dysphagia for patients with MS is even greater today, when an increasing number of orally used immunomodulatory drugs is appearing on the market.
According to one of the most recent meta-analyses on the prevalence of dysphagia in MS patients, the overall prevalence rate of dysphagia in MS patients was 43.33%.5 According to a Brazilian research, the progressive forms of MS (primary progressive and secondary progressive) were more frequently linked to severe dysphagia, whereas the relapsing-remitting form (RRMS) was linked to mild and moderate dysphagia.6 The disability level of expanded disability status scale (EDSS) and the length of the disease were revealed to be important predictors of dysphagia in MS patients by an Iranian group of investigators.7
Despite the availability of a swallowing rehabilitation program that can improve the swallowing function of MS patients with dysphagia, in cases of increasing dysphagia, a gastrostomy tube may be the only option for optimal feeding.8 According to a newly published finding, the median period from MS diagnosis to gastrostomy was 17.8 years, and the median survival duration following gastrostomy was 21.73 months (based on a sample size of 53 MS patients).9
It is believed that there are roughly 650 MS patients in Montenegro, a country with a population of approximately 650,000 people, with approximately 400 of them having RRMS.
The aim of our study was to perform screening of dysphagia in RRMS patients in Montenegro, as well as to correlate characteristics of dysphagia with demographic and clinical features of study group.
Methods
Our cross-sectional study included 104 patients with RRMS who underwent an examination in the clinic for neurology of the Clinical Center of Montenegro (Podgorica, Montenegro) and Polyclinic Neuron (Bijelo Polje, Montenegro) from November 2020 to December 2020. Approval was obtained from the ethics committee of the Clinical Centre of Montenegro (No: 03/01-23457/1). The procedures used in this study were according to the principles of Helsinki Declaration. Inclusion criteria for participation in our study were diagnosis of RRMS and age ≥18. Exclusion criteria were diagnosis of primary progressive multiple sclerosis (PPMS), secondary progressive multiple sclerosis (SPMS) and other neurological diseases as well as age <18. After getting acquainted with the goals of the research and the methodology, all patients signed an informed consent form before joining the research.
Questionnaires
We applied the dysphagia in multiple sclerosis (DYMUS), eating assessment tool-10 (EAT-10), and swallowing disturbance questionnaire (SDQ) questionnaires to conduct our study. The presence or absence of relevant symptoms was determined using the DYMUS questionnaire, which consisted of 10 yes/no questions.10 A score ≥3 was considered abnormal. Patients were asked to reply to all of the statements in the EAT-10 questionnaire and to rate the severity of their difficulties on a scale of 0-4 (where 0 indicated no problems and 4 indicated severe problems).11 An EAT-10 score ≥3 was considered to be indicative of possible dysphagia. The SDQ consisted of 15 questions. The first 14 questions were scored on a grade scale of 0-3 (where 0 indicated no disorders and 3 indicated severe disorders), and the last question was a yes/no question (scored 0.5 points if the response was “no” and 2.5 points if the response was “yes”). An overall score ≥12.5 points was considered abnormal.12
Statistical analysis
Data was analyzed using the Statistical Package for Social Sciences (SPSS) software version 23.0 (IBM Corp., Armonk, NY, USA). We used the chi-square test for homogeneity in order to evaluate whether there was a statistically significant difference in the distributions of different populations of respondents. We used a 5% significance level, namely, we will reject the hypothesis that the populations are homogenous if the p-value is <0.05. Additionally, we calculated the Pearson’s correlation coefficients and used linear regression to examine whether there was a statistically significant correlation between various parameters evaluated in the research.
Results
After excluding 2 patients from the study owing to an incomplete questionnaire, our sample included 102 patients. Of these 102 patients, 24 (23.5%) were male patients and 78 (76.5%) were female patients, and the mean age was 38.2±9.7 years. The mean duration of illness in our subjects was 6.3±5.5 years, the mean time to diagnosis was 2.5±3.8 years, and the mean period from diagnosis to the start of disease-modifying therapy (DMT) was 2.5±3.3 years. At the time of examination, the mean EDSS score was 2.9±1.2. Regarding the number of relapses, the largest number of respondents had one (32 respondents, 31.4%) and 2 (25 respondents, 24.5%) relapses in the course of the disease, 14 (13.7%) respondents had 3 relapses, 15 (14.7%) had 4 relapses by the time of the study, and 16 (15.7%) had 5 or more relapses. Concerning the DM that patients used, most patients (72 patients, 70.6%) were on first-line drugs, and 8 (7.8%) patients were in one of the following 3 groups: patients switched to second-line drugs after first-line drugs; patients on second-line drugs as a first therapy choice, and patients not using DMT. We had one (1.0%) patient using only third-line therapy and 5 (4.9%) patients using third-line drugs after using first- and second-line drugs. The mean duration of therapy was 3.8±5.0 years.
