


Abstract
Lumboperitoneal (LP) shunt is considered as a unique procedure in neurosurgical practice. The over drainage of Cerebrospinal fluid (CSF) is considered a usual side effect of the procedure that usually manifests in the form of subdural collection, headache, or nausea and vomiting. However, cranial nerve palsy, particularly abducens nerve palsy, is a rare manifestation of CSF over drainage. We describe our experience with a patient that has developed bilateral sixth nerve palsy followed by LP shunt insertion, with resolution of the symptoms upon removal of the shunt. This shades the light on a rare but significant complication related to Lumboperitoneal (LP) shunt insertion that necessitate the modification in the hardware of valve or insertion technique to decrease the risk of CSF over the drainage.
Lumboperitoneal (LP) shunt, in neurosurgical practice, is a unique procedure.1 Cerebrospinal fluid (CSF) over drainage is an often-encountered side effect of this procedure along with shunt failure.1 Cerebrospinal fluid over drainage can manifest as headache, subdural collection, subdural hematoma, or epidural hematoma.2 Abducens palsy is a rare complication of various CSF diversion procedures.3 Sporadic case reports, case series, and systematic reviews have discussed cases of abducens palsy following diagnostic LP shunt, lumbar drain, spinal/epidural block and ventriculoperitoneal (VP) shunt.2 However, there has been no evidence