


Abstract
Objectives: To investigates the knowledge and attitudes toward epilepsy in Rabigh province in western Saudi Arabia.
Methods: A cross-sectional survey-based study was conducted from July to September 2020. Survey was distributed through the web to Rabigh province general population. Epilepsy awareness score (EAS) was estimated utilizing a generated questionnaire.
Results: The number of participants is 511. Most participants did not know what actions to take for an active seizure other than moving the person away from harm (87%). Participants who agreed that epilepsy was highly stigmatized represented 15%. Participants were refusing (27%) or undecided about their reaction (34%) if their child were to marry an epilepsy person (EP). The majority did not mind if their children socialized with EP. Some parents were anxious about having their children play or associated with EP. There are statistically significant associations between EAS and age (p=0.03), monthly income (p=0.03), having children (p=0.04).
Conclusion: The data found in this study was similar to other Saudi and global studies. Further efforts are needed to strengthen community awareness regarding epilepsy. Stigma in society affects those that are afflicted and has consequences on their loved ones as well. Therefore, supplementary educational campaigns are needed to normalize and create acceptance. Also, to increase awareness regarding first aid of epilepsy.
Globally, approximately 70 million (1-2%) people suffer from epilepsy, a neurological condition that predisposes the affected individual to have recurrent seizures.1 As defined by the International League Against Epilepsy (ILAE), a patient is required to have 2 unprovoked seizures at least 24 hours apart to be labeled as having the disease.2 Cryptogenic or idiopathic seizures account for approximately 50% of those with epilepsy while sociodemographic factors may play a role in prognosis and outcome.3,4 Although little is known regarding epilepsy prevalence in Saudi Arabia (SA), a study conducted in 2001 approximated the prevalence in the country to be 6.54 per 1000 population.5
Locally, the awareness and attitude regarding epilepsy across various major cities in different regions of SA showed that public knowledge regarding the condition was insufficient for the past several years.6,7 Rabigh province, is a province that growing and transforming into a more urbanized area. There are multiple main projects of SA in this province like King Abdullah Economic City, King Abdullah University for Science & Technology, Aramco (Arabian American Oil Company) refinery, and Petro-Rabigh plant which is one of the biggest and sophisticated plants in SA and the world.8 This study aims to assess the awareness and attitudes of a local population regarding epilepsy in the Western region of SA and to compare the results with previous studies.
Methods
A cross-sectional, population-based study conducted through an online survey disseminated amongst residents of the Saudi province of Rabigh from July to September 2020. The survey was spread via social media dedicated to Rabigh Province and the students in Rabigh King Abdulaziz University. The inclusion criteria are working in Rabigh province and age above 18 years old. We exclude persons with history of epilepsy and persons live outside Rabigh for more than 2 days per week. Ethical approval was obtained from the Research Ethics Committee of the Faculty of Medicine at King Abdulaziz University in Jeddah, Saudi Arabia and the guidelines outlined in the Declaration of Helsinki were followed.
Previous studies regarding epilepsy awareness in Saudi Arabia and specially in Rabigh province, in the last 5 years were searched in google scholar and PubMed using the keywords: Epilepsy, Awareness/Knowledge/Attitude, Saudi Arabia, and Rabigh.
The questionnaire consists of 4 sections: respondent demographics, epilepsy background, epilepsy knowledge, and attitude toward epilepsy. Demographics included information about gender, age group, nationality, marital status, level of education, monthly income, being diagnosed with epilepsy, family history of epilepsy, and occupation. Epilepsy background questions asked respondents whether they have ever read of convulsive seizures, seen or known anyone with or have had an active seizure, know what to do, or have received first aid training in the management of epilepsy. The epilepsy knowledge section consisted of a series of questions to assess the respondent’s level of comprehension regarding what to do during a seizure attack, the causes of epilepsy, treatment options, and abilities of those affected by the disease. The last portion of the questionnaire aimed to assess the attitude of the respondents towards epilepsy. The questions were generated from validated questionnaire of previous studies conducted in Saudi Arabia in 2019 and above.7,9–13
An epilepsy awareness score (EAS) was generated for each correct answer from the epilepsy knowledge portion of the questionnaire. Zero points were given for a wrong answer, “I don’t know”, or a blank. The score was out of 45 total questions.
