


ABSTRACT
Objectives: To examine the occurrence and contributing factors of disordered eating patterns in individuals post-bariatric surgery. It also investigated the impact of these patterns on weight loss outcomes and long-term weight management, focusing on psychological and emotional factors. Additionally, the relationship between body image dissatisfaction and disordered eating patterns was explored.
Methods: A cross-sectional study was conducted across multiple medical centers in Saudi Arabia, using self-administered questionnaires to evaluate the prevalence of eating disorders and self-esteem among patients who underwent bariatric surgery in the past five years. Out of 557 respondents, 452 met the inclusion criteria.
Results: The study found that 21.5% of participants experienced psychological disorders post-surgery. Notably, there was a significant improvement in mean self-esteem scores after surgery. Depression was the most frequently reported disorder (12.4%), followed by Generalized Anxiety Disorder (9.3%) and Eating Disorders (4.6%). The mean Rosenberg Self-esteem Scale score increased significantly from 28.17±6.2 pre-surgery to 31.7±5.3 post-surgery (p<0.001).
Conclusion: The findings highlight a notable prevalence of psychological disorders among post-bariatric surgery patients, with depression being the most common. Despite this, significant improvements in self-esteem were observed. Understanding the psychological and emotional factors contributing to disordered eating patterns and body image dissatisfaction is crucial for improving long-term weight management and patient outcomes post-surgery.
Eating disorders (EDs) are behavioral problems defined by significant and persistent disturbances in eating behavior and its associated harmful thoughts and feelings. These can be life threatening and affect one’s physical, mental, and social functioning.1 Eating disorders and disordered eating symptoms are influenced by multiple biopsychosocial factors, some of which are now recognized as established risk factors. Evidence suggests that genetic predisposition, premature birth, birth trauma, and biochemical individuality significantly influence the eventual development of an eating disorder.2 Data suggest that psychological and environmental factors interact with and influence the expression of genetic risk to cause eating pathology.3 The sociocultural idealization of thinness variables (media exposure, pressures for thinness, thin-ideal internalization, and thinness expectancies) and personality traits (negative emotionality, perfectionism, and negative urgency) has attained “risk status” for eating disorders and/or disordered eating symptoms.3 Bariatric surgery (BS) is the most effective treatment for weight loss, as it has exhibited consistent results when compared to lifestyle modification.4 The psychological consequences of bariatric surgery remain poorly understood despite the considerable incidence of psychological disorders among individuals considering this intervention. However, studies have revealed that patients experienced overall improvements in psychopathology, depressive symptoms, eating behavior, body image, and health-related quality of life following bariatric weight loss surgery.5 Furthermore, despite undisputed significant weight loss and improvements in comorbidities, a recent literature review has suggested several persisting disorders in psychological outcomes like depression and body image for patients at longer-term follow-ups.6 However, the onset of eating disorders after surgery remains poorly understood and under-reported. Accelerated weight loss, increased dietary restrictions, and frequent reminders to control food intake, which are critical for successful treatment, may lead to the development of eating disorders postoperatively.7 This study aimed to examine the occurrence of and factors contributing to disordered eating patterns in individuals who have undergone bariatric surgery. We also investigated the impact of these eating patterns on weight-loss outcomes and long-term weight management after surgery. In addition, this study sought to identify the psychological and emotional factors that contribute to the emergence of disordered eating patterns after surgery. Finally, it aimed to understand the relationship between dissatisfaction with body image and the development of disordered eating patterns in these individuals. A systematic review and meta-analysis of 7 studies revealed the prevalence of eating disorders in the postoperative period to be 7.83%. The most important factor, binge eating disorder, had a 3.81% prevalence and was identified in six of these investigations.8 In one case series, resemblances to typical EDs were observed. The characteristics that most differentiated these individuals from those with typical EDs were their current age and the age at which the ED first manifested in certain cases.7
Methods
Study design and inclusion and exclusion criteria
This cross-sectional study was conducted in multiple medical centers in Saudi Arabia between May 2022 and January 2023 to evaluate the prevalence of eating disorders and the levels of self-esteem among patients who had undergone bariatric surgery in the last five years. A total of 557 participants were enrolled in this study, and their responses were assessed using online self-administered questionnaires (via Google Forms) based on the DSM-5 criteria/ (PHQ-eating disorders) scale, which consists of 4 main parts: sociodemographic assessment, self-esteem assessment pre- and post-surgery, prevalence of positive and negative post-surgery psychological changes, and prevalence of bad eating habits during the last three months.
The inclusion criteria were as follows: patients older than 18 years, patients who had undergone bariatric surgery in the previous 5 years, and patients residing in Saudi Arabia. We excluded patient who were under 18 years of age. those who had undergone bariatric surgery more than 5 years ago, and patients outside the Kingdom of Saudi Arabia.
The Ethics Committee of Imam Mohammed Ibn Saud Islamic University approved this research project, and all participants provided institutional review board approval for the study (IRB number: 211/2022)
Questionnaire questions
In the self-administered questionnaires, sociodemographic questions assessed age, sex, nationality, place of residence, and educational level. The participants were asked about the type of bariatric surgery (gastric bypass, balloon surgery, BPD/DS, Sleeve gastrectomy) and if it was selective/obligatory or doctor’s advice, if the psychological assessment was necessary or elective before the surgery, and if they were properly assessed psychologically before surgery.
Regarding the psychological assessment pre- and post-surgery, participants were asked if they had been diagnosed with any psychological disorder. They were then assessed using the Rosenberg Self-esteem Scale before and after the surgery. Their current BMI was measured, and they were asked if they had experienced any positive or negative psychological changes after surgery.
To identify any bad habits formed during the last 3 months, the following questions were asked of all participants: “Did you have overeating episodes in which you ate huge amounts of food for 2 hours?”, “Did your overeating episodes occur twice a day?”, “Did feel out of control while eating during your overeating episodes?”, “Did you do anything to compensate for or prevent weight gain from overeating, such as vomiting, fasting, physical exercise practices , or taking laxatives, injections?”, “Did your body weight and shape affect how you felt about yourself?”, and “Did the overeating episodes only occur when you were below the optimal weight for your height?”
Statistical analysis
Descriptive data analysis was performed using SPSS software (V26, IBM, New York, U.S.). Data are reported as number and frequency or mean and standard deviation, as appropriate. For the self-esteem scale, the data were coded as follows: 1= Strongly Disagree, 2=Disagree, 3=Agree, and 4= Strongly Agree. Items 2, 5, 6, 8, and 9 were reversed. The sum of the scores for all 10 items was calculated, with higher scores indicating higher self-esteem. The Wilcoxon signed-rank test was used to compare the total scores before and after surgery. Statistical significance was set at p<0.05.
Results
Demographic characteristics of the included patients
Out of the 557 respondents, 452 met our inclusion criteria. Female sex was predominant (n= 275, 60.8%) compared to male sex (n=177, 39.2%). Most patients were between 18 and 35 years of age (n =314, 69.4%). A total of 95.8% of the patients had Saudi nationality. A total of 170 (37.6%) patients resided in the central region, 153 (33.8%) patients were in the western region, the eastern region included 76 individuals (16.8%), the southern region included 32 (7%) participants, and 21 (4.6%) participants resided in the northern region.
Two-thirds of the sample had bachelor’s degrees (n= 318, 70.4%), 18.6% (n=84) finished high school, and 11.1% (n=50) finished postgraduate studies (Table 1).
- Characteristics of patients.
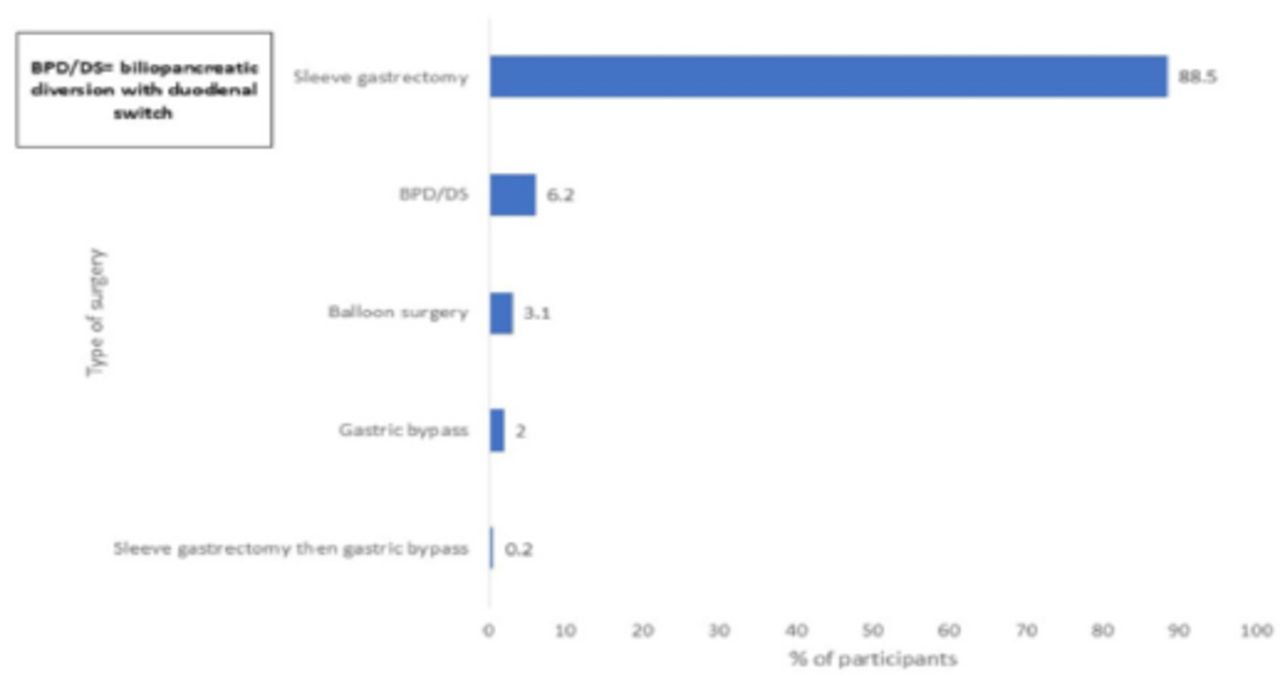
Most participants (n= 400, 88.5%) underwent sleeve gastrectomy. The BPD/DS was performed in 28 patients (6.2%), while balloon surgery and gastric bypass surgery were performed in 14 (3%) and nine (2%) participants, respectively. Only one patient underwent sleeve gastrectomy followed by gastric bypass (Figure 1).

- Type of surgery performed.
More than half of the participants (n=272, 60.2%) underwent selective surgery. However, 180 (39.8%) patients were either obliged or advised by a doctor. A total of 202 participants (44.7%) agreed on the necessity of psychological assessment before surgery, while only 163 (36.1%) had properly been assessed by their doctors. Table 1 summarizes the patient characteristics.