of any such case in the past literature about bilateral sixth cranial nerve palsy following by LP shunt. We describe our experience with the recognition, management, and follow-up of a patient having bilateral sixth nerve palsy following by LP shunt insertion.2,4 These shades the light on a rare but significant complication related to Lumboperitoneal (LP) shunt insertion.
Case Report
Patient information and clinical findings
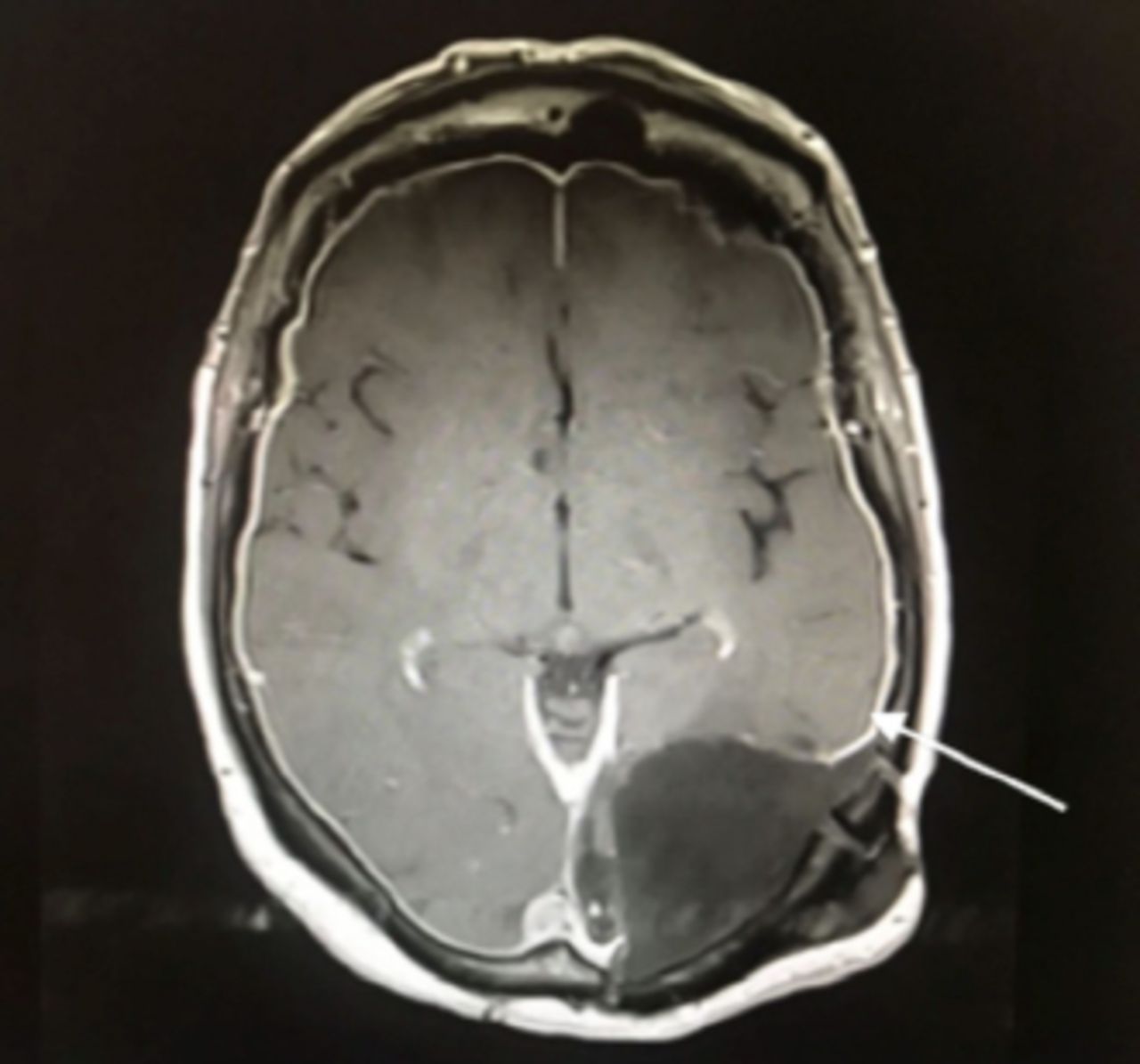
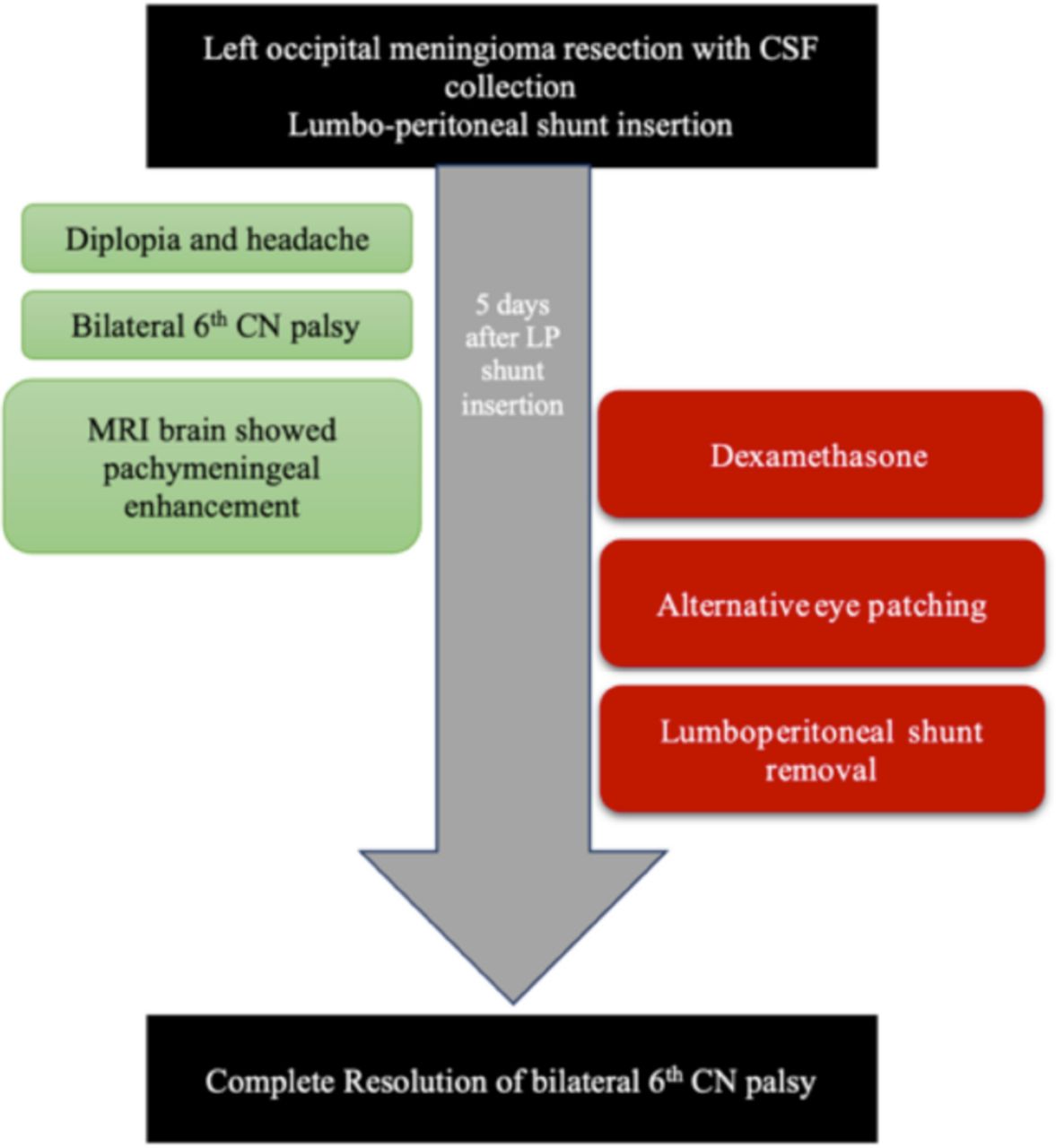
A 62-year-old female who previously underwent two-stage left occipital meningioma resection developed surgical site subgaleal CSF collection that failed to resolve with conservative measures. After discussing various options and their risks and benefits with the patient, the decision was made for the insertion of a valveless LP shunt. The patient underwent LP shunt insertion (StrataNSC LP Medtronic valve). Through the mini-laparotomy approach, the peritoneal cavity was considered for insertion by distal end. In the fifth day postoperatively, the patient started to have a mild headache and diplopia. Two days thereafter, the symptoms worsened and became cumbersome. The patient presented to our emergency department on the seventh day postoperatively. Examination revealed bilateral abducent cranial nerve palsy, with the left side being more severely affected than the right, with interval improvement in the subgaleal collection (Figure 1).