The survey data used in this study are available upon request from the corresponding author. Statistical analysis was carried out using IBM SPSS Statistics Version 20. Pearson’s Correlation Coefficient is used to investigate the linear association between two continuous variables. Analysis of variance (ANOVA) and independent samples t-test were used to investigate the association between the means of the study variables as appropriate. The significance level was taken at <0.05 with a 95% confidence interval (CI).
Results
Demographic data
A total of 511 people volunteered to participate in the survey. 53% were male and 47% were female. The majority (51.5%) were between 30–55 years of age and approximately two thirds (60.9%) were married with a little more than half (54.6%) answering that they had children. Although the great majority (57.1%) held a bachelor’s degree, 44.4% had a monthly income less than 5000 Saudi Riyals and 22.4% were unemployed. Most of the participants live in Rabigh city (61.4%) and 23.7% came from another province, but currently live in Rabigh province. All the study participants denied personal history of epilepsy and 29.4% admitted to family history of epilepsy. Detailed demographic data is displayed in Table 1.
- Demographics.
Epilepsy background
Regarding participants’ epilepsy background, 90.6% claimed to have read about convulsive seizures and 56% responded they have seen an active seizure before. Only 171 of those who responded (33.5%) stated to know what to do if someone is seizing, however just 22.7% stated that they received first aid training regarding epilepsy management. Further information regarding respondent’s answers can be seen in Table 2.
- Participants’ background on epilepsy.
Epilepsy knowledge
Regarding first aid knowledge, during an active seizure, 87.3% of participants knew that it was correct to move a seizing person away from danger. However, almost one third (33.9%) were not sure whether to force the patient to take their medication, force a spoon or cloth in their mouth (31.1%), splash water on them (23.9%), and 62.6% answered incorrectly that they should hold or fix the seizing person, so they are unable to move.
Most participants (406/506) knew that epilepsy affects all ages, and 62% knew that it did not affect lifespan. However, participants were not sure if epilepsy has effects on sexual ability or pregnancy. The following symptoms were correctly recognized as symptoms of Epilepsy: convulsion or shaking (85.3%), loss of consciousness (75%), transient change of behavior (40.9%), period of amnesia (38%), and blank staring (46%). On the other hand, headache (37.2%) and hallucination (28%) were incorrectly recognized as symptoms of Epilepsy among some respondents, while 5.3% thought epilepsy was a form of insanity.
The cause of epilepsy was correctly identified as hereditary or genetic (60.7%) or a result of brain disorder or injury (77.3%). Incorrect answers included epilepsy being caused by mental disorders (32.4%), devil spirits (19.4%), blood disorders (4.7%), birth defects (3.4%), and contagious disease (1.2%).
Treatment options were correctly recognized as medical (95.7%) and surgical (32.6%) in some cases. However, some incorrectly felt there was a role for herbal treatment (24.9%), over the counter medications (34.4%), wet cupping (30.6%), spiritual healers (10.7%) and 9.1% believed that epilepsy is not treatable, with 3% believing that there is no need for any sort of treatment.
The majority (93.2%) recognized that people with epilepsy can be active members of society and although 93.6% recognized that the mental abilities of those with epilepsy are the same as those without epilepsy, only 61.7% thought they should be employed like those without epilepsy. Detailed questionnaire data regarding epilepsy knowledge can be found in Table 3.
- Participants’ knowledge about epilepsy and first aid of epilepsy.
Attitude toward epilepsy
Among participants, 84.6% replied that they would befriend someone with epilepsy, 75% would not object to having their children associated with a person with seizures at school, and 77.6% would not object to their children playing with a child known to have seizures. Regarding their children marrying someone with epilepsy, only 39.1% said they would not object, and 2% replied that they would lie about having a family member with epilepsy. Table 4 shows detailed respondent answers on attitude toward epilepsy.
- Participants’ attitude toward epilepsy.
