


Abstract
Objectives: To establish the prevalence of Neuropsychiatric Systemic Lupus Erythematosus (NPSLE) symptoms in Saudi Arabia and the variables that are linked to it.
Methods: This cross-sectional study was conducted in June 2021 among SLE patients in Saudi Arabia. The Saudi Rheumatism Association exploited social media platforms to provide a self-administered online questionnaire to SLE patients. All data analyses were performed using the Statistical Packages for Social Sciences (SPSS) version 26.
Results: Two hundred and eight SLE patients participated in the study (females 91.3% vs. males 8.7%). In addition, 13.5% of patients had a family history of SLE, and 26% had SLE for one to 3 years. The most common symptoms of NPSLE were alteration or loss of sensation (53.4%), followed by fear (52.4%), and headache (48.1%). The prevalence of patients with NPSLE was 40%. In a multivariate regression model, fear, altered sensations, cerebrovascular illness, sleep disruption, and diminished interest in routine activities were identified as independent risk variables for NPSLE
Conclusion: Nearly half of SLE patients demonstrated NP manifestations, with significant symptoms including fear, alteration of sensation, cerebrovascular disease, sleep disturbance, and reduced interest in normal activities. To detect the pathophysiology of NPSLE, it is necessary to understand the relationship between neuropsychiatric morbidity and other relevant rheumatic disorders in the SLE population.
Systemic Lupus Erythematosus (SLE) is an autoimmune connective tissue disease in which the immune system attacks the tissues of the body, resulting in inflammation and tissue damage. It can affect people of all ages, ethnic groups, and genders, while women are substantially more likely than males to get the condition (at a ratio of 9:1).1 In young women, the peak age of onset is between their late teens and early 40s (childbearing age).2 In our population there are limited studies regarding SLE, however, the prevalence and incidence of SLE varies upon countries in recent studies, the prevalence SLE is estimated to be 19.28 per 100,000 population using the ACR criteria.3 In a global review study, The overall global incidence of SLE ranges between 1.5 and 11 per 100,000 person-years, and the global prevalence ranges from 13 to 7,713.5 per 100,000 individuals.4 Maria Gulinello mentioned in her study 80% to 90% of SLE patients have some neuropsychiatric manifestation, with the most prevalent being depression (50% to 60%), headache (50% to 70%), and cognitive dysfunction (30% to 50%), according to comprehensive and specific neurologic and psychological diagnostic tools sensitive to the detection of dysfunction in the relevant behavioral domains. Seizures, anxiety, acute confusional state, stroke, and psychosis are other, less common signs.5 Ainiala, H study showed that The most prevalent symptom was cognitive dysfunction among 37 patients (81%). Then headache was detected in 25 patients (54%). Among 43% of the patients, depression consists of a major depressive episode of mild severity and mood disorders with mixed features was detected. Polyneuropathy was diagnosed in 13 (28.2%) patients. And cerebrovascular disease was detected in 7 patients (15%). To compare it with our study, which includes 208 participants, the most common symptoms of NPSLE were alteration or loss of sensation (53.4%), followed by fear (52.4%) and headache (48.1%).6 The prevalence of NP disorders in SLE patients in Pakistan was estimated to be 30.42%, with cognitive dysfunction being the most common (31.51%), followed by headache (10.22%), seizures (5.96%), psychosis (3.64%), and neuropathy is the least common (0.86%).7 The SLE has a wide range of symptoms since it can affect every organ in the body. Neuropsychiatric Systemic Lupus Erythematosus (NPSLE) is a group of symptoms observed in SLE that is likely the most frequent.4-6 Although these constitute one of the significant causes of morbidity and mortality in SLE patients, they remain poorly understood and can be challenging for physicians to recognize and manage. Nineteen major symptoms of NPSLE have been classified by the American College of Rheumatology (ACR), and this classification process has helped to guide subsequent research. Broadly, there are 2 major groups of symptoms: those involving the central nervous system (CNS) and those involving the peripheral nervous system (PNS), each of which is further broken into lesser divisions.8 The incidence of NPSLE symptoms in people with SLE varies widely between studies, ranging from 12% to over 95% in both children and adults. The Neuropsychiatric (NP) symptoms can sometimes emerge without any active systemic illness or serologic activity. That might be due to disease processes that impact the neural system directly, or because the disease process first affects other systems and subsequently affects the nervous system, or they could be a side effect of disease-controlling medicines.6,9-13 Although there has been a great deal of SLE-related research worldwide, there is a gap in NPSLE-related research, especially in Saudi Arabia. Consequently, this paper aims to determine the prevalence of NP symptoms among SLE patients in Saudi Arabia, assessing their knowledge, and understanding of NPSLE.
