


ABSTRACT
Objectives: To examine the association between sleep deprivation and cigarette smoking among adolescents in the “Gulf Cooperation Council (GCC)” countries, accounting for relevant sociodemographic and behavioral factors.
Methods: The present study was conducted between June and August 2024 using data from the most recent “Global School-based Student Health Survey (GSHS)” conducted in 5 GCC countries. The study included 21,105 adolescents aged 11–18 years. Multiple logistic regression models were used to examine the association in each country. A random-effects meta-analysis was conducted to synthesize results across countries.
Results: Overall, 17.9% of adolescents reported sleep deprivation. The pooled adjusted odds ratio for the association between cigarette smoking and sleep deprivation was 1.75 (95% CI: 1.56–1.96), indicating that adolescents who smoked cigarettes had 75% higher odds of experiencing sleep deprivation compared to non-smokers. This association was consistent across all 5 GCC countries, with low heterogeneity (I² = 18.1%).
Conclusion: This study provides evidence of a significant positive association between sleep deprivation and cigarette smoking among adolescents in GCC countries. These findings emphasize the need for comprehensive public health interventions promoting both smoking prevention and sleep health among adolescents in the region.
Sleep is a crucial component of human health and well-being, particularly during adolescence when rapid physical, cognitive, and social-emotional development occurs.1 Adequate, high-quality sleep is essential for promoting physical and mental well-being in young people.2 Sleep deprivation among youth is a growing public health issue worldwide, with potential long-term consequences for academic performance, physical and mental health, and overall quality of life.3, 4 The prevalence of sleep deprivation in adolescents has been increasing globally, especially with the common use of digital devices and social media.2
Tobacco use, including cigarette smoking, is a substantial public health concern globally, and its prevalence remains high among adolescent populations.5 Previous research has linked tobacco use to various adverