


Abstract
Objectives: To determine the relationship between hemoglobin A1c (HbA1c) and different types of stroke, and how different comorbidities and risk factors are related to the occurrence of stroke in a Saudi Arabian tertiary care hospital.
Methods: This retrospective study was conducted at King Abdulaziz Medical City, Riyadh, Kingdom of Saudi Arabia. The study included patients who experienced either hemorrhagic stroke (HS), ischemic stroke (IS), or transient ischemic attack (TIA) between 2015 and 2020.
Results: In total, 976 patients were included, of whom 670 were males (68.6%). The incidence of HS was significantly higher in males compared to females (14.2% vs. 6.9%), whereas the incidence of IS was higher in females (76.8% vs. 74.6%) (p=0.001). Ischemic stroke was significantly higher in the 65 years or older age group, whereas HS was comparatively higher among those aged <65 years. The means HbA1c levels in all three types of stroke were abnormally high. However, HbA1c levels were significantly higher in IS than in the other 2 stroke types (p=0.017). The HbA1c levels showed statistically significant differences between the different types of stroke, where the estimated marginal means were higher in patients with IS with a small effect size. Heart disease was also more prevalent in the IS group. Stroke-related mortality was reported in 16 patients and was significantly higher in the IS group than in the HS group.
Conclusion: The HbA1c levels were elevated in all types of stroke, significantly in IS. Controlling patients’ HbA1c and other modifiable risk factors could significantly reduce the risk of stroke.
Stroke refers to the sudden neurological deterioration caused by a decrease or compromise in blood supply.1 It is the second most common cause of mortality and a major cause of morbidity.2 According to a report by the American Heart Association in 2022, there were approximately 765,000 cases of stroke in the United States (US).3 Another study conducted in the US found that stroke is responsible for 165,000 deaths annually.4 Statistics regarding stroke are insufficient when considering Saudi Arabia; however, a study conducted in 2020 suggested that there are 29 stroke cases per 100,000 people annually.5 Another study reported that stroke was the second leading cause of death in Saudi Arabia.6
Stroke can have various etiologies, but the 2 main types are Ischemic stroke (IS) and Hemorrhagic stroke (HS). Ischemic stroke accounts for 87% of all stroke cases worldwide.3 It arises when the blood flow to a part of the brain is compromised, which leads to the deprivation of vital nutrients and oxygen in the brain tissue. Ischemic stroke can occur due to an embolus or thrombus lodging in an artery that supplies the brain, or it could be due to a stenosis in an arterial lumen of the brain.7 The second most common type of stroke is HS, which accounts for approximately 10% of all strokes. Hemorrhagic stroke arises when a vessel in the brain ruptures, leading to intracerebral hemorrhage.7 Hemorrhagic stroke is usually caused by hypertension, cerebral amyloid angiopathy, or an IS that has converted into an HS.7 Risk factors are classified as either modifiable or non-modifiable risk factors. Race, ethnicity, age, genetics, and sex are non-modifiable risk factors. On the other hand, modifiable risk factors for stroke include atrial fibrillation (AF), hyperlipidemia, hypertension diabetes mellitus, physical inactivity, and transient ischemic attack (TIA).8
A recent study conducted in the US to determine the risk of stroke in patients with type 2 diabetes mellitus found a bimodal distribution between stroke development and hemoglobin A1C (HbA1c) levels. Moreover, they found that patients with poor or strict glycemic control (HbA1c less than 6%) were at an increased risk of HS rather than IS.9
This study aimed to determine whether an increase or decrease in HbA1c was linked to HS and IS in the Saudi Arabian population at a tertiary care medical hospital. We also aimed to understand how different comorbidities, including heart disease, smoking, and previous cerebrovascular accidents, play a role in stroke formation.
Methods
This retrospective chart review was conducted at the Neurology Department of King Abdul-Aziz Medical City, Riyadh, Ministry of National Guard Health Affairs (MNGHA) in Kingdom of Saudi Arabia. The study (SP22R/215/09) was approved by our Institutional Review Board. As the study was conducted retrospectively, informed consent was not required. However, to ensure the safety and privacy of patient data, any information that identified the patient was removed and replaced with a code.