Methods
This cross-sectional study was conducted in June 2021 among SLE patients in Saudi Arabia. The Saudi Rheumatism Association (SRA) was approached to deliver the survey to SLE patients directly.
The SRA dataset has 335 SLE patients. Individuals who were incorrectly categorized as SLE patients or SLE patients under the age of 18 from the SSR database were eliminated. Subjects were approached through social media channels (WhatsApp, Instagram, and Twitter). A description of the study’s goal and a permission form was included with the survey. To confirm that only SLE patients are included, a “yes/no” question was asked at the beginning of the survey if the patient has SLE or not. Only those who clicked “yes” can participate. 208 (68.2%) out of 305 SLE patients responded to this questionnaire, and their responses were collected and analyzed.
The questionnaire consisted of 2 parts. The first part consists of 7 questions about patients’ demographic information. The second part includes questions adopted from the Mosca et al’s14 questionnaire. That aimed to screen the presence of neuropsychiatric symptoms in SLE patients in clinical practices. The Mosca et al14 questionnaire includes 27 weighted item questions, of which 12 questions are related to central and peripheral nervous system symptoms and 15 questions are related to psychiatric manifestations. Most of the answers to these questions are “Never, one episode, 2 episodes, or more than 2 episodes”. Also, one question related to the use of corticosteroids in improving headache was omitted, since using corticosteroids as a daily dose is not regular in most SLE patients’ treatment plans. In order to avoid confusion, 2 similar questions related to weakness and loss of muscle power were combined into one question since they have the same meaning “Never, one episode, 2 episodes, or more than 2 episodes,” is the most common response to these questions. As a result, the modified questionnaire contains a total of 25 questions, of which 10 questions are related to the central and peripheral nervous symptoms and 15 questions are related to psychiatric symptoms, in addition to the demographic questions.
To confirm the validity, a professional translator used the forward-backward translation process to translate the original questionnaire into Arabic. The modified questionnaire was reviewed by 2 consultant rheumatologists and one researcher who is an expert in the rheumatology research field. Their feedback was that the questionnaire was comprehensive and easy to complete.
Ethical approval was obtained by the Institutional Review Board (IRB) committee of the university. Patients have given their authorization for the Saudi Rheumatism Association to contact them via WhatsApp for any communication, including research surveys. No personal information was collected in the survey, and all data was anonymized. The overall test of the NPSLE symptoms questionnaire was 0.884, or 88.4 %, suggesting strong internal consistency (as measured by Cronbach’s alpha).
Descriptive analysis was performed to describe the SLE patients included in the study. For continuous variables, means and Standard Deviation were determined. Counts and percentages were used for categorical variables. The Chi-square test was used to examine the association between NPSLE symptoms and the patients’ socio-demographic variables. Also, univariate logistic regression model, as well as multivariate logistic regression model were used to estimate the crude and adjusted odds ratios and 95% confidence interval using 0.05 (two-sided) p-value as a statistical significance level. Statistical Packages for Social Sciences (SPSS) version 26 (Armonk, NY: IBM Corp., USA) was used for all data analyses.
Results
Two hundred eight individuals with SLE were enrolled in the current study. Table 1 shows that the most prevalent age group was 26–35 years old (36.5%), with practically all females (91.3%). The majority of the patients (86.5%) were Saudi nationals, and nearly half of them (49%) were single. In terms of education, the majority (68.3%) had a bachelor’s degree, whereas 56.7% were unemployed. Patients who said they had comorbidities were 47.1%.
- Socio-demographic characteristics of patients diagnosed with SLE (n=208)
In Table 2, it was shown that 26% of the participants had SLE symptoms for one to 3 years and 13.5% of the patients had a history of SLE in their families. In addition, 48.1% of people had frequent headaches, and 54% of them had headaches after they were diagnosed with SLE. Also, 48.1% of patients said they didn’t know much about SLE symptoms while E-books and research were the most prevalent sources of SLE knowledge (50.4%), followed by social media (48.7%). E-books and research (50.4%), social media (48.7%), and clinicians (36.1%) were the most prevalent sources of SLE information, with more than half (57.2%) having partial to full awareness of SLE symptoms.
