


ABSTRACT
Objectives: To describe age-standardized incidence and disability-adjusted life years (DALYs) of ischemic stroke (IS), intracerebral hemorrhage (ICH), and subarachnoid hemorrhage (SAH) in the Kingdom of Saudi Arabia (KSA) from 1990 to 2019 and forecast these variables using the Global Burden of Diseases (GBD) data over the next years (2020–2030).
Methods: Poisson regression models were employed to identify significant changes in incidence rate ratios (IRRs) and DALY rates for different stroke types. For time series models, the autoregressive integrated moving average (ARIMA) and exponential smoothing state space (ETS) models were used for forecasting.
Results: The study demonstrated an increasing trend in the age-standardized incidence rate per 100,000 different types of strokes over the last 30 years, with a slight decrease in ICH and SAH types in 2015, followed by a continued increase. The prediction models indicated a sustained increase in the 3 types of strokes, accompanied by a decrease in DALYs. As regards DALYs, the trend for IS and ICH has been slowly and steadily increasing; however, there will be a modest decrease in DALYs rates for SAH during the next decade.
Conclusion: Stroke rates in KSA have increased over 3 decades, mainly among women and older individuals, and have a slow sustained increase over the forecasted period (2020–2030); thus, proactive strategies and healthcare interventions are required.
Stroke, as defined by the World Health Organization (WHO), is characterized by sudden neurological symptomscaused by either blood flow blockage [ischemic stroke (IS)] or bleeding within the brain [intracerebral hemorrhage (ICH)]. Subarachnoid hemorrhage (SAH), a subtype of hemorrhagic stroke, is non-traumatic and occurs in the subarachnoid space.1 The Global Stroke Fact Sheet 2022 estimates that approximately 16% of stroke cases annually affect people aged 15–49 years, with over 60% affecting those under 70 years of age. Additionally, the incidence of stroke shows a gender disparity, being more prevalent among women (53%) than men (47%).2
Stroke contributes to high mortality and morbidity worldwide.3 Stroke is the second most common cause of death, following ischemic heart disease, and ranks third in disability. It is responsible for 11.6% of deaths worldwide and 5.7% of disability-adjusted life years (DALYs).4 Globally, stroke results in 6.5 million deaths per year, mainly among people under 70 years of age.2 In the Kingdom of Saudi Arabia (KSA), stroke is the second cause of mortality.5 The reported annual incidence varies significantly, ranging from 19 to 57 cases per 100,000 residents, with studies showing discrepancies in rates from 15.9 to 57.6 per 100,000 individuals.5 These differences have been attributed to unequal distribution of healthcare services, particularly between private and public sectors.6 The KSA also exhibits a relatively high stroke mortality rate of 27%, which exceeds that of other Middle Eastern countries, with IS representing the majority (79–87%).7 Although previous research has addressed the global burden of stroke, there is a critical need for region-specific analyses focusing on KSA while considering the various subtypes of stroke.8 Thus, this research aimed to determine the age-standardized incidence and DALYs of IS, ICH, and SAH in the KSA from 1990 to 2019 and forecast these variables using the Global Burden of Diseases (GBD) data over the next 11 years (2020–2030). The findings of this study would help healthcare authorities to plan and implement primary and secondary preventive strategies to reduce stroke-related morbidity, disability, and mortality.
Methods
A descriptive epidemiological study followed by trend analysis and forecasting were performed using the data from the GBD database, conducted by the Institute for Health Metrics and Evaluation (IHME), which is recognized globally for its comprehensive approach to quantifying health trends. This database employs rigorous methodologies, including systematic reviews, expert consultations, and advanced statistical techniques, ensuring high-quality data.9 The timeframe sample size was used to cover over 30 years from 1990 to 2019 in KSA and include all stroke incidence cases and DALYs in various stroke types, covering various health indicators and deaths.3 Stroke was identified and classified according to the clinical criteria established by the WHO.2 Approval of the study was obtained from the Ethics Committee of King Khalid University, KSA (ECM#2024-309).
Age-standardized values were utilized to represent stroke incidence rates, adjusted for age distribution. The median was used to present the total number of cases and DALYs. Differences in stroke incidence based on age and sex were analyzed using the Kruskal–Wallis test. Trends for incidence and DALYs were illustrated across 5-year age groups and by sex. Poisson regression models were conducted to identify significant variations in incidence rate ratios (IRRs) and DALY rates for the different types of strokes, with separate models created to consider sex or age groups as predictors. The DALYs were calculated by determining years of life lost due to death and years lived with disability. A significance level of p<0.05 and a 95% confidence interval were applied. The linearity of time series and forecasting models was assessed visually by inspection, while residual normality was checked via the Kolmogorov–Smirnov test. Autocorrelation was evaluated using the autocorrelation function (ACF) and the Ljung–Box test, stationarity was determined with the Kwiatkowski–Phillips–Schmidt–Shin (KPSS) test, and zero mean was assessed using a one-sample t-test. Validation involved a train-test split to compare predicted and actual values. For time series models showing significant results in the Ljung–Box test, KPSS test, and autocorrelation, autoregressive integrated moving average (ARIMA), time series regression, or exponential smoothing state space (ETS) models were employed to identify the best-fitting model. The analysis took into account the autoregression order (AR (p)), moving average order (MA (q)), and degree of differencing (I(d)). The optimal model was selected based on goodness of fit, indicated by the coefficient of determination, Akaike’s information criterion (AIC), and mean square error. Prediction models were developed to estimate stroke incidence rates and DALYs for various stroke types. Data analyses were conducted using R version 4.3.2.
Results
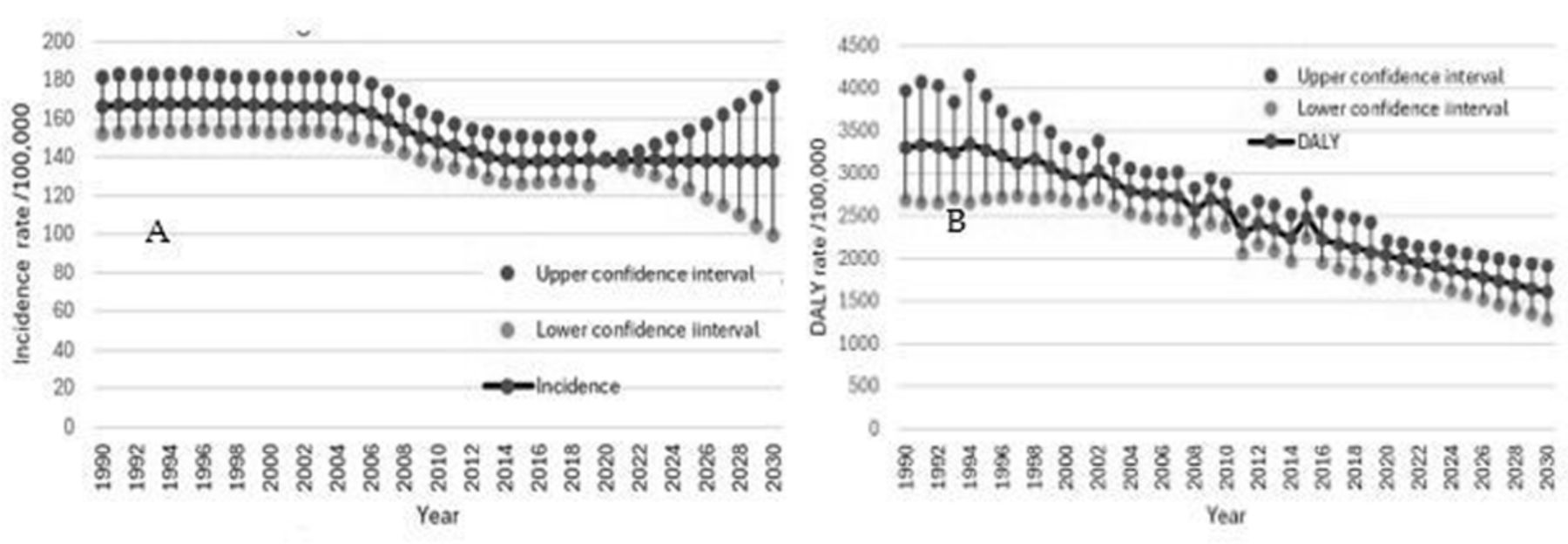
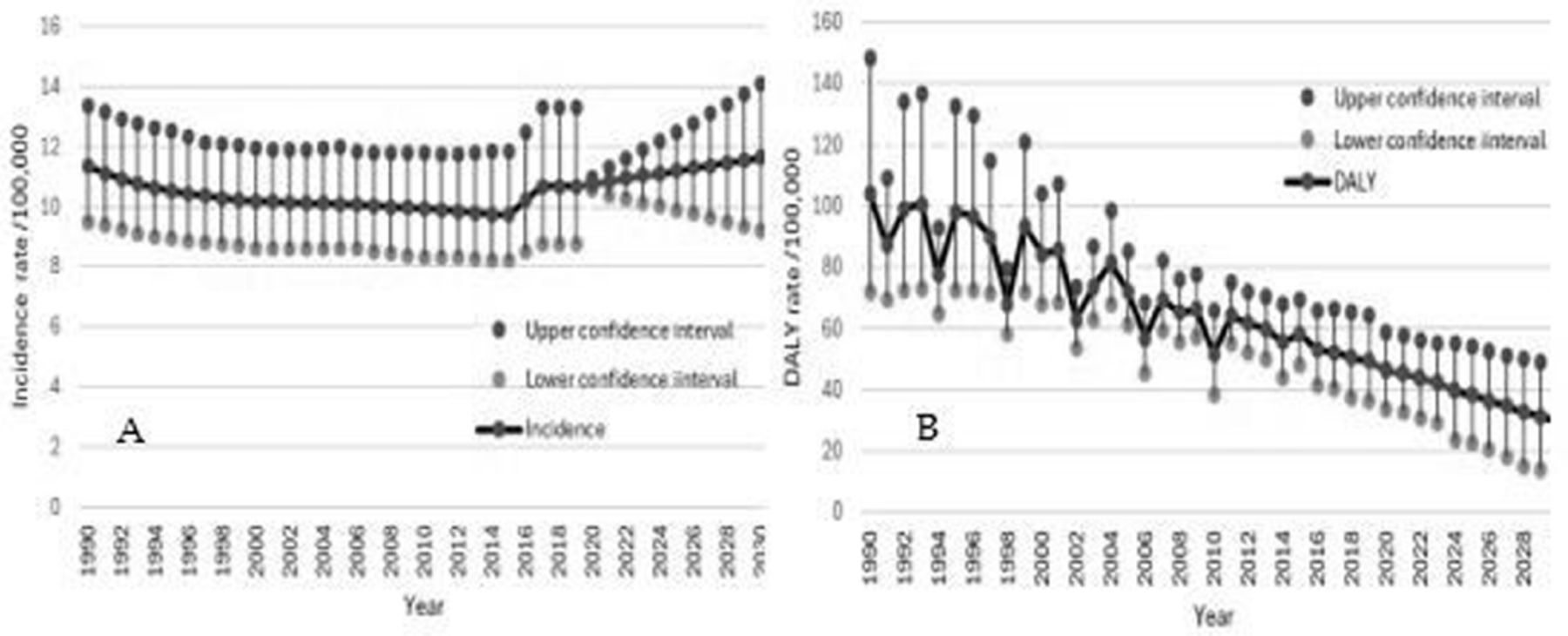
The age-standardized incidence rate (ASIR) of overall stroke, including IS, ICH, and, SAH, decreased from 2006 to 2019. The ARIMA model2,2,1 was selected as the best-fitting model for forecasting based on the non-significant Ljung–Box test (p=0.208) and the ACF plot, which showed no autocorrelation. This model includes two autoregressive terms (AR=2), indicates the series has been differenced twice to achieve stationarity (I=2), and incorporates one moving average term (MA=1). Further, it predicts that this decreasing trend will continue until 2030 (Figure 1).

- Age-standardized incidence rates and DALYs of overall strokes, including subarachnoid hemorrhage, intracranial hemorrhage, and ischemic stroke.
The age-standardized disability rates (ASDR) of overall stroke, including IS, ICH, and SAH, decreased from 1994 to 2019. The ARIMA model (2,1,0) was selected as the best-fitting model for forecasting based on the non-significant Ljung–Box test (p=0.877) and the ACF plot, which showed no autocorrelation. This model includes 2 autoregressive terms (AR=2), indicates the series has been differenced once to achieve stationarity (I=1), and incorporates no moving average terms (MA=0). Further, it predicts that this decreasing trend will continue until 2030 (Figure 1).
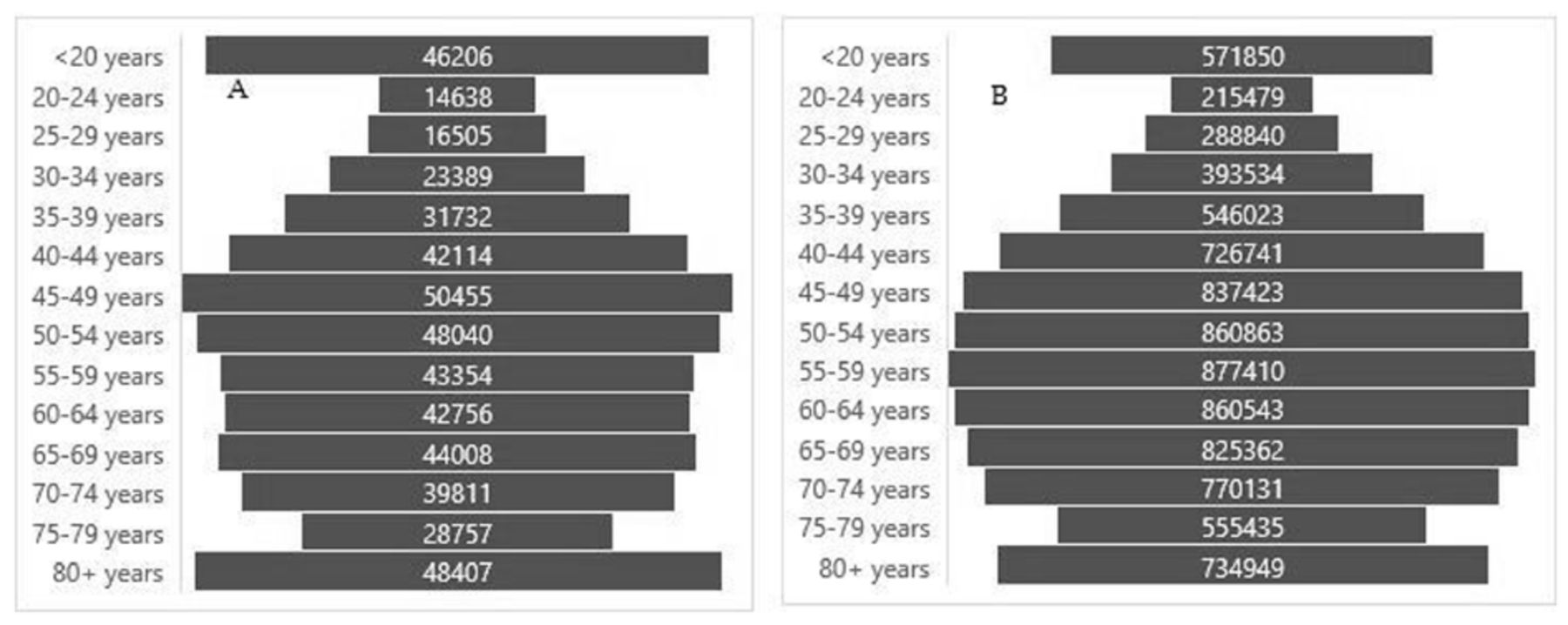
The overall stroke showed the highest incidence number in the age group (<20 years), which could be explained by the highest incidence of subarachnoid stroke in this age group. The highest DALYs were reported in the age group (55–59 years) (Figure 2).

- Shows A) Incidence number of the overall strokes, B) DALYs number of the overall strokes.