Table 1 shows the prevalence of dysphagia in our subjects in relation to each questionnaire used. A detailed overview of the answers to all questions from the 3 questionnaires is provided in Tables 2, 3 & 4.
- The prevalence of dysphagia in study subjects according to questionnaire (n=102).
- A detailed overview of responses of patients to DYMUS questionnaire.
- A detailed overview of responses of patients to EAT-10 questionnaire.
- A detailed overview of responses of patients to SDQ questionnaire.
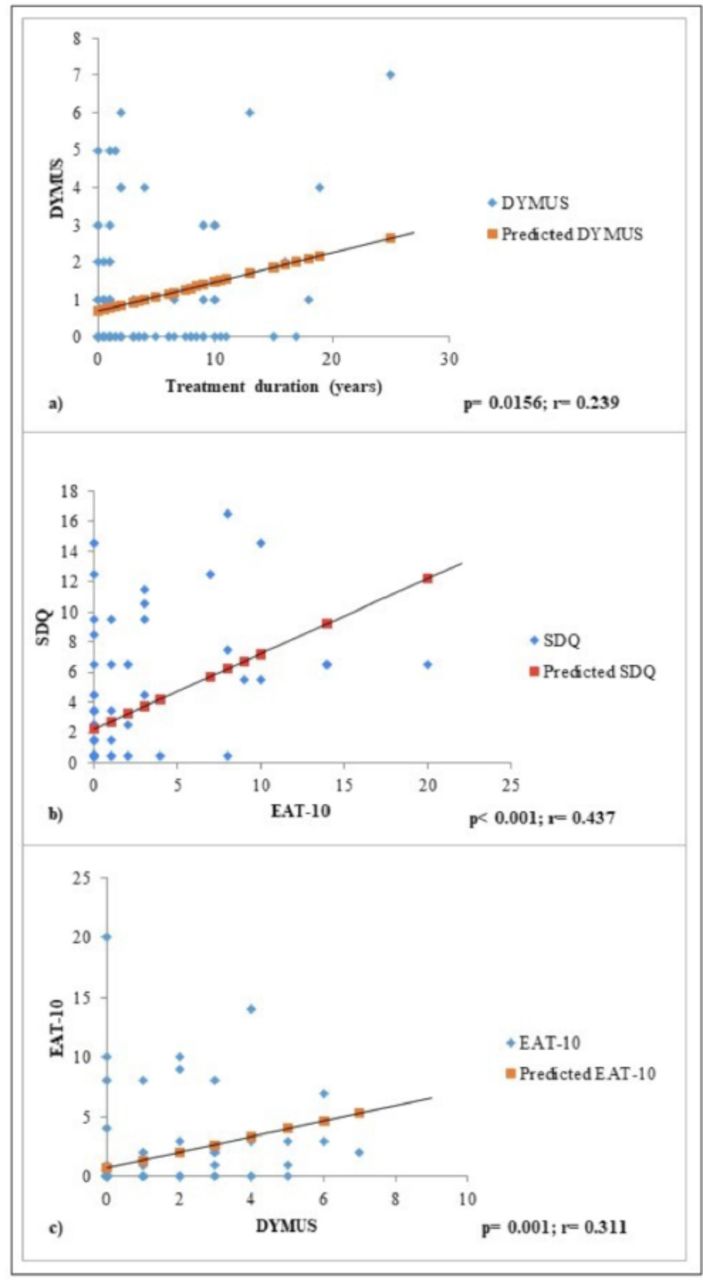
Table 5 shows the clinical and demographic characteristics of our patients in relation to the 3 questionnaires used in our study. In terms of statistical correlations, we found 3 significant correlations, as shown in Figure 1.