- Duration of SLE and other related characteristics of patients (n=208).
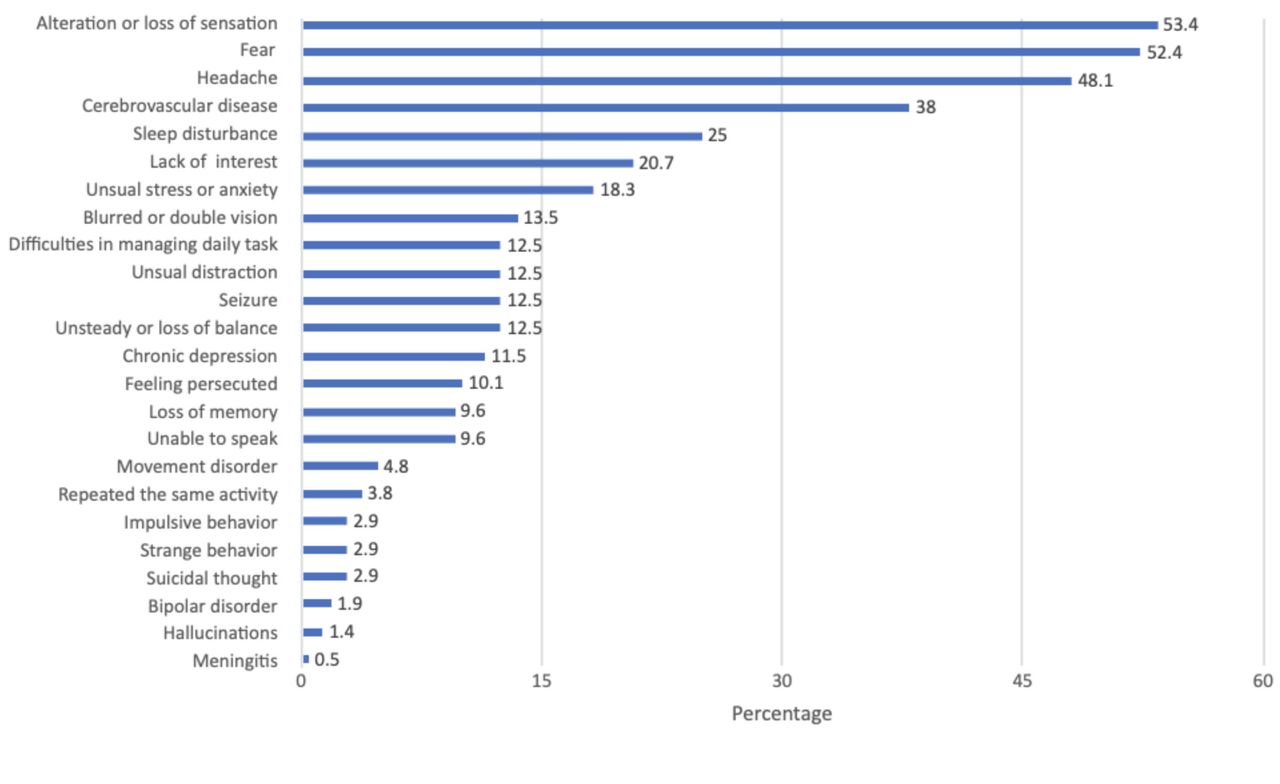
The current study showed that NPSLE symptoms affect 40% of the patients according to the modified questionnaire (82 patients). In addition, the most prevalent NPSLE symptoms were altered or loss of sensation (53.4%), fear (52.4%), and headache (48.1%) (Figure 1).