Prevalence of psychosocial disorders
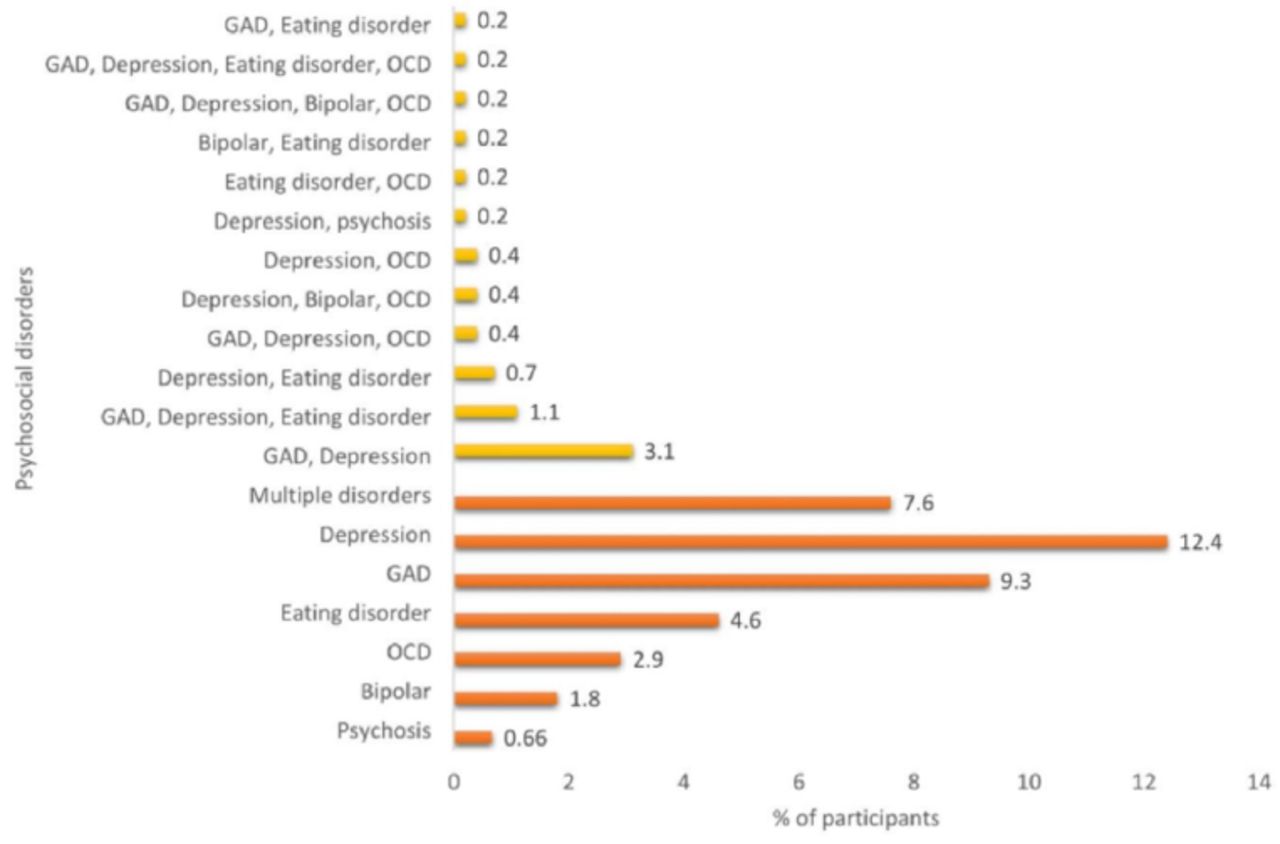
The prevalence of reported psychosocial disorders was 21.5% (N=97). Depression was the most frequently reported disorder (n=56, 12.4%), followed by GAD (n=42, 9.3%) and eating disorders (n=21, 4.6%). Bipolar and psychosis were the least reported psychosocial disorders and were identified in 1.8% and 0.66% of participants, respectively. Multiple disorders were reported in 34 patients (7.6%), the most common being depression with GAD in 14 patients (3.1%), and GAD, depression, and eating disorders coexisting in five patients (1.1%) (Figure 2).

- Frequencies of reported psychological disorders.
Effect of surgeries on self-esteem
Regarding the Rosenberg Self-esteem Scale, participants scored a mean score of 28.17±6.2 pre-surgery, which significantly increased to 31.7±5.3 post-surgery (p<0.001). Furthermore, all domains showed a significant increase after surgery. In terms of positive thinking questions, almost 94% of the participants were satisfied with themselves post-surgery compared with 54.7% preoperatively, and the mean score significantly increased from 2.64±1 3.57±0.6. A total of 54% of the participants thought that they had a number of good qualities, which increased to 95.3% after surgery, The mean score for recognizing personal qualities increased from 3.24±0.8 pre-surgery to 3.5±0.64 post-surgery.
After surgery, 93.2% and 86.5% of the participants thought they were able to do things as well as most other people, and felt as a person of worth, at least on an equal plane with others, respectively. Compared to 75% of the participants before surgery, 92.9% reported that they had a positive attitude toward themselves after surgery, increasing the mean score from 3.07±0.92 to 3.5±0.67. As to the questions about negative thinking, the percentage of participants who thought they were not good at all declined from 50.6% to 30.6%. There was a slight increase (from 62.6% to 72.3%) in participants who disagreed with feeling less proud. A total of 70.3% disagreed with feeling useless compared with 60.2% prior to the operation. Only 34.7% disagreed with the wish to have more respect for oneself compared to 25.7% before surgery. A decrease in the feeling of failure after surgery was reported (34.8% to 23%). (Table 2)
- Rosenberg self-esteem scale results before and after surgery.
- Positive and negative outcomes after the surgery.
- Prevalence of bad habits during the last three months.
Positive and negative outcomes
In terms of postoperative outcomes, 39 participants (8.6%) reported no changes. The most frequent positive outcome was increased self-esteem (81.4%), and more than half of the participants (56.6%) reported experiencing improved moods. Social openness were reported by 46% and improved relationship improvement with family and friends reported by 41% of the participants. Measured at only 25.4%, decreased anxiety was the least frequently recorded outcome. Mood deterioration and increased anxiety were the most frequently reported negative outcomes (10% and 9.5%, respectively). Withdrawal and social isolation occurred in 4.6% of the patients. Deterioration of relationships with family and friends was reported by 4.4% of the patients, while deterioration of relationships with partners was reported by 2.6% of the participants. Decrease in self-esteem was the least frequently reported outcome (1.8%). More than half of the participants had a normal BMI after surgery (58.4%), compared to 36.3% and 5.3% who showed high and low BMI, respectively.
A total of 103 patients (22.8%) reported overeating episodes in which they consumed large amounts of food for two hours. Of these 103, 98 experienced these episodes twice a day. A total 113 participants (25%) reported feeling out of control during their overeating episodes. More than half of the participants (59.15%) agreed that their body weight and shape affected their feelings toward themselves. A total of 145 participants (32.1%) reported vomiting, fasting, physical exercise, or taking laxatives and injections to compensate for or prevent weight gain from overeating episodes.
Discussion
Bariatric surgery is considered the treatment of choice for morbid obesity and the reduction of type 2 diabetes mellitus complication. Patients who had undergone bariatric surgery have been reported to exhibit symptoms of depression and eating disorders.9 Therefore, we aimed to measure the prevalence of psychological disorders among patients who had undergone bariatric surgery in the last five years. The current study showed a 21.5% prevalence rate of reported psychosocial disorders. This finding is consistent with the reported average prevalence of psychological disorders (20.9%) in Italy.10 A higher prevalence (55.5%) was estimated for bariatric surgery candidates in Germany.11
Depression was the most frequently reported disorder in our sample (12.4%), which was higher than the prevalence reported in an Italian sample (4.6%) and lower than that reported in a German sample (25.3%). The second most frequently reported disorder was any anxiety disorder (9.3%), which was lower than the prevalence reported in the Italian and German samples (12.4% and 15.1%, respectively). The third most common disorder in our sample was eating disorder (4.6%), lower than that in the Italian (7.1%) and German (37.7%) samples. The reported average prevalence of binge eating disorders ranges from 4% to 49%.12 According to a meta-analysis published in 2017, depression was the most common psychological disorder at the time of surgery (19%), followed by eating disorders (17%).13 Among the outcomes of bariatric surgery are that patients would experience improvements in shape and weight, and pooled results from a recent systematic review showed general improvements in certain aspects of body image with a mean follow-up duration of up to 48 months.14 Writing on quality of life after bariatric surgery, Sarwer et al. and Julia et al. reported a significant increase within 6 months post-surgery and up to 24 months post-surgery.15,16 Indeed, this improvement in weight, shape, and quality of life may in turn decrease psychological distress. A systematic review of 14 prospective studies published in 2019 revealed a significant reduction in the severity of depression and anxiety symptoms after two and three years post surgery.17