Epilepsy awareness score
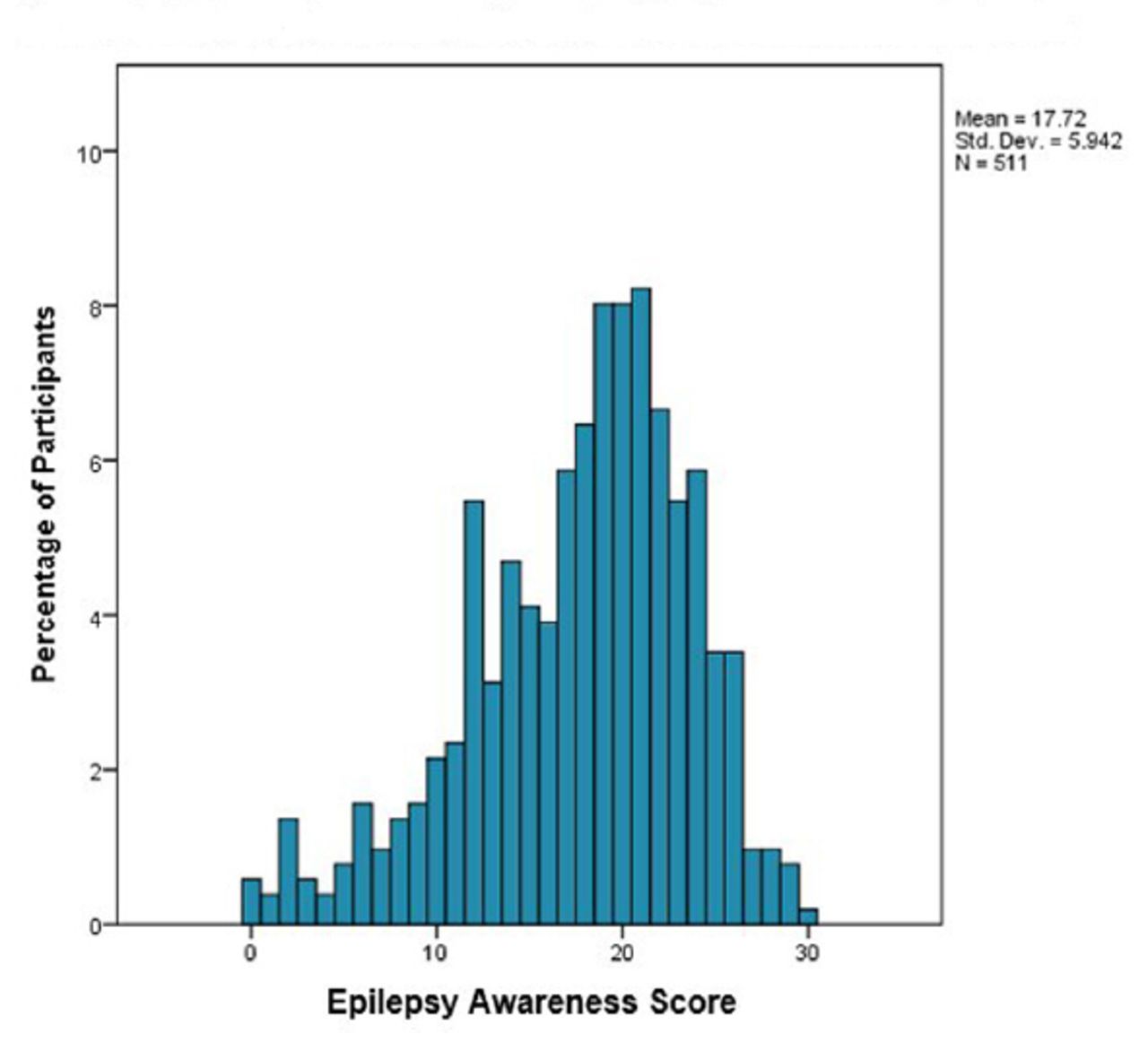
The average EAS was 17.7/45±5.9, with the highest score of 30 and the lowest score of zero (Figure 1). EAS was a significant association among those with children but not with gender (p=0.06), marital status (p=0.47), or education level (p=0.07) (Table 5). The data show a positive correlation with EAS with monthly income r=0.10 (p=0.02), and education level r= 0.08 (p=0.07). On the other hand, there is a negative correlation between age and EAS, r=-0.05 (p=0.26).
