


Abstract
Aneurysmal bone cysts (ABCs) are rare benign vascular bony lesions mostly encountered in young patients. These cysts can occur as primary lesions or, less frequently, secondary to other pathologies such as osteoblastomas. Skull ABCs are rare and can extend intracranially, presenting with hydrocephalus and bleeding. Here we illustrate the case of a 9-year-old male who presented with headache, nausea, and vomiting, without neurological deficit. Radiological investigations showed a soap-bubble lesion with mass effect over the right cerebellum. The patient underwent right sub-occipital craniotomy with marginal wide resection of the cystic lesion. The patient had excellent outcomes. The histopathological report was consistent with osteoblastoma with an aneurysmal bone cyst.
An aneurysmal bone cyst (ABC) is a blood-filled benign expansile lesion of the bone first described in 1942 by Jaffe and Lichtenstein.1 The majority of cases have occurred in young patients during the first 2 decades of life, with a slight female predominance. Although ABCs can occur anywhere in the skeletal system, these lesions are commonly present in the metaphysis of long bones and vertebrae. Other locations, such as the head and neck, remain extremely rare, with an incidence of 2-3% of all ABCs.2 When located in the skull, ABC can extend intracranially and presents with cerebral hemorrhage and hydrocephalus.2,3 Despite the use of different modalities that successfully treat such lesions, surgical resection remains the mainstay of treatment, with lower recurrence rates.4,2,5 Here we report a case of secondary ABC of the occipital bone with an intracranial extension.
Case Report
Patient information
A 9-year-old otherwise healthy boy presented with headache, nausea, and vomiting of one-week duration.
Clinical findings
No neurological deficit was observed on physical examination. Local examination revealed a 10x10 cm right occipital diffuse and hard swelling associated with mild tenderness.
Diagnostic assessment
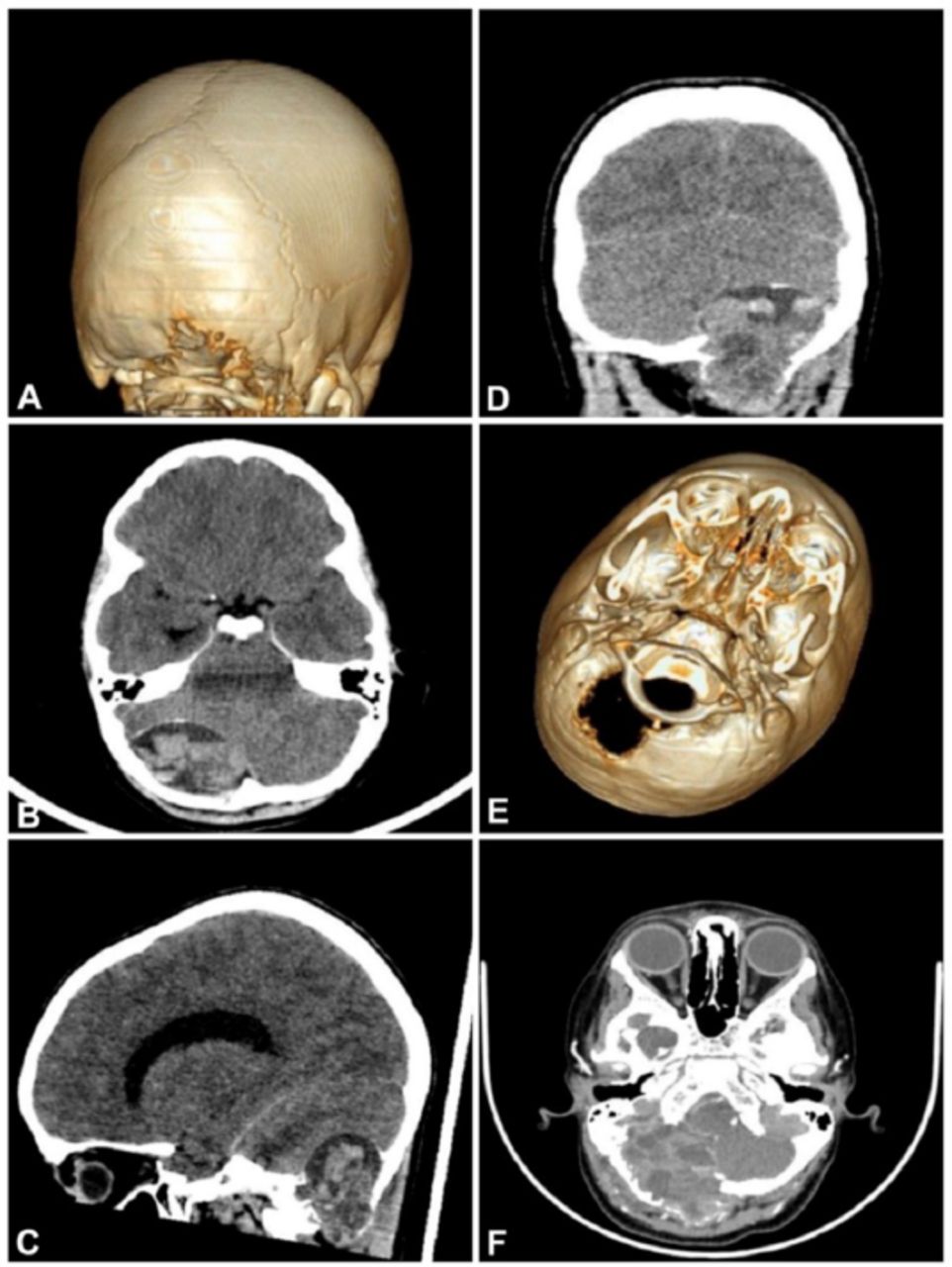
Computed tomography (CT) of the brain showed a 5x5 cm right occipital expansile bony lesion with heterogenous densities and a thin sclerotic rim (soap-bubble appearance with internal septation) (Figure 1). The lesion was exerting a mass effect over the adjacent cerebellum (Figure 1b &1c &1d). The CT angiography showed that the fourth segment of the right vertebral artery lies close to the anterior margin of the lesion. (Table1).