This study employed a non-probability convenient sampling method. A total of 976 patients with stroke met the inclusion criteria. Our inclusion criteria were male and female patients aged 18-100 years admitted with IS, HS, or TIA. Patients aged <18 years, >100 years, admitted with a condition other than stroke, or not admitted to the Neurology Department, were excluded from the study. Data were collected from the MNGHA Neurology Department from patients’ medical records using the BestCare electronic system. All data were collected between 2015 and 2020 which included demographics (history of smoking, gender, age, and body mass index (BMI)), clinical data that such as pertinent medical history, laboratory results, and imaging.
If applicable, patient data on arrival, medical history, history of medications (statins, antiplatelets, and anticoagulants), HbA1c levels, blood pressure upon admission, previous cardiovascular disease (valvular heart disease (VHD), AF, and coronary artery disease (CAD)), radiological imaging results (computed tomography and magnetic resonance imaging), and outcomes were collected. Stroke was classified as IS, TIA, or HS. Regarding HbA1c, the World Health Organization (WHO) guidelines for diabetes and hypertension were followed. A HbA1c value greater than 6.5% was considered high.10 Patients with blood pressure readings equal to or greater than 140/90 mmHg were considered hypertensive.11
Data entry and analysis were performed using the statistical program IBM Statistical Package for the Social Sciences Statistics for Windows version 23.0 (IBMCorp, Armonk, NY, USA). Categorical data, such as diabetes and smoking, are presented as percentages and frequencies, on the other hand, numerical data, such as age, are presented as standard deviations and means.
The chi-square test was used to assess the prevalence and significance of the type of stroke, and other factors, such as hypertension, smoking, and age group, with a confidence interval of 95%; a p-value <0.05 was considered statistically significant.
An analysis of variance (ANOVA) test was used to assess whether there was any difference in HbA1c levels between the three types of stroke, with a confidence interval of 95% and a p-value <0.05 considered statistically significant.
An analysis of covariance (ANCOVA) test was used to assess if any other categorical variables influenced the level of HbA1c, such as aging, previous stroke, previous TIA, and statin therapy, with a confidence interval of 95% and a p-value<0.05 considered statistically significant.
Results
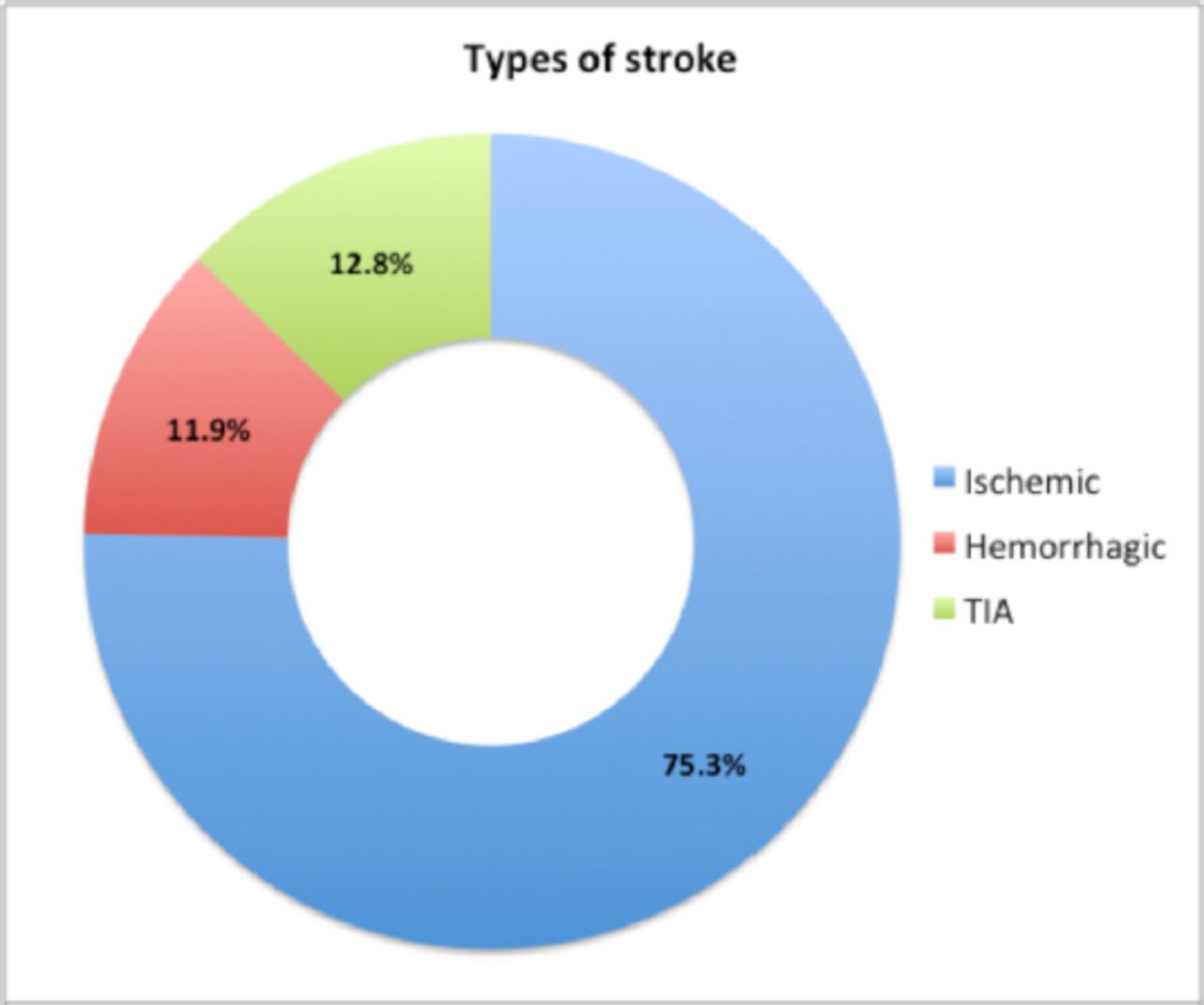
Our analysis included the medical records of 976 patients with stroke. Of these patients, 735 (75.3%) had IS, 116 (11.9%) had HS, and 125 (12.8%) had TIA (Figure 1).
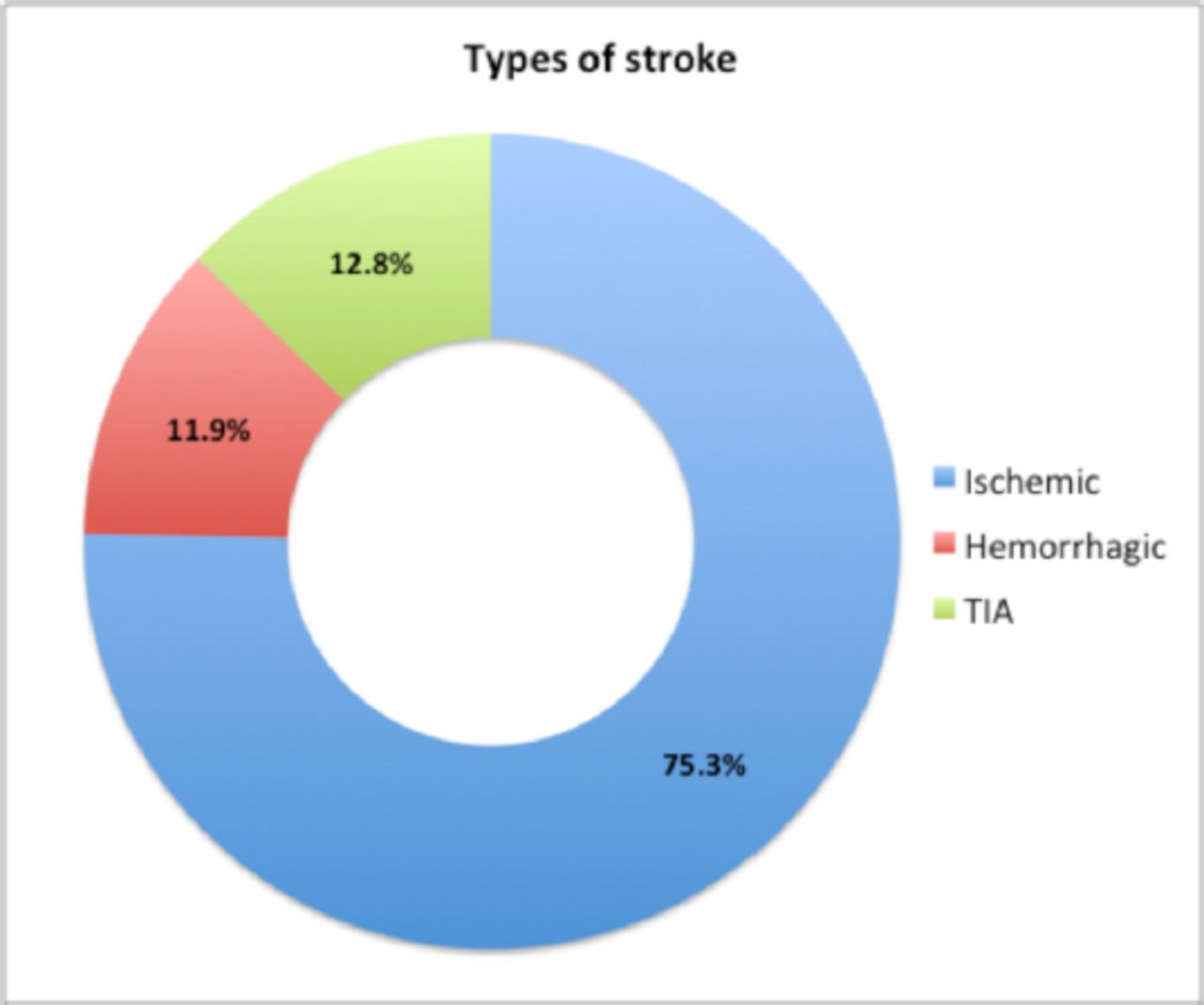
- Distribution of different types of stroke.