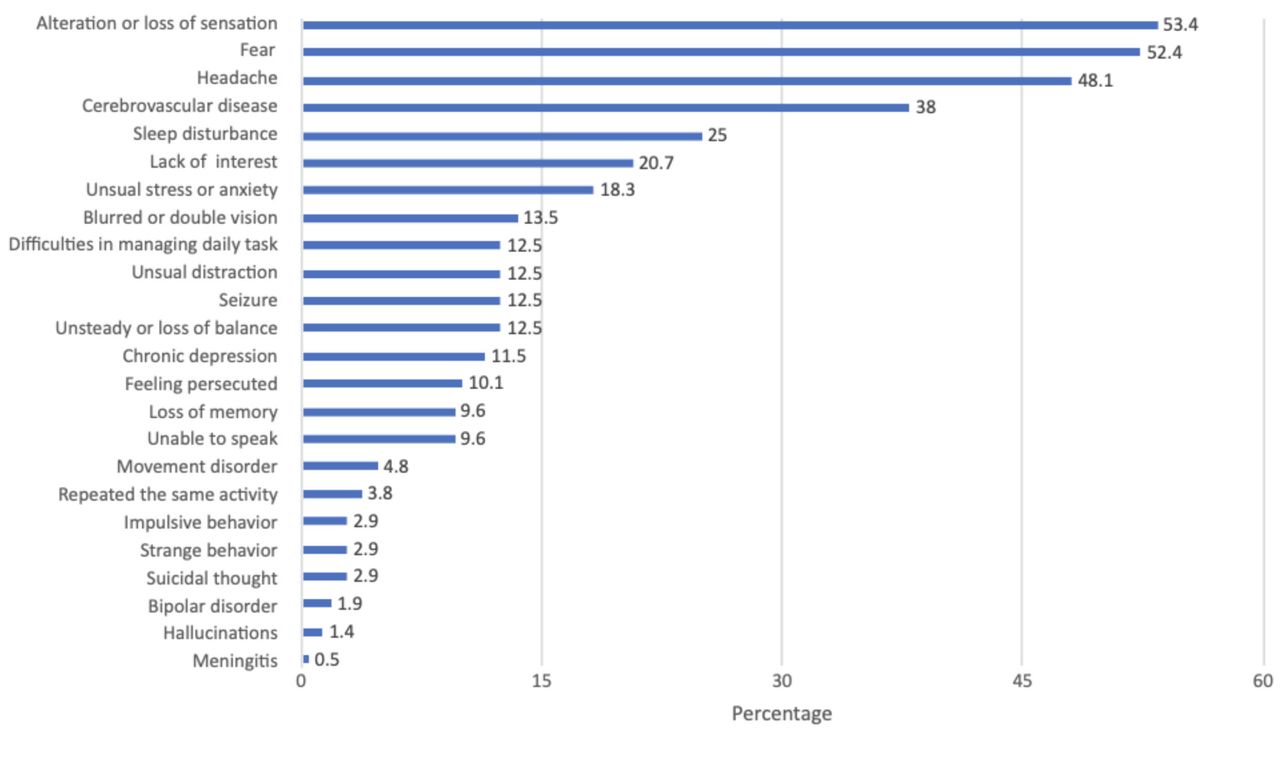
- Pattern of NPSLE manifestations in SLE patients in Saudi Arabia 2021.
Univariate logistic regression analysis shows that the risk of having NPSLE symptoms for patients with associated comorbidity was 80% higher than for those without the underlying disease (OR=1.8; 95% CI=1.0, 3.2; p=0.036) and this relationship remained significant after adjustment for confounder, which are age, marital status, educational level, occupation, duration since diagnosis with SLE, and knowledge about SLE symptoms. (AOR=2.1; 95% CI=1.2, 2.8; p=0.015). Also, the risk of NPSLE symptoms for the patients with a family history of SLE was 2.6 times higher than for those without a family history of SLE (OR=2.6; 95% CI=1.2, 5.9; p=0.021), and after adjustments, the odds increased to 3.2 (AOR=3.2; 95% CI=1.4, 7.6; p=0.008). Other variables included in the model did not show a significant impact on positive NPSLE symptoms, including age, marital status, educational level, occupation, duration since diagnosis with SLE, and knowledge about SLE symptoms (p>0.05). (Table 3). Among 208 participants with SLE some of them have associated comorbidities, 26 (12.5%) has hypertension, 3 (1.4%) has osteoporosis, 28 (13.4%) has thyroid disease and 9 (4.3%) has diabetes mellitus.