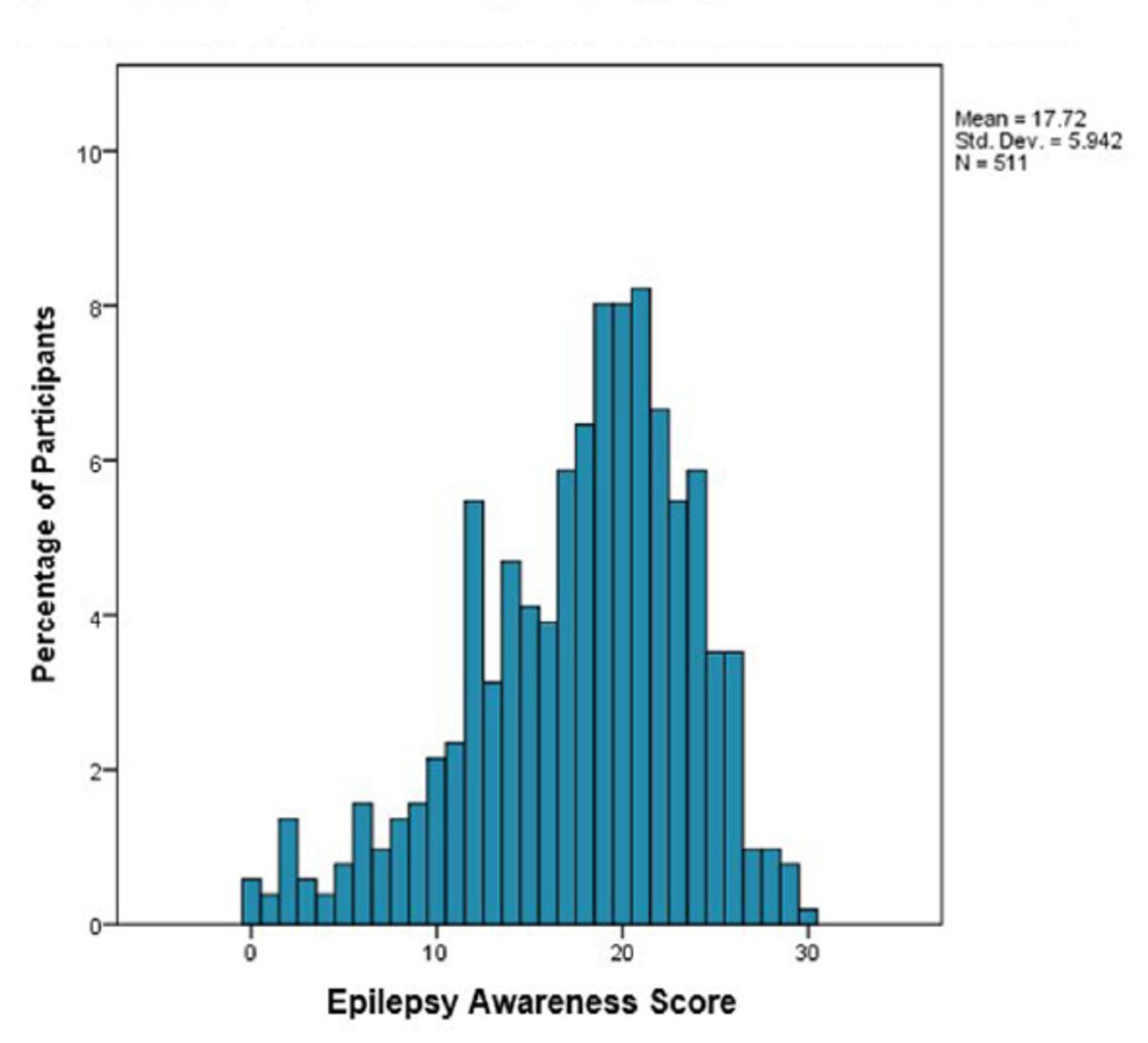
- Epilepsy awareness score distribution among participants
- Significance of epilepsy awareness score (EAS) with participants’ demographics and epilepsy background.