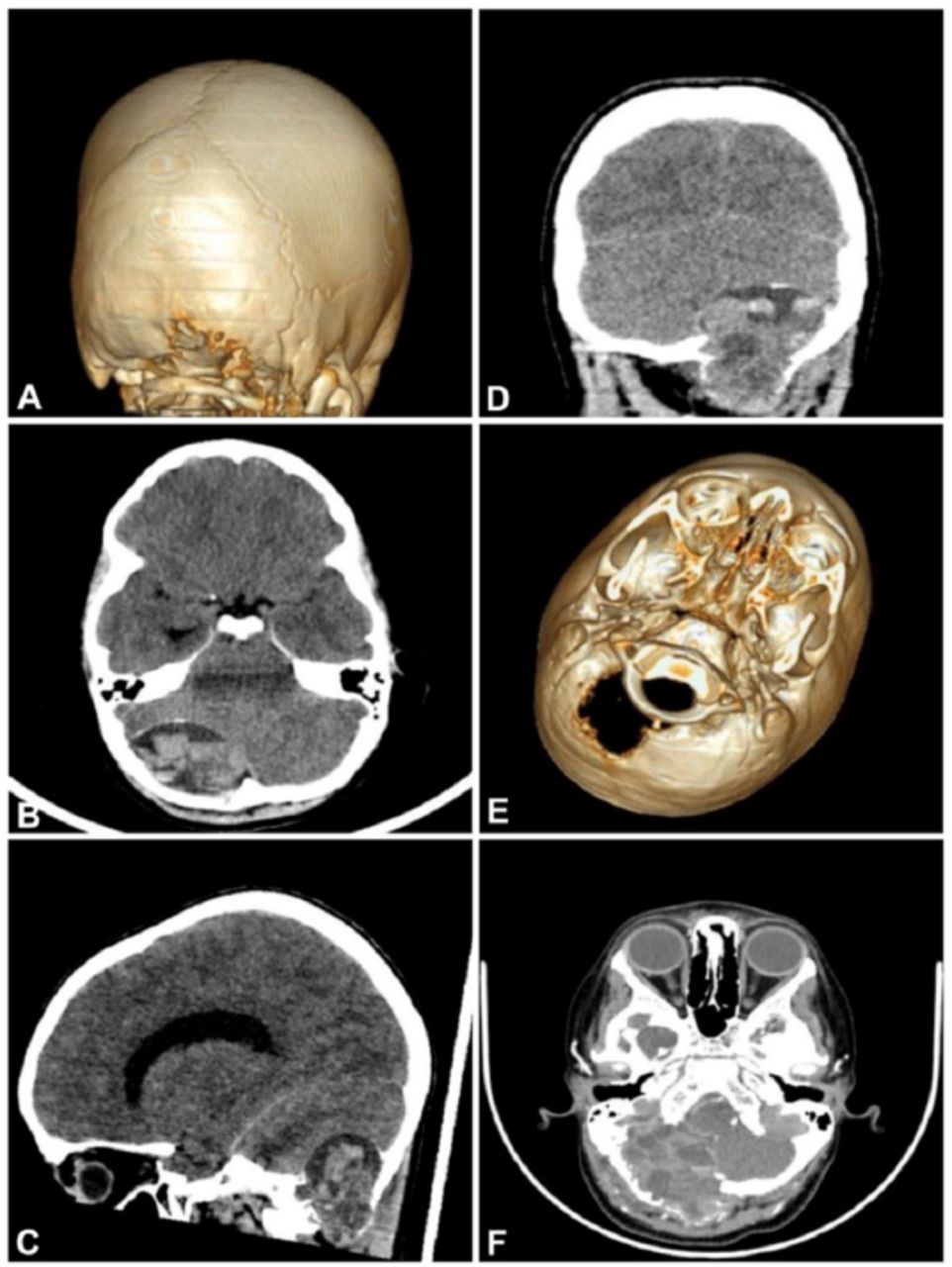
- Pre-op computed tomography (CT) brain showing occipital lesion demonstrating soap-bubble appearance.
- Timeline.
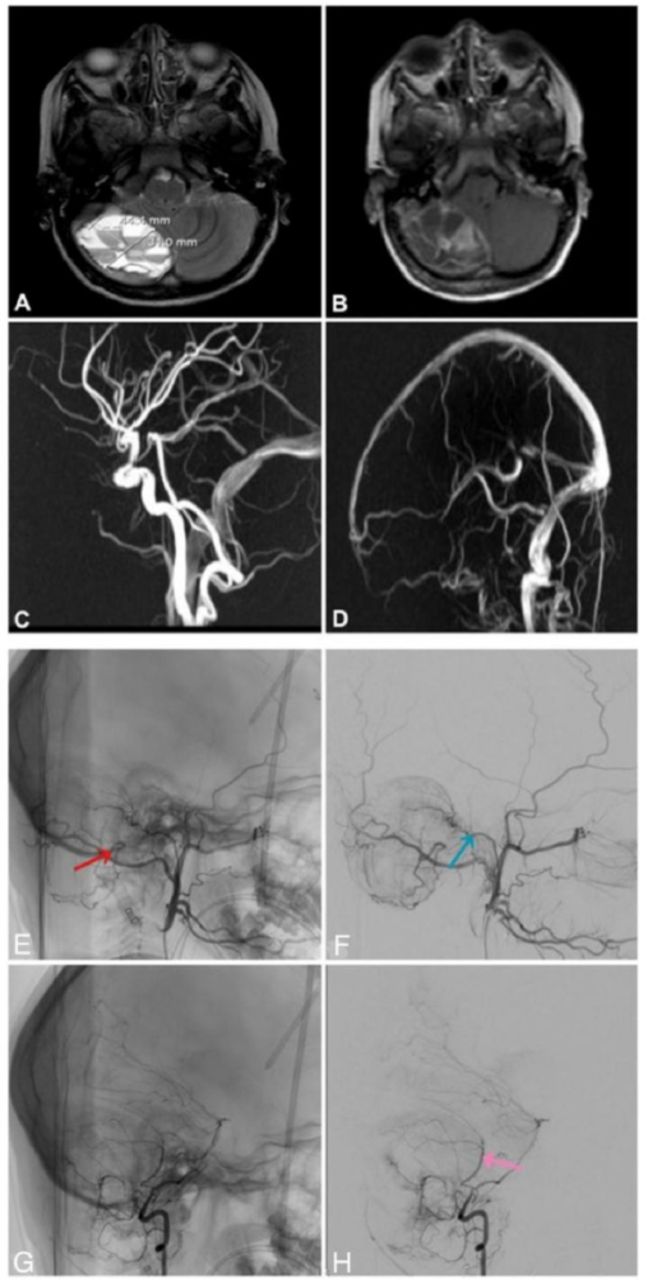
An infusion of contrast medium resulted in massive enhancement of the septa between the blood lakes, which inconstantly showed fluid-fluid levels (Figure 1f). Magnetic resonance imaging (MRI) of the brain demonstrated clear fluid-fluid levels, which indicates bleeding at different stages (Figure 2). More delineation of vascular anatomy was done by cerebral angiography which showed main blood supplies from the right external carotid artery (ECA). The largest contribution was from branches of the right occipital artery (supplying the inferior and mid-portion of the cyst) (Figure 2e) and the meningeal branch of the ascending pharyngeal artery (supplying the superior portion of the cyst) (Figure 2f). Moreover, the lesion had a blood supply from segmental branches at the C2 level and meningeal branches of the Posterior Inferior Cerebellar Artery (PICA) (Figure 2g & 2h). Endovascular embolization was not done, because it carried a risk of potential strokes.