- Relationship between the level of NPSLE among the socio-demographic and other related characteristics of the patients. (n=208)
Discussion
The purpose of this study was to investigate the prevalence of NPSLE symptoms among SLE patients in Saudi Arabia. The prevalence of NPSLE symptoms among SLE patients in this research was 40%, according to Mosca et al’s criteria.14
According to our findings, 48.1% of patients suffered headaches following the beginning of SLE. Furthermore, we discovered that SLE patients with comorbidities will experience more NP symptoms than SLE patients without comorbidities, with an odd ratio of 1.8. we found that SLE patients with a positive family history of SLE had more NP symptoms than SLE patients with a negative family history OR=2.6. The NPSLE symptoms were shown to be prevalent across all age groups, marital status, educational level, employment, SLE duration, and SLE knowledge. According to Borowoy et al15 educational level, income level, age at diagnosis, disease duration, and gender were not significantly linked with NPSLE symptoms. However, our results showed that education, knowledge of SLE symptoms, age, marital status, occupation, or time since diagnosis had no significant impact on these NPSLE symptoms (p>0.05). Patients with NPSLE symptoms, on the other hand, were substantially older at the outset of the disease, according to Eissa et al.16 Also, our study showed that patients with SLE had a longer perceived duration. Changes in peripheral sensations were the initial and most prevalent NP symptoms in our investigation. Cognitive impairment (51%) was the most prevalent symptom of NPSLE in Ecuador,17 followed by anxiety disorders (41%), and mood disorders (40%). Twenty percent of our patients had a lack of interest as a psychiatric symptom which is one of the significant symptoms in diagnosing depression according to the DSM-5 criteria from the American Psychiatric Association. Furthermore, 18% of our patients had anxiety.
As stated in our results, there is a significant association of having NPSLE symptoms for patients with positive family history, the fact that the disease risk increased with a positive family history which may justify our findings (CDC). On the other hand, our study included all adult age groups, which could explain why age and other factors have no effect on NPSLE symptoms (Table 3).
When compared to previous research, The frequency of NP involvement among patients with SLE was 33.5% in Egypt,16 we discovered that we had a greater prevalence. However, the data gathered by several investigations has shown substantial variance. In a meta-analysis published by Unterman et al.18 The prevalence of NP syndromes in patients with SLE was estimated to be 56.3%. However, they emphasized that many NP syndromes, including cognitive dysfunction and autonomic conditions, may be difficult to distinguish and require a thorough examination of all patients to avoid underdiagnosis. According to the findings, the prevalence of NPSLE symptoms varies depending on the criteria used, with different assessments of the central nervous system (CNS) yielding varying estimations of NPSLE symptoms prevalence. The prevalence of NPSLE symptoms was better estimated using more limited criteria.18 Loss of sensation (53.4%), fear (52.4%), and headaches (48.1%) were the most common signs, according to our findings. Headaches have been described as a prominent symptom of NPSLE in several other studies.11,16,18
As far as we are aware, this is the first article to evaluate the NPSLE symptoms and its associated factors among SLE patients in Saudi Arabia. The study’s main value is that it shows how common neuropsychiatric signs and symptoms are in SLE patients in Saudi Arabia. Our questionnaire covered both neurological symptoms and psychological symptoms, as well as patients’ knowledge of SLE and the source of information. Research into Saudis’ knowledge of SLE can be further enhanced by the data we obtained. This should enhance awareness of the extensive presentations of SLE illness in our region among physicians, SLE patients, and their families, allowing patients to disclose their complete spectrum of symptoms when seeking medical treatment, and increasing their chances of getting a correct diagnosis.
Possible confounders in the study may arise from having other chronic diseases besides SLE or from side effects of a specific medication. In addition, Recall bias is a potential limitation of the study because participants may forget essential and helpful information. Patients filled the questionnaire by online survey and we did not use the scoring system in the questionnaire. Which is also important to consider as a limitation of the study some of the OR increased due to the small size. Patients with SLE who were recorded in The Saudi Society of Rheumatology (SSR) databases were included in our study. Other SLE patients in Saudi Arabia, on the other hand, may have different features. The NP symptoms were seen in nearly half of SLE patients. Fear, change or loss of sensation, cerebrovascular illness, sleep disruption, and lack of interest in regular activities were found to have a significant impact on SLE patients. After being diagnosed with SLE, a new-onset headache was found to be a common symptom. The NPSLE symptoms were more likely to arise in families with SLE and other chronic disorders.
Conclusion
Identifying the relationship between neuropsychiatric morbidity and other rheumatic disorders in distinct groups of SLE patients might help researchers better understand the pathophysiology of NPSLE. There is a need for further study that involves a larger sample size and fills the gaps regarding the NPSLE in our region.
Acknowledgment
We would like to thank Al-Nasekh Al-Arabi translation office (License No.578) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received November 21, 2022.
- Revision received June 13, 2023.
- Accepted June 13, 2023.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.