- Left lateral gaze, shows left abducens palsy.
Diagnostic assessment
The brain’s Magnetic resonance imaging in contrast (Figure 2) showed diffuse pachymeningeal enhancement.
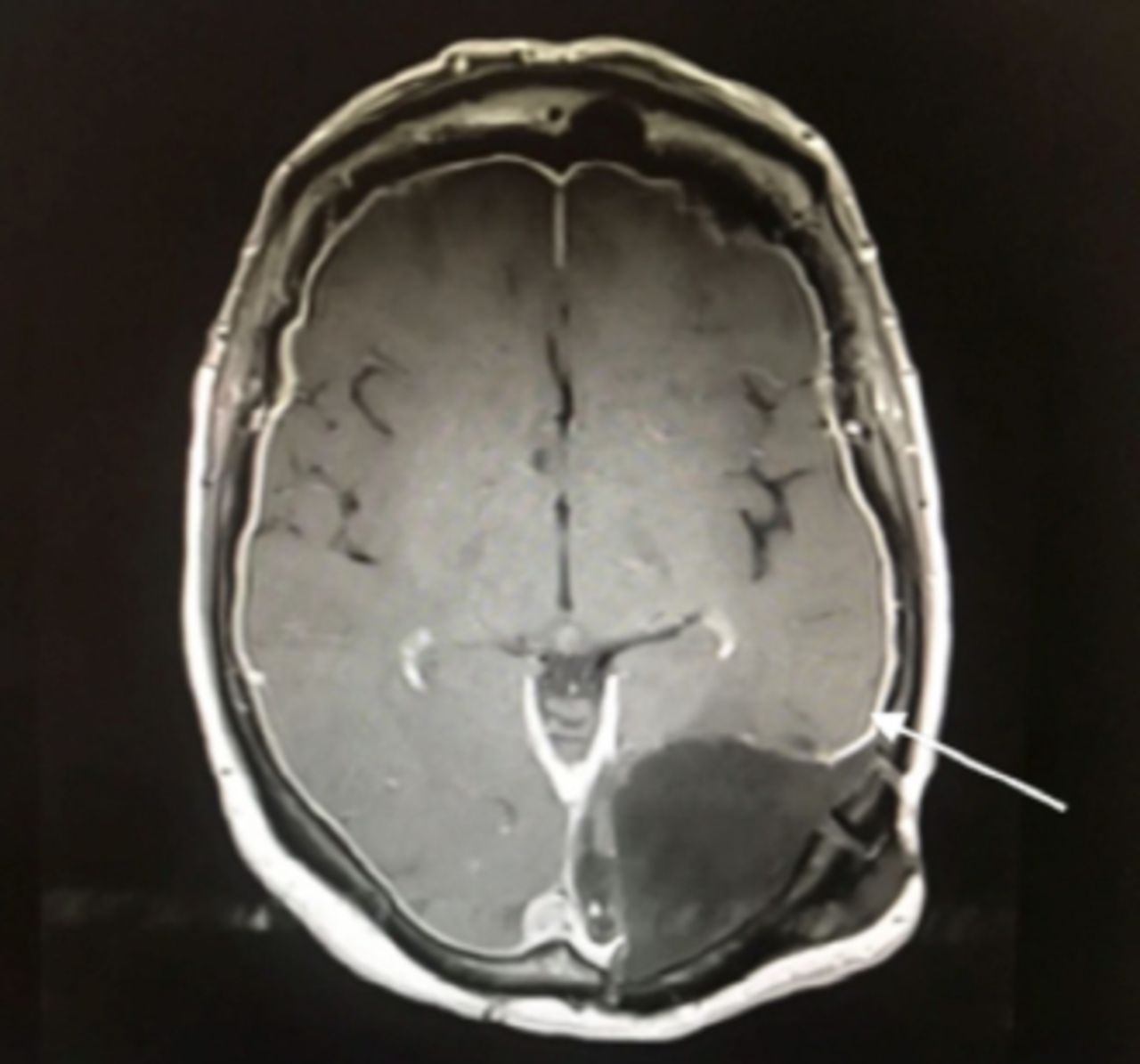
- Brain MRI, T1 with contrast, showing diffuse pachymeningeal enhancement, indicating CSF over drainage.
Therapeutic intervention
The patient was initially treated with intravenous dexamethasone therapy by providing a dose of 4 mg for each 6 hours and alternating eye-patching for every 2 hours. Ultimately, it led towards the removal of the LP shunt.
Follow-up and outcome
A clinic visit after 3 months showed complete resolution of sixth nerve palsy with no progression in the size of subgaleal collection (Figure 3). Clinical findings, diagnostic assessment, treatment modalities and outcome are shown in timeline diagram (Figure 4).

- Right lateral gaze, shows partial right abducens palsy.
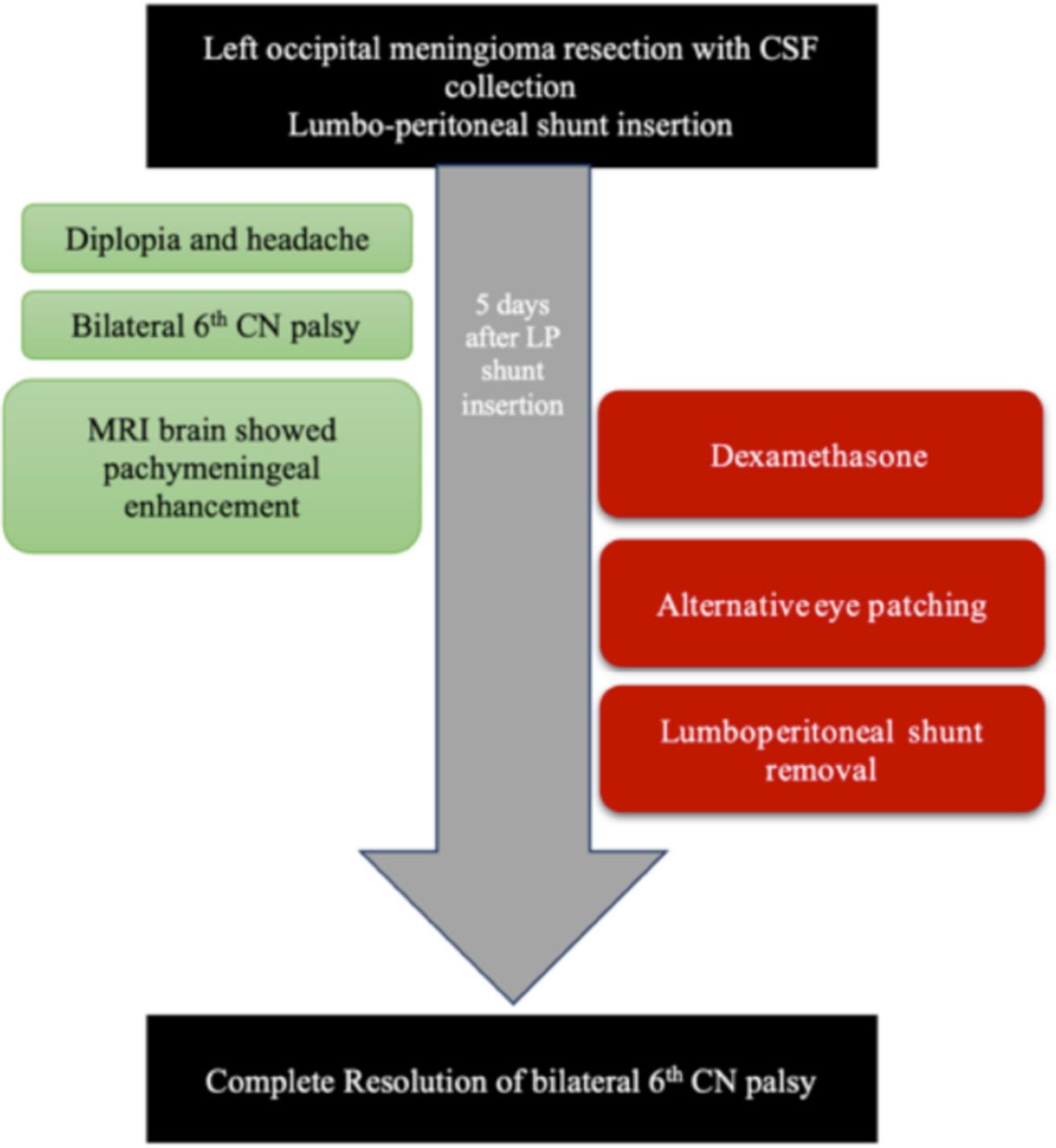
- Time table of the clinical condition
Discussion
The LP shunt is being considered as a safe and effective CSF diversion strategy, even though the rate of complications of this procedure can reach up to 20.5%.3 These include complications generally associated with CSF diversion procedures, such as migration or fracture of the catheter, malfunction requiring revision and infection.6 Complications specifically related to LP shunt include nerve root irritation resulting in radicular pain, subarachnoid hemorrhage, epidural hematoma, tonsillar herniation, acute subdural hematoma and spinal deformities.2
Clinical presentation
Lumbar CSF drainage can reduce the volume of CSF with a drop of intracranial pressure (ICP); this commonly presents with a chronic headache and may sometimes result in a subdural collection.1 Cranial nerve palsy following different CSF diversion procedures or dural puncture procedures (diagnostic lumbar puncture, lumbar drain, spinal/epidural block, lumbar myelography, VP shunt, and intrathecal drug delivery) is considered a rare entity as described in the literature.2,3,4,9 Quincke was the first to describe transient sixth nerve palsy following a lumbar puncture in the early 1900s4. Li et al3 conducted a retrospective review of five cases in their institution along with a systemized literature review from the period of 1950 to 2015 for all cases diagnosed with cranial nerve palsy followed by the CSF diversion or dural puncture processes, identifying a total of 53 patients. The authors described the involvement of several cranial nerves (CNs) including CN II, CN III, CN IV, CN V, CN VI, CN VII and CN VIII. The sixth cranial nerve was most frequently involved (44 cases, 83%). Headache, particularly of the postural type, was reported as the most common warning symptom preceding the development of cranial nerve palsy, consistent with our patient’s clinical condition.3,4 Ninety-Six percent of patients in the review achieved complete resolution after the application of a variety of treatment strategies.3,5