The gender distribution showed that 670 (68.6%) patients were male and 306 (31.4%) were female. Hemorrhagic stroke was significantly more prevalent in males than in females (14.2% vs. 6.9%), whereas IS was more prevalent in females (76.8% vs. 74.6%) (p=0.001). The mean age of the patients in our study was 60.8±12.3 years and the ages ranged from 15 years to 97 years. In addition, 408 (41.8%) patients were aged 65 years or above. Ischemic stroke was significantly higher in this age group (79.7%), whereas HS was comparatively higher among those aged under 65 years (p=0.008).
A total of 78.7% patients with stroke had a BMI of >25. However, no significant relationship was observed between BMI and stroke type (p=0.718). Approximately 710 (72.7%) patients had hypertension; however, no statistically significant differences were observed in the distribution between the different types of stroke (p=0.569).
Approximately 208 (21.3%) patients had a history of stroke, which was significantly higher among those with IS (p=0.031). Approximately 169 (17.3%) patients had a history of CAD, AF, or VHD, which was significantly higher in patients with IS than in those with other stroke types (p=0.003). Previous TIA was reported in 23 (2.4%) patients, and approximately 30.4% of the patients who had TIA had a previous TIA as well (p=0.013). It was found that 799 (81.9%) patients used anticoagulants and antiplatelets, of whom 81.7% had IS (p<0.001). Approximately 711 (72.8%) patients used statins, of whom 81.3% had IS and only 4.5% had HS (p<0.001). In our sample, 142 (14.5%) patients were smokers; however, there were no statistically significant differences in their distribution considering the different types of stroke (p=0.416). Total mortality related to stroke was reported in 16 (1.6%) patients and was significantly higher in patients with IS than in those with HS (62.5% vs. 37.5%) (p=0.003) (Table 1). The mean HbA1c levels in all three types of stroke were found to be high. However, the mean HbA1c levels were significantly higher in IS patients (8.17±2.34) compared to other types of stroke patients (p=0.017) (Table 2).
- Distribution of different types of stroke according to patient medical history and demographics
- Comparison of HbA1c levels (n=976).
We performed ANCOVA to test the main and interaction effects of categorical variables on continuous HbA1c levels (Table 3). The HbA1c levels showed statistically significant differences between the different types of stroke, where the estimated marginal means (EMMs) were higher in the IS group with a small effect size (F(2,974)=3.156, p=0.043, ηp2=0.7%). To further explore the significant interactions, EMMs were computed for each type of stroke. The EMMs was found to be 8.154, 7.842, and 7.619 for IS, HS and TIA, respectively.
- Univariate ANCOVA model.
Post hoc analyses were conducted using Bonferroni test, revealing significant differences between IS and TIA (p=0.043), but not between IS and HS (p=0.227) and HS and TIA (p=0.992).
Discussion
Our study found that the Hb1AC level was high in all types of stroke but was significantly higher in the IS group. The incidence of HS was higher than IS in males, whereas IS was higher in females. The incidence of HS was also higher in the group aged less than 65 years, while IS was higher in the age group of 65 years and above. The incidence of underlying heart disease was significantly higher in the IS group than in other stroke types. A high percentage of patients using anticoagulants developed IS. The mortality rate was significantly higher in the IS group than in the HS group.