The incidence of IS from 1990 to 2019 was described using the median and was stratified according to age group and sex. The Kruskal–Wallis test revealed a significant difference in the median incidence of IS between different age groups (p<0.001). In contrast, there were insignificant sex differences in the incidence of IS (p=0.072) (Table 1).
- The number of age-adjusted different pathological types of strokes across different ages and sex.
The Poisson model illustrated that the IS incidence rate per 100,000 was higher in females than males (1.21, 95% CI, 1.16-1.26; p<0.001).
The Poisson model revealed significant increases in IRRs when comparing the <20 years age group, used as the reference group, to different age groups. The IRRs for the +80, 75–79, 70–74, 65–69, 55–60, 50–54, 45–49, 40–44, 35–39, 30–34, and 25–29 years age groups were 111.19 (95% CI: 103.14–120.11), 76.32 (95% CI: 70.78–82.45), 67.46 (95% CI: 62.56–72.89), 55.10 (95% CI: 51.09–59.53), 39.22 (95% CI: 36.36–42.39), 26.54 (95% CI: 24.59–28.70), 17.04 (95% CI: 15.78–18.44), 10.26 (95% CI: 9.48–11.12), 6.20 (95% CI: 5.72–6.73), 3.50 (95% CI: 3.22–3.82), 2.17 (95% CI: 1.98–2.38), and 1.30 (95% CI: 1.17–1.43), (p<0.001), respectively. The 20–24 years age group showed a significant decrease compared to the <20 years group with an IRR of 0.89 (95% CI: 0.79–0.99) (p=0.03).
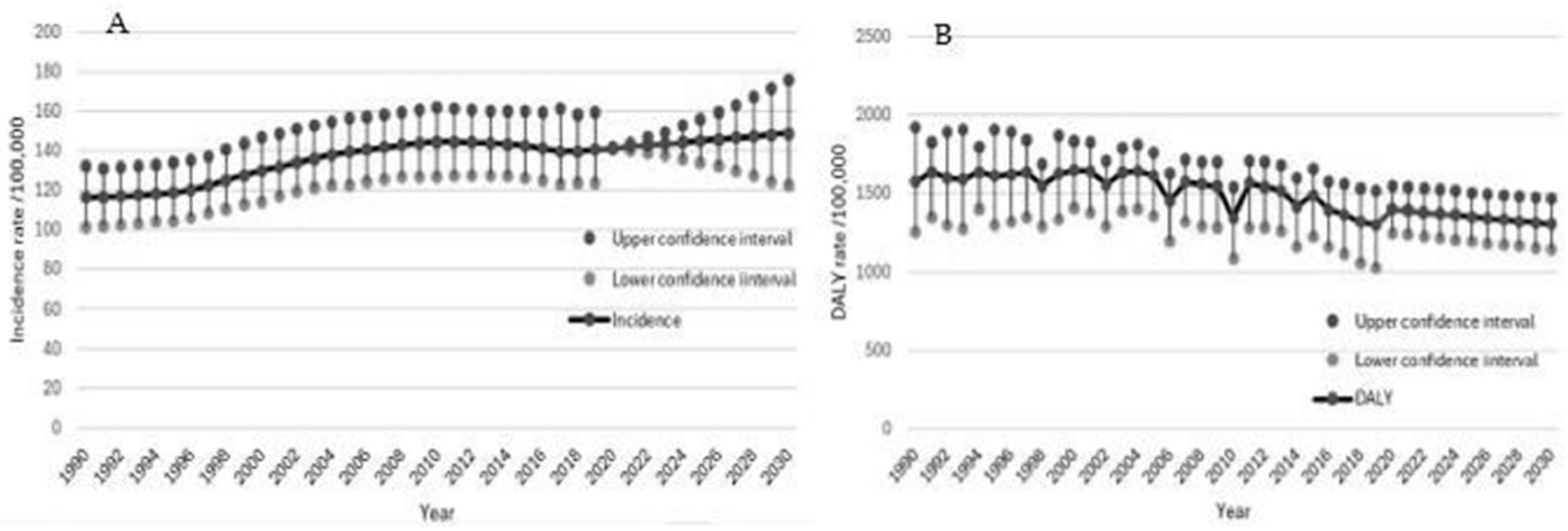
The incidence of IS showed a sustained increase from 1990 to 2014, followed by a plateau from 2014 to 2019. The most fitted model for forecasting the IS incidence rate till 2030 was ARIMA (0,2,1), selected based on the non-significant Ljung–Box test (p=0.996), no autocorrelation, and the lowest AIC=14.34 compared to the non-ARIMA model. The ARIMA model had moving average coefficients of 0.85 (95% CI: 0.58–1.12, p<0.001). The model indicates a systematic linear increase in the trend of IS incidence rate by 2030 (Figure 3).The Poisson model illustrated that the stroke DALYs per 100,000 in females were higher than males, with an IRR of 1.08 (95% CI: 1.07–1.09), (p<0.001).

- The forecasted incidence rate A) and DALYs B) of ischemic stroke in the Kingdom of Saudi Arabia between 2020 and 2030.