Pathophysiology
The CSF drainage in the valveless LP shunt is uncontrolled and associated with intracranial hypotension.9,10 Specifically, the abducens nerve is considered as more sensitive as compared to other cranial nerves and this shows the attribution for long intracranial course;9 however, anatomical studies have shown the longest intracranial course in trochlear nerve that is insensitive towards ICP based injuries.10 The increased vulnerability of the abducens nerves depends on the local anatomic factors in which the severe angulation in the point of entry at petroclival dural, which is an entrance to Dorello’s canal, is considered as the most susceptible area because there is a chance that nerves will be tethered within the canal.10 The CSF hypotension causes a high risk of traction injury at the fixation point of the nerves due to acute angulation with the descent of brainstem.10 The ischemic changes by vasospasm and vessel compression or direct mechanical stretch injury or the combination of both results in nerve palsy.7,9
Management and outcome
Clamping of lumbar drain, hydration and bed rest following lumbar puncture, and application of an epidural blood patch are different strategies used for the management of cranial nerve palsy following CSF diversion procedures.3 Sixth cranial nerve palsy following CSF hypotension is reversible in most cases if managed early before irreversible damage occurs.10 Recently, use of programmable valve is taking the lead in prevention of complications related to CSF over drainage.1 The correlation between risk of cranial nerve deficit and use of programmable LP valve needs further investigation. Cranial nerve palsy following LP shunt may be underreported. This case illustrates the risks associated with valveless LP shunt and underscores the importance of early intervention to prevent permanent damage.
In conclusion, the use of programmable LP shunt may be safer than valveless LP shunt and avoids the risk of CSF over-drainage and its complications.1 Abducens and other cranial nerve palsies can also be reversible in most cases if CSF over-drainage is managed with early intervention.
Acknowledgement
We would like to thank “Cambridge Proofreading LLC” English editing company, for language editing
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received December 17, 2021.
- Accepted April 19, 2022.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.