Our study shows that HbA1c levels are elevated in all types of stroke but are significantly elevated in those affected by IS. This is consistent with previous reports that an increase in HbA1c is associated with first-time stroke in both patients with or without diabetes.12 Another study that included 44,451 patients with diagnosed AF and diabetes mellitus found that stroke risk is increased in patients with HbA1c of 7% or more in comparison to patients with that less than 7%. Moreover, HbA1c levels > 9% significantly increased the mortality risk.13 A meta-analysis of 39 studies found that diabetes was less prevalent in patients with HS than in those with IS.14 Furthermore, several studies have found that high glucose levels are associated with worse neurological and functional outcomes, longer hospitalization duration, and stroke recurrence.14 A study conducted in a tertiary care center in Saudi Arabia found that the most common subtype of stroke in the diabetic population was large artery disease, which is a subtype of IS. In addition, most of the patients who developed stroke had diabetes.15 Another study conducted by Al-Rubeaan et al. in Saudi Arabia found that HbA1c levels were significantly higher (8.9%) in patients with stroke and that IS was associated with poor glycemic control.16
Age and sex are known to increase stroke risk. The incidence of stroke increases with age until the 7th decade of life in Saudi Arabia.17 Additionally, the average age for stroke in males was less than females.18 In our study, the number of patients aged 65 years and older was approximately 408 (41.8%). In 2009, a study found that the stroke incidence in males was approximately 30% higher than that in females.19 Another study also showed that prevalence of stroke in males aged ≥40 years was significantly higher than females.20 Moreover, females have a higher risk of TIA and IS,21 whereas males were found to have a higher incidence of HS.22 One study suggested that women above the age of 85 years had a higher stroke incidence than males of the same age group.23 Consistently, our study found that IS was higher in females while HS was twice as common in males. Furthermore, HS is comparatively higher in ages of less than 65 years, while IS is significantly higher in ages of 65 years and above.
Atrial fibrillation is known to increase the risk of stroke by up to 5 times and is usually related to IS.24,25 One study showed that healthy young males with AF did not seem to have a significantly increased risk of stroke.26 CAD was found to increase the risk of stroke by almost 3 times, but a recent review article showed that it might not be related to stroke based on results from Japan.27,28 Valvular heart disease related risk of stroke varies depending on the population and the affected valve. For example, in American Indians, mitral annular calcification is a strong risk factor for stroke, mainly IS, but aortic valve stenosis is not considered a risk factor for stroke.29 In our study, we found that 17.3% of patients with previous heart disease had a significant risk of both types of stroke, but mainly IS.
In our study, the mortality rate was 1.6%, with the majority of deaths related to IS compared with HS (62.5% vs. 37.5%). Furthermore, the mortality rate in patients with HS was higher than that in patients with IS (5.1% vs. 1.4%). Therefore, HS is more fatal but less common than IS. Consistent with our observations, a previous study conducted between 1982 and 1992 in Saudi Arabia found higher mortality rates in patients with HS.30 In addition, a systematic review conducted in the Middle East found that HS was more lethal than IS.31 Furthermore, another study conducted between 2001 and 2005 in Sweden found that the chance of survival was greater in patients with IS than in patients with HS.32
Our study has several limitations, during the data analyses, patients who were older than 100 years old were excluded. Overweight and obese patients were analyzed as a single group, and the WHO classification of obesity was not specifically followed for BMI. Additionally, anticoagulation and antiplatelet drugs were grouped into one category, resulting in a lack of insight into their effectiveness. Drug adherence and duration of therapy with antiplatelet agents, anticoagulants, and statins were not documented in the data collection. Furthermore, we divided the age groups into two categories: younger and older than 65 years. A more detailed approach for age classification was not implemented. All heart conditions were analyzed in a single group. Lastly, our study lacks generalizability as all data were collected from a single tertiary care center.
In conclusion, HbA1c levels were elevated in all types of stroke but were significantly higher in the IS group. The incidence of HS was higher in males, while IS was higher in females. In addition, cardiovascular diseases had a significant association with stroke occurrence, especially IS. A decrease in HbA1c levels and having a control over other modifiable risk factors could have a significant reduction of stroke rates in our population, however, studies should be conducted to further evaluate the morbidity and mortality rates of all types of stroke in Saudi Arabia. Awareness campaigns targeted at the general population and schools, early detection of chronic diseases and diabetes, and health programs should be encouraged to raise awareness among our population and decrease the rate of stroke.
Acknowledgement
We would like to acknowledge Editage editing services for English language editing.
- Received April 17, 2023.
- Accepted September 19, 2023.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.