The Poisson model found significant increases in DALYs per 100,000 in the different age groups when compared to the reference group (<20 years). Specifically, the DALYS for the +80, 75–79, 70–74, 65–69, 55–60, 50–54, 45–49, 40–44, 35–39, 30–34, 25–29, and 20–24 years age groups were 754.09 (95% CI: 719.44–791.00), 493.61 (95% CI: 470.93–517.78), 346.43 (95% CI: 330.50–363.39), 225.12 (95% CI: 214.76–236.15), 152.27 (95% CI: 145.25–159.74), 76.28 (95% CI: 72.75–80.03), 48.47 (95% CI: 46.22–50.87), 27.37 (95% CI: 26.43–29.11), 16.53 (95% CI: 15.75–17.36), 9.44 (95% CI: 8.98–9.92), 5.37 (95% CI: 5.10–5.66), 3.51 (95% CI: 3.33–3.71), and 2.76 (95% CI: 2.61–2.92)], (p<0.001), respectively.
The ASDR of IS showed a decrease over the years from 1990 to 2019. The best-fitted model for DALYs of IS was the time series regression model, the simplest form of the time series models, where the dependent variable was the DALYs rates and the independent variable was time. This model was selected based on the non-significant Ljung–Box test (p=0.166), and the ACF plot represented no autocorrelation. Each passing year decreases DALYs significantly by -9.28 (95% CI: -12.26–6.31, p<0.001) (Figure 3). Significant differences in incidence rates were detected between different age groups and sexes (p<0.001) (Table 1).
The Poisson model revealed that the incidence rate of ICH per 100,000 showed insignificant sex differences, with an IRR of 1.01 (95% CI: 0.94–1.09), (p=0.800).
Using the Poisson model, the present study reported significant increases in ICH IRR per 100,000 in the +80, 75–79, 70–74, 65–69, 55–60, 50–54, 45–49, 40–44, 35–39, 30–34, 25–29, and 20–24 years age groups compared to the <20 years age group, with the values being 95.39 (95% CI: 85.05–107.47), 53.63 (95% CI: 47.79–60.45), 42.66 (95% CI: 38.01–48.10), 33.74 (95% CI: 30.05–38.06), 26.86 (95% CI: 23.91–30.31), 21.21 (95% CI: 18.87–23.95), 16.80 (95% CI: 14.94–18.98), 12.13 (95% CI: 10.77–13.72), 7.19 (95% CI: 6.36–8.16), 4.03 (95% CI: 3.54–4.60), 2.64 (95% CI: 2.31–3.04), 1.83 (95% CI: 1.59–2.12), and 1.59 (95% CI: 1.37–1.84), (p<0.001), respectively.
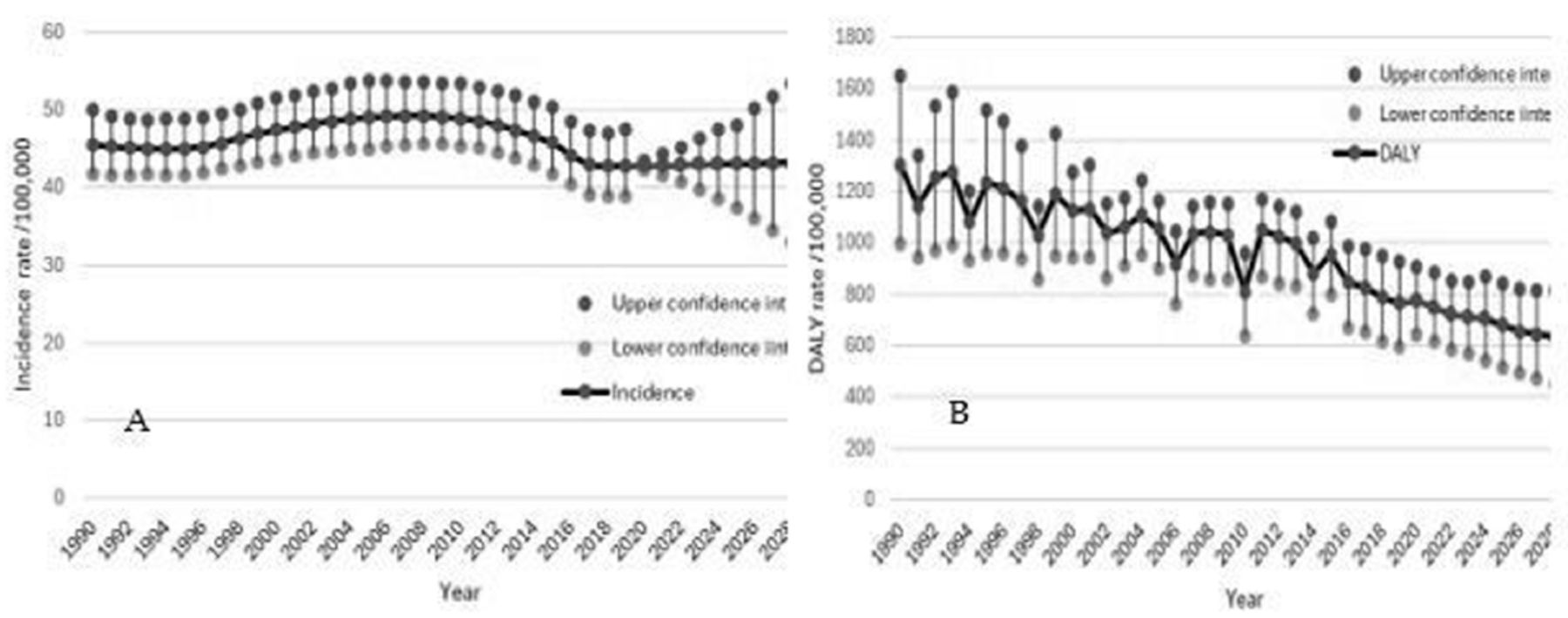
The trend of ICH increased from 2000 to 2012, then decreased until 2016, after which it plateaued. The most fitted model for forecasting intracranial hemorrhage stroke incidence rate was ETS (A,A,N), exponential smoothing with additive errors for both the level (l) and the trend (b), with no seasonal component. The model selection was based on a non-significant Ljung–Box test (p=0.560), no autocorrelation according to ACF, and the lowest AIC= 48.94 compared to the ARIMA model, which represented autocorrelation according to ACF. The initial level (l) was 45.8286 and the initial trend (b) was -0.2896. The model suggests a slight increase in the hemorrhagic stroke incidence rate trend.