- Correlation between EAT-10, DYMUS and SDQ with demographic and clinical characteristics of respondents.
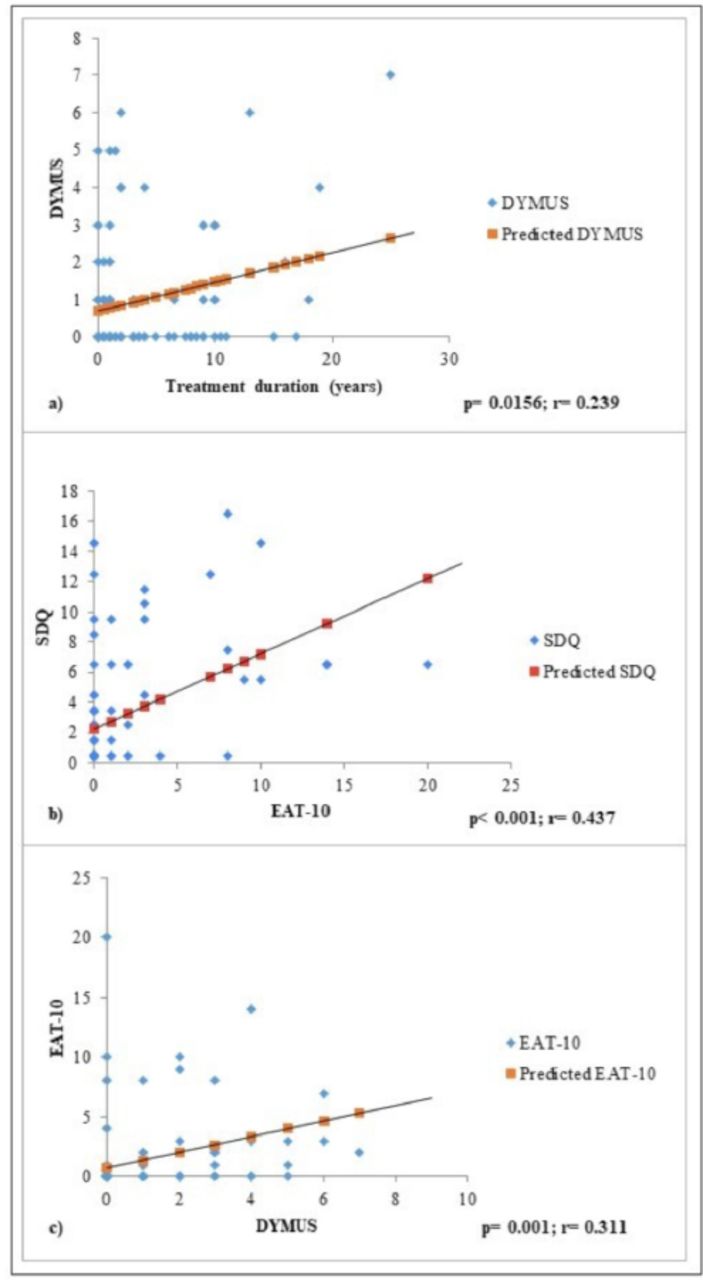
- Statistically relevant correlations.
In order to compare demographic and clinical characteristics in our subjects, they were divided into the following 2 groups: dysphagia patients (abnormal results in at least one of the applied questionnaires) and non-dysphagia patients (normal results in all 3 applied questionnaires). The obtained results are shown in Table 6.
- Comparision of demographic and clinical characteristics of dysphagia- and non-dysphagia patients.