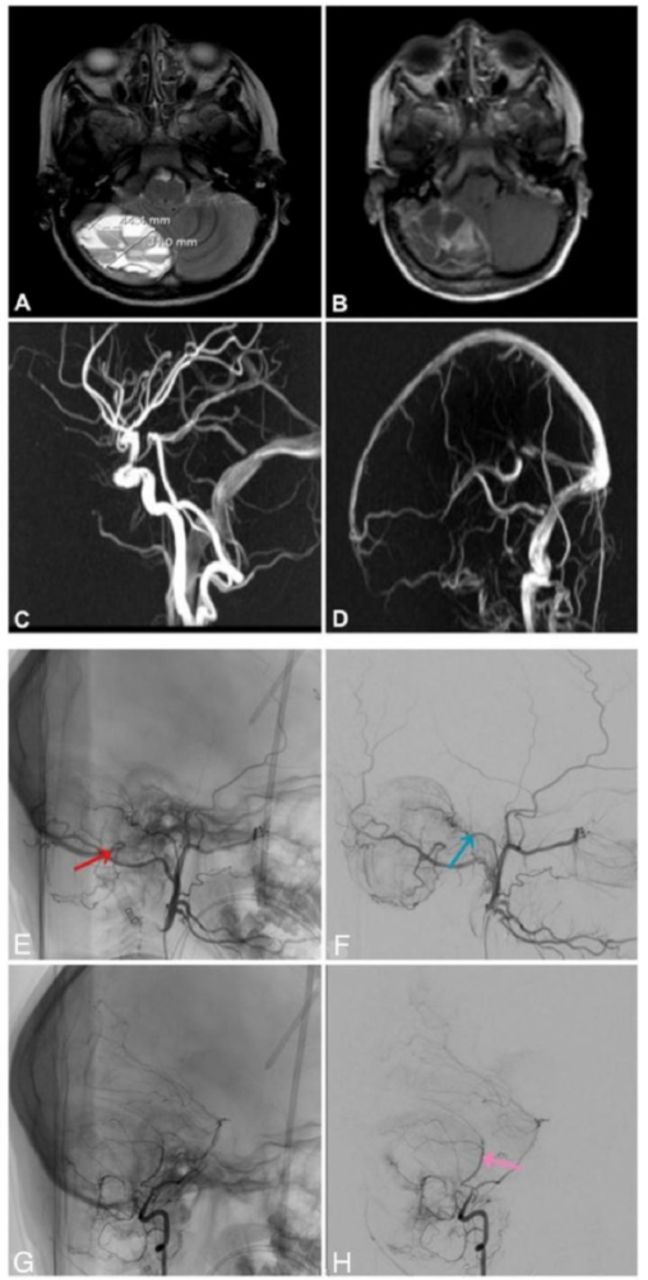
- The T1 and T2 MRI brain show different signal intensity suggesting acute stage hematoma. The MRA and MRV showed intact vascular anatomy. Right ECA artery injection cerebral angiography showing the right occipital artery (red arrow) and ascending pharyngeal artery (blue arrow) supplying midportion and superior portion respectively. Right VA injection cerebral angiography shows meningeal branches of PICA (pink arrow) supplying the tumor. MRA - Magnetic Resonance Angiography, MRV - Magnetic Resonance Venography, PICA - Posterior Inferior Cerebellar Artery, ECA - External Carotid Artery
Therapeutic intervention
The patient was scheduled for elective craniotomy and tumor resection. However, he developed active hydrocephalus, as demonstrated by follow-up outpatient CT of the brain. We performed an external ventricular drainage insertion, followed by lesion resection. The patient underwent right sub-occipital craniotomy and marginal wide resection of the cystic lesion.