The Poisson model revealed that DALYs of ICH per 100,000 in females were significantly higher than in males, with an IRR of 1.03 (95% CI: 1.02–1.05), (p<0.001).
Using the Poisson model illustrated significant increases in ICH DALYs per 100,000 in the +80, 75–79, 70–74, 65–69, 55–60, 50–54, 45–49, 40–44, 35–39, 30–34, 25–29, and 20–24 years age groups when compared to the <20 years age group, with the values being 181.57 (95% CI: 173.85–189.75), 168.63 (95% CI: 161.46–176.23), 146.73 (95% CI: 140.48–153.34), 141.42 (95% CI: 135.41–147.80), 105.78 (95% CI: 101.27–110.56), 88.60 (95% CI: 84.82–92.60), 60.90 (95% CI: 58.30–63.66), 40.67 (95% CI: 38.92–42.52), 25.37 (95% CI: 24.28–26.54), 13.81 (95% CI: 13.20–14.45), 7.59 (95% CI: 7.25–7.95), 5.75 (95% CI: 5.48–6.03), and 3.96 (95% CI: 3.77–4.16)], (p<0.001), respectively.
The ASDR of hemorrhagic stroke showed a sustained decrease from 1990 to 2019. The ARIMA (3,1,0) was the most fitted model to forecast ICH stroke with autoregressive components, AR1=-1 (95% CI: -1.28–-0.73), AR2=-0.9 (95% CI: -1.22–-0.59), AR3=-0.61 (95% CI: -0.88–-0.34), and drift =-16.68 (95% CI: -23.56–-9.80). This model was selected based on the non-significant Ljung–Box test (p=0.928), the absence of autocorrelation based on ACF, and the lowest AIC. The model suggested a sustained decrease in DALYs (Figure 4).

- Forecasted incidence rate A) and DALYs B) of intracranial hemorrhage stroke in Saudi Arabia (2020–2030).
A significant difference was found among the various age groups (p<0.001, while there was an insignificant sex difference between males and females in SAH stroke (p=0.060) (Table 1).
The poisson model showed that the incidence of SAH stroke per 100,000 in women was significantly higher than in men, with an IRR of 1.35 (95% CI: 1.15–1.58, p<0.001).
The Poisson model revealed significant increases in the IRR of SAH per 100,000 in the +80, 75–79 years, 70–74, 65–69, 55–60, 50–54, 45–49, 40–44, 35–39, 30–34, 25–29, and 20–24 years age groups than the reference group (<20 years), with the values being 33.13 (95% CI: 26.45–42.21), 27.15 (95% CI: 21.66–34.62), 29.12 (95% CI: 23.24–37.12), 27.89 (95% CI: 22.25–35.56), 23.46 (95% CI: 18.70–29.93), 20.08 (95% CI: 15.99–25.64), 17.77 (95% CI: 14.14–22.70), 15.43 (95% CI: 12.26–19.73), 13.06 (95% CI: 10.37–16.72), 9.88 (95% CI: 7.82–12.68), 5.88( 95% CI: 4.62–7.60), 3.29 (95% CI: 2.55–4.31), and 2.11 (95% CI: 1.60–2.80), (p<0.001), respectively.
The trend of SAH stroke incidence decreased from 1990 to 2002, remained stable until 2015, and then increased until 2019. The most fitted model for forecasting the SAH stroke incidence rate was ARIMA (0,2,2), with the moving average MA1=0.10 (95% CI: -0.19–0.40, p=0.487) and the second moving average MA2=-0.74 (95% CI: -1.03–-0.45, p<0.001). The model was selected based on the insignificant Ljung–Box test (p=0.849), the absence of autocorrelation, and the lowest AIC. MA1 and MA2 suggest that the current observation is influenced by the first and second lags of the error term. This model indicates an increasing trend in the subarachnoid hemorrhage incidence rate (Figure 5). The Poisson model revealed that the SAH stroke incidence rate per 100,000 was higher in females than males, with an IRR of 1.65 (95% CI: 1.56–1.75, p<0.001).

- Forecasted subarachnoid hemorrhage incidence rate A) and DALYs B) in the Kingdom of Saudi Arabia (2020–2030).
Using the Poisson model, there were significant increases in DALY of SAH per 100,000 in the +80, 75–79, 70–74, 65–69, 55–60, 50–54, 45–49, 40–44, 35–39, 30–34, 25–29, and 20–24 years age groups compared to the <20 years age group, with the values being 22.79 (95% CI: 20.50–25.42), 21.02 (95% CI: 18.91–23.45), 22.14 (95% CI: 19.92–24.70), 17.26 (95% CI: 15.52–19.27), 12.61 (95% CI: 11.33–14.09), 14.19 (95% CI: 12.75–15.85), 11.25 (95% CI: 10.10–12.58), 9.42 (95% CI: 8.44–10.54), 11.79 (95% CI: 10.58-13.18), 7.55 (95% CI: 6.76–8.46), 4.54 (95% CI: 4.05–5.11), 2.89 (95% CI: 2.56–3.27), and 2.11 (95% CI: 1.86–2.40), (p<0.001), respectively.