Discussion
The group of respondents included in our study made up approximately 25% of the total number of RRMS patients in Montenegro, and their gender distribution corresponded to the recent knowledge of MS gender distribution (female-to-male ratio of 2.3-3.5:1).13
The prevalence of dysphagia according to the questionnaires used in our research was similar to that reported in a recent published paper by Milewska et al.14 It was surprising that almost 40% of patients with RRMS in Montenegro reported dysphagia in the DYMUS questionnaire as a symptom of the disease. However, this is confirmed by previous research emphasizing that dysphagia is a present but often neglected problem in MS patients. It is important to emphasize that DYMUS is the preferred method of dysphagia screening in clinical practice.15 According to the DYMUS questionnaire, 16.67% of our respondents had dysphagia, indicating that every 7th respondent was a MS patient with severe dysphagia. This result is especially important when considering the fact that the DYMUS questionnaire can be a useful clinical tool for red flagging patients who should undergo objective testing and should be referred to a otorhinolaryngologist.16
Looking more closely, 18 (17.65%) patients reported weight loss as a symptom, as part of the DYMUS questionnaire. In our opinion, this number is too large, and it might be a reflection of current stressful events related to COVID-19, because MS patients are, according to our study, concern about the future status of the disease in the current epidemic era.17 The large number of patients with weight loss might also be associated with the season in which the examination was performed (summer). Interestingly, almost an identical percentage of respondents answered in the affirmative to this question during the validation of the Portuguese DYMUS questionnaire.18
Certainly, the fact that every 10th respondent (9.80%) stated that he/she has problems swallowing solid food should not be overlooked. According to the SDQ, the frequency of this problem in most respondents was once a month or less often. From the obtained results, we noted that once a month, 19.61% of respondents experienced food residues in the mouth, in the cheeks, under the tongue, or stuck to the nose on eating or drinking. These data suggest the need to expand routine anamnestic issues to regular patient check-ups.
We did not find a correlation between the DYMUS questionnaire findings and EDSS, as was reported in other studies.10,19 Additionally, we did not find a correlation between the EAT-10 questionnaire findings and EDSS or between the SDQ findings and EDSS. Our study confirmed the previously reported strong correlation between the DYMUS and EAT-10 questionnaire findings and showed a strong correlation between the EAT-10 questionnaire and SDQ findings (p<0.001, r=0.437).20
Our results showed a correlation of the age of our respondents with the DYMUS questionnaire findings, but not with the findings of the other 2 questionnaires used. Elderly patients are expected to report symptoms of dysphagia to a greater extent.21 Additionally, in our results, time spent from disease onset to diagnosis of MS was strongly correlated with the SDQ findings. This confirms that early diagnosis of MS is a prerequisite for achieving favorable therapeutic effects in MS patients. Treatment duration was correlated with the SDQ findings. It should be noted that a close correlation was present between treatment duration and the DYMUS questionnaire findings, as shown in Figure 1 (p=0.0156, r=0.239).
As mentioned earlier, Table 6 shows the demographic and clinical characteristics of patients who had an abnormal result on at least one of the questionnaires (labeled as dysphagia patients) and those who had a normal result on all 3 questionnaires (labeled as non-dysphagia patients). The population of dysphagia patients was significantly older compared with the population of non-dysphagia patients, and in this population, statistically higher mean values were obtained in all 3 questionnaires used. Our study did not identify a statistically significant difference in other clinical features, such as EDSS and mean disease duration, which is consistent with findings from previous studies.5
Limitations
Our study had a limitation in that it did not include individuals who were in remission or who did not have regular check-ups. Another limitation was that the questionnaires took approximately 20 minutes to complete, and fatigue may have had an impact on patient responses. Moreover, cognitive changes are present in patients with MS, and they might have had some influence on patient responses.
In conclusion, our results suggest that the prevalence of dysphagia in RRMS patients in Montenegro is high, and since it is often disregarded by both patients and physicians, it is necessary to pay additional attention to this problem. Any of the questionnaires used in our study can be incorporated in a routine follow-up as an initial assessment. Patients with scores indicating dysphagia may then be prompted to undergo further evaluation. The teamwork of neurologists, gastroenterologists, and otorhinolaryngologists would improve the process of diagnosing, treating, and monitoring dysphagia in RRMS patients in Montenegro. Further work foreseen includes an extensive study of dysphagia problems in a larger number of MS patients, as well as on other phenotypes of MS (progressive forms).
Ethical Consent
All manuscripts reporting the results of experimental investigations involving human subjects should include a statement confirming that informed consent was obtained from each subject or subject’s guardian, after receiving approval of the experimental protocol by a local human ethics committee, or institutional review board. When reporting experiments on animals, authors should indicate whether the institutional and national guide for the care and use of laboratory animals was followed.
Acknowledgment
The authors gratefully acknowledge Wordvice (https://wordvice.com/) for English Language Editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 11, 2021.
- Accepted July 11, 2021.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.