Surgical technique
The operation was performed under general anesthesia in a prone position and the head was fixed via a Mayfield clamp (Figure 3a). Ultrasound doppler was used to map the pulsation of the right occipital artery. We started the surgery by opening the skin in a hockey stick fashion as the lesion is situated at the para-midline (Figure 3b). Muscles in the right sub-occipital triangle were opened layer by layer until the deep layer was found stuck to the lesion. The right occipital bone was expansile, soft, and very bloody. The periosteal layer was difficult to identify due to tumor invasion. The lesion was removed using bipolar cautery and was sackable piecemeal. It consisted of a gray-brown mass overflowing with blood. Its margins were hard, while the center was soft. It was multiloculated and filled with blood. The outer tablet was breached and the inner tablet was bulging inward, displacing the dura, which was adherent but not invaded by the tumor.

- The patient position on the operating table. The Surgical cavity of the tumor after complete wide resection.
Wide resection was achieved and safe margins were ensured. Tumor resection left an empty surgical cavity, indicating a slowly progressing lesion with a remodeling effect on the surrounded structures (Figure 3c & 3d). The bone defect was closed and reconstructed using a Medpor-titanium mesh. We achieved hemostasis, closed the skin, and extubated the patient.
Pathological examination revealed multiple fragments of hemorrhagic and dark brown firm tissues. Serial sectioning revealed blood-filled hemorrhagic cysts spaces. The primary pathological diagnosis was osteoblastoma with a prominent aneurysmal bone cyst.
Follow-up and outcomes
The post-operative course went smoothly, the patient recovered gradually and EVD was removed without the need for permanent shunting.
Discussion
The ABCs are rare non-neoplastic lesions with an incidence of 0.14 per 100,000 individuals according to the literature.6 ABCs represent 1-2% of primary bone tumors.7 ABCs are cystic, fibrous walled, blood-filled bone cavities that resemble soap bubbles.6 About 70% of all ABCs occur as primary pseudotumors, while the remaining 30% present secondary to other lesions, such as giant cell tumors, osteoblastomas, chondroblastomas, or fibrous dysplasia.7 Intracranial ABCs are reported in 2-6% of all cases, most of which are located in the temporal bone, followed by the occipital, frontal, and parietal lobes. The sphenoidal sinus and ethmoid bone remain the least common sites.6
Here we describe a rare occipital ABC extending intracranially and presenting secondary to osteoblastoma. Clinical presentation can vary depending on lesion location. Pain at the site of the ABC and tenderness are frequently reported. Patients with intracranial ABCs can present with headaches and symptoms suggestive of high intracranial pressure (ICP), like nausea and vomiting, hydrocephalus, cranial nerve palsies, seizures, and gait disturbance, and rarely cerebral hemorrhage.8 This patient presented with symptoms suggestive of increased ICP with no neurological deficit on examination. Diagnosis of ABCs hugely relies on radiological features. On a CT scan, ABCs often appear as expansile lytic lesions with widened diploic spaces, septations, and well-defined margins that show enhancement after administration of contrast media.9 An MRI usually shows an expansile well-defined mass that is lined by a hypointense rim with internal septations that divide the lesion into small cavities. A fluid-fluid level is the hallmark of ABCs, which indicates sedimentation of red blood cells inside the cavities.8,9
We observed these radiological features in our patient, which made ABC a top differential. Although total resection is the goal of treatment, it could be difficult to achieve depending on the site involved and the patient’s overall condition. Incomplete resection showed recurrence rates of 20-70%.10 Due to high vascularity, preoperative embolization can be used to minimize bleeding.10 However, in our case, total surgical excision was achieved without a prior embolization with excellent outcomes and no complications. When surgical resection is not possible, other treatment modalities can be used. These include radiotherapy, sclerotherapy or cryotherapy, and intralesional curettage.9,10
Conclusion
The ABCs are rare, vascularized lesions with a high risk of bleeding. Although cerebral angiographic embolization helps decrease vascularity, we preferred to proceed with surgery and bypassed this step. Intraoperatively, we didn’t face any major complications and the outcomes were excellent. Therefore, it is possible to achieve total resection with good outcomes without a prior embolization.
Acknowledgement
We would like to thank Wordvice company for their distinguished job in providing an excellent English editing service.
- Received May 30, 2023.
- Accepted September 4, 2023.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.