The ASDR of SAH showed a sustained decrease from 1990 to 2019. The most fitted model to forecast subarachnoid hemorrhage DALYs until 2030 was selected based on the non-significant Ljung–Box test (p=0.670), the absence of autocorrelation, and the lowest AIC. ARIMA (3,1,0) was the best-fitted model with AR1=-1.07 (95% CI:-1.30–-0.84, p<0.001), AR2 =-1 (95% CI: -1.25–-0.74, p<0.001), and AR3=-0.72 (95% CI: -0.94–-0.51, p<0.001). The negative drift coefficient of -1.67 (95% CI: -2.36–-1.16, p<0.001) suggests a systematic linear decrease in the trend of SAH DALYs until 2030 (Figure 5).
Discussion
This study in KSA aims to assess the burden of various stroke types by examining incidence, ASIR, and ASDR from 1990 to 2019, while also projecting trends in incidence and DALY rates for stroke subtypes from 2020 to 2030. Consistent with our findings, earlier studies9,10 reported a rise in the ASIR of IS between 1990 and 2010. The observed increase in IS incidence in KSA during this period (programs) is likely attributable to implementing early detection and diagnosis. The increasing trend in ASIR since 1990 underscores the importance of sustaining public health policies focused on stroke prevention and early detection. However, previous studies conducted in China, the United States (US), and globally reported a continuous decline in ASIR of overall stoke and IS from 1990- 2019.11-13 This discrepancy between the studies could be attributed to the difference in IS detection and preventive methods.
Regarding disability, our findings are in the same line with previous studies12,13 which revealed a global decrease in overall stroke and stroke type-standardized DALYs rates. In the Middle East and North Africa (MENA) region,3 regional ASDR has decreased since 1990 and placed KSA, Lebanon, and Kuwait with the lowest DALYs rates, which was attributed to advancements in managing stroke-related consequences. Conversely, Afghanistan, Iraq, and Yemen had the highest ASDR which was attributed to lower access to preventive and acute stroke care in these countries.
Another finding of the current study showed that the ASDR of IS trended upward before 2010 and then trended downward after 2010. This points to better stroke care in KSA after the prevalent administration of recombinant tissue plasminogen activator (rTPA).14 Moreover, different management approaches that incorporate innovative home-based methods as telerehabilitation, robotic devices, virtual reality tools,15 and self-management, improve rehabilitative services and outcomes.16 Similarly, a prior MENA study discussed the ASDR of the total stroke and found that Kuwait faced an upward trend before 2010 and a downward trend after 2010.9 Another study discussed the global burden of IS and found greater IS-standardized DALY rates in high socio-demographic index (SDI) regions than in other SDI regions.10 This could be explained that higher SDI may cause a sedentary lifestyle and speeding IS risk factors.
The present study identified a statistically significant rise in IS incidence with increasing age, consistent with findings from previous research.9,10,13,17,18 While population growth and demographic shifts were primary drivers of this trend, insufficient lifestyle modification initiatives, and education, contributing to a high prevalence of risk factors such as tobacco use and diabetes, may have further exacerbated these patterns in the MENA region.19,20 Aging usually is associated with neurovascular unit (NVU) dysfunction, intensifying cerebral injury progression through mechanisms including disruption of the blood-brain barrier (BBB), neuronal cell death, and infiltration of immune cells.21,22 Another study also showed that the IRR for IS was highest among individuals aged 65–69, 80–84, and 70–74.18 Similarly, another study reported the highest IS incidence in the 80–84 age group, with a gradual increase observed in the 50–69 and 70+ age groups.11 These findings underscore the role of age as a relevant risk factor for stroke. On the contrary, studies from the MENA region3 and the US12 that focused on the overall stroke burden indicated that stroke burden increased in younger persons.
Regarding sex, previous studies10,17 aligned with our findings and showed female predominance in IS. Female patients have worse outcomes and higher comorbidities, which lowers their survival.23 Thus, KSA should implement sex-specific stroke prevention and post-morbid treatment, especially IS. Additionally, higher ASDR levels were observed in females, a finding consistent with previous MENA research.24 Conversely, a previous study found that men had a higher ASDR than women from 1990 to 2019.25
Another finding of the Poisson model of the present study is the increase in ASDR of IS per 100,000 for older individuals (≥80, (75-79), (70-74), (65-69), and (60-64) than younger individuals (<20 years old). Similarly, the elevated age-standardized DALY rates for IS among older ages were confirmed by another research using GBD data10 and the MENA study.9 On the contrary, a previous study found a decrease in all age-standardized DALY rates for overall stroke types.18 Thus, future research is necessary to evaluate the effect of aging on IS-standardized DALY rates in KSA.
This study found that the ASIR of ICH increased until 2010 and trended downward after 2010. However, the ASIR of SAH trended downward until 2015 and then increased. This downward trend of hemorrhagic stroke could be explained by the fact that following the 2011 global health agenda, KSA has improved stroke prevention and risk factor modification programs.9 Moreover, neurocritical care services, such as treating surgical hematoma and ruptured intracranial aneurysms have improved which lower sits mortality-related rates. In contrast, previous findings showed that age-standardized ICH stroke and SAH incidence rates constantly declined over 30 years.9,26 The discrepancy could be attributed to the difference in the preventive and detection methods of hemorrhagic stroke globally.
The age-standardized analysis revealed that the highest median incidence of ICH stroke occurred in the age groups <20, 45–49, 50–54, and 55–59. A prior MENA study3 noted a higher stroke burden among younger populations in the region compared to global trends. These findings align with earlier research on overall stroke burden,12,27 which highlighted the prevalence of cardiovascular risk factors in younger and middle-aged individuals. This underscores the need for increased efforts from Saudi public health authorities to address the growing incidence of ICH among younger and middle-aged populations. In contrast, a previous study observed that total hemorrhagic stroke incidence peaked in the 65–69, 80–84, and 70–74 age groups.18 Additionally, Xia et al28 found the peak incidence of ICH to occur at 55–59 years for men and 60–64 years for women.28
In agreement with the Poisson model of the current findings, a previous study found a higher DALY rate of ICH among age subgroups 85 years old or older.11 In addition, another study found the rate of DALYs peaked at the ages of 75–79 years in 1990, while in 2019, the rate of DALYs peaked at the ages of 85–89 years.27 This finding underscore the importance of assessing the impact of ICH on the DALY rate over time.
In agreement with our findings, previous studies have reported higher ICH incidence and standardized incidence rates in men compared to women.28,29 Hormonal, social, and lifestyle factors may contribute to these gender disparities and should be further investigated to understand the underlying factors that make certain genders more susceptible to ICH. However, our study revealed that the ASDR for ICH was higher in women as compared to men, which contrasts with a previous study.28 This discrepancy may be attributed to regional and cultural differences and higher rates of comorbidities among women.
Furthermore, our study found that the IRR and DALY rates for SAH were highest in the age groups ≥80, 75–79, and 65–69, which aligns with earlier research.11,18 As standardized DALY rates reflect the overall burden of stroke, further studies in KSA are essential to monitor these trends over time.
Another finding of the current study, the ASIR of SAH was significantly greater in women than in men, which is consistent with a prior USA study.28 The possible explanation includes hormonal factors, particularly hormone replacement treatment.29,30 These results underscore the significance of age and gender as pivotal variables in comprehending the burden of stroke.
To effectively plan for infrastructure changes, it is essential to predict stroke incidence. A key finding of this study is the projection of stroke-type incidence and DALY rates for the next 11 years. Our analysis revealed that ASIR for all stroke types is expected to increase gradually from 2020 to 2030. Similarly, a previous study in KSA indicated a rise in total stroke incidence over the coming decade.31 Another study also forecasted an increase in IS incidence across all age groups and SDI quintiles between 2020 and 2030.32 This rise is likely driven by increased exposure to metabolic risk factors such as hypertension and diabetes,33,34 alongside improvements in detection and diagnostic capabilities, which may lead to higher reported ASIR for stroke. Therefore, effective prevention of IS requires addressing these risk factors.35 Additionally, a European study found trends similar to ours in the broader stroke category.36 In contrast, a previous study forecasted a more stable, modest ASIR trend over the next 25 years.18
In terms of ASDR, our study showed a slow, sustained decrease for both IS and hemorrhagic strokes over the next eleven years. This trend aligns with findings by Pu et al.,32 who reported a global decline in IS DALY rates, although countries with lower SDI, such as Senegal and Ecuador, experienced the fastest increases in DALY rates. The predicted decrease in DALY rates in KSA suggests potential improvements in post-stroke care in the coming decade.
A final novel finding of this study is the projected slow decrease in ASDR for both IS and hemorrhagic strokes over the next eleven years. This trend mirrors global observations by Pu et al,32 with notable increases in DALY rates in low-SDI countries. The decline in ASDR indicates potential progress in post-stroke care in KSA, highlighting the importance of continued prevention and treatment initiatives.
This study has crucial implications for global, regional, and national assessments of stroke burden, as well as for predicting future trends in stroke types. These findings will assist policymakers in addressing the rising stroke burden in KSA, guiding resource allocation, healthcare planning, and the development of effective prevention and detection strategies.
Limitations
This study also had several limitations, such as its reliance on secondary data from GBD, which may contain missing or incomplete data. Additionally, there is scarcity of studies exploring the expected patterns of a broad category of strokes over the next ten years, and it did not consider possible stroke risk factors, which require further study in the future.
Conclusions
Between 1990 and 2019, the current study found that the incidence of IS and hemorrhagic strokes in KSA increased. The ASIR and ASDR of overall stroke showed a downward trend after 2010. The ASIR of IS and SAH was significantly female predominance, while the ASIR of ICH was significantly higher in men. Also, the ASIR for strokes in general showed a slow sustained increase over the forecasted period (2020–2030). However, ASDR of IS, ICH, and SAH showed a slow sustained decrease for 2020- 2030. As a result, we urge that evidence-based interventions be considered in the next few years to minimize the burden of different forms of stroke in KSA. Also, we recommend public health strategies to target the risky groups of different strokes in the future.
Acknowledgement
We would like to extend our appreciation to the Deanship of Research and Graduate Studies at King Khalid University for funding this work through a Large Research Project under grant number RGP2/440/45.
Footnotes
Disclosure. This study was funded by the Deanship of Research and Graduate Studies at King Khalid University, Abha, Kingdom of Saudi Arabia grant number RGP2/440/45.
- Received August 19, 2024.
- Accepted December 9, 2024.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.