Discussion
Epilepsy patients tend for poor mental health, especially children. Combining with social stigma and lack of social support, the patient will suffer and have a poor quality of life. Therefore, a cornerstone to improving mental health for epilepsy patients is to have good social support and normalize the stigma of the disease. However, Rabigh is a province growing and transforming into a more urbanized area as many participants found to be moved from other provinces for work or study, most probably as the students represent almost one-third of the participants. Therefore, the combination of old and young generations may result in ambiguous situations that need investigation for better intervention in the future.8 Males and females were almost equally surveyed in this study, with the majority being middle-aged and educated. Most of the participants claim previous reading regarding epilepsy, and half of them witnessed an active seizure. However, only one-third stated to know what to do during an active seizure, and a mere 23% received first aid training for seizure management.; despite the epilepsy awareness campaigns in SA.14 However, there is not enough information about establishing awareness campaigns in Rabigh. Epilepsy awareness was also lacking in other Arab countries and some African and Asian countries.15–17 In addition, developed countries such as the United States have reported insufficient public knowledge regarding epilepsy,18 indicating that epilepsy awareness should be a global concern.
During an active seizure, most participants did not know what actions to take other than moving the seizing person away from harm. Answers such as putting a spoon or cloth in their mouth, splashing water on the person, holding or fixating them, or forcing their medication in their mouth are less than beneficial actions that could potentially be more harmful.19 Similar data was revealed in Saudi systematic review and meta-analysis study,14 and studies in other countries,20,21 suggesting further education regarding the first aid management of seizures is needed not only among the local population but also in other countries as well.
Participants had adequate knowledge of the symptoms of epilepsy attack, but improvement is needed as many recognize or are unsure if headache or hallucination is one of the symptoms. The causes of epilepsy can be divided into four categories: developmental, acquired, provoked, and cryptogenic epilepsy.22 Participants are mainly were able to identify the various causes of epilepsy correctly. However, the evil eye was mentioned among the causes of epilepsy more than the other common misconceptions causes mentioned in SA society, which is similar to another study in the western region of SA.10 Those who have previous reading regarding epilepsy, or those who witnessed an active seizure or claim they know what to do to someone having an active seizure or had first aid training all have significantly higher EAS. Therefore, establishing awareness campaigns, increasing first aid training, and improving self-efficacy to handle an active seizure all positively impact awareness and attitude toward epilepsy patients.
Regarding the stigmatization of the disease, many agreed that epilepsy was highly stigmatized but did not mind if their children socialized with epilepsy patients. Participants were undecided on their reactions if their child would marry a person with epilepsy. One study in Montenegro revealed similar results regarding marriage; however, parents were also anxious about having their children play with those with the disease.23 Parents of children with epilepsy are aware that their children are stigmatized due to their disease and worry about their offspring’s future.24
Studies for teachers’ epilepsy awareness are limited in SA.7 However, our data show that elementary school teachers have higher EAS than others (Table 5). On the other hand, a recent review study by Alkhotani25 shows that high school teachers had a higher level of awareness. Similar studies revealed that the younger teachers, the better their awareness.25,26 Also, our data show that the lower the age, the higher is EAS; however, it is not statistically significant (p=0.26).
We cover most of the questions in previous studies regarding epilepsy awareness in SA. However, this study has limitations as some variables have fewer than 5 respondents or are more deficient in one group than the rest, which may be imprecise in some analysis results. In addition, it should be considered that the sample contains a small number of ages over 55. Therefore, age-related results should be interpreted cautiously, and further research should cover older age.
Conclusion
Further efforts are needed to strengthen community knowledge and awareness regarding epilepsy. Stigmatization of the disease in society not only affects those that are afflicted, but it has consequences on their loved ones as well. Supplementary educational campaigns need to be carried out to normalize this condition and create acceptance and increase awareness regarding first aid in the community.
Acknowledgment
The authors want to thank PaperTrue (https://www.papertrue.com/) for English language editing. In addition, this research would not have been done without the help of many communities and social media service in Rabigh province that distributed the survey. Special thanks to them
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 3, 2022.
- Accepted July 3, 2022.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.