However, as evidenced by a systematic review on prolonged long-term follow-up, the achieved peak of higher quality of life declined by the fifth year after surgery.18 Furthermore, the presence of post-surgery eating disorders has been found to be associated with negative outcomes. In one study that aimed to assess pre- and post-surgery psychological profiles with long-term follow-up, psychological disorders, such as eating disorders, anxiety, and depression, were reduced after 23 months and then increased by 60 months, suggesting the need for a continuous long-term psychological evaluation and follow-up even after weight loss in high-risk patients.19 Furthermore, symptoms of OCD and depression have been posited as predictors of negative body image, self-efficacy, and body dissatisfaction in bariatric patients after surgery.20
Furthermore, the presence of depression or lower self-esteem in surgery candidates could serve as a predictor of poorer outcomes after the surgery, as found in a recent study prposing a model in which changes in depression symptoms, weight-related self-esteem, shape concerns, and weight concerns predict increases in weight loss one year after surgery.13 This study showed a significant improvement in mean self-esteem scores after surgery, with patients having high satisfaction with the current BMI. This is consistent with another cohort study that reported improvements in weight-related self-esteem from pre-surgery to 12 months after surgery.21
Changes in eating behaviors are very common after bariatric surgery; therefore, it is recommended that patients eat small meal portions, increase their water and vitamin intake, and avoid high-calorie and high-fat diets. Noncompliance has been reported as the most common obstacle following surgery. In our study, overeating episodes lasting two hours were reported by 22.8% with a frequency of two overeating episodes per day (21.7%). According to the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) criteria, those who have at least one overeating episode per week for three months, feel depressed or guilty after a binge, and lack control when overeating during binge can be diagnosed with binge eating disorder.22 The authors of a Swedish study investigated the effect of surgical treatment for weight loss and found a higher incidence of eating disorders and psychopathology in surgical groups compared to those who underwent nonsurgical treatments, except binge eating, which was equal in both groups, suggesting the importance of discussing these issues in surgical units.23 However, research has still found no significant risk factors associated with eating disorders, such as sex, age, or level of education. One study showed that women were more depressed, had lower self-esteem, and felt that weight interfered with their feeling good about themselves—factors associated with binge eating symptomatology. Conversely, in males, depression contributed to binge eating scores.24 Other eating disorder symptoms have emerged or been associated with surgery, including grazing, which has been identified as the continuous consumption of small amounts of food over an extended period of time. Colles et al25 suggested that preoperative grazing was associated with lower dietary restraint and hunger, with its prevalence increasing after surgery from 26.3% to 38.0%.25 Meanwhile, Saunders et al26 found that former binge eaters became grazers six months after surgery. In this study, other negative outcomes were reported by the participants, including mood deterioration, increased anxiety, withdrawal, and social isolation.
Our study had several limitations. Our questionnaire was a self-reporting survey, and we could not interview each participant to obtain a full diagnosis of their psychological disorders according to established guidelines and criteria. Self-reported weight evaluation surveys have been criticized for their inefficiency and tendency to underestimate the actual weight of patients with a high BMI.27 In terms of patient characteristics, female gender was more common than male gender (60.8% vs. 39.2%). This is a reliable difference since females are more likely to undergo bariatric surgery.28
In conclusion, patients who underwent bariatric surgery showed a mild prevalence of psychological disorders. However, a significant improvement in their mean self-esteem scores after bariatric surgery was noted. In addition to positive post-surgery outcomes, several negative outcomes and bad eating habits have been reported, supporting the association between psychological disorders and poor outcomes, not only in terms of weight loss but also the presence of bad eating habits. Long-term follow-up and continuous evaluation are highly recommended for patients with psychological disorders.
Acknowledgement
We would like to thank Enago, a member of Crimson Interactive Pvt. Ltd. for their assistance in language editing.
Footnotes
Disclosure. The authors declare no conflicting interests, support or funding from any drug company.
- Received August 13, 2024.
- Accepted November 5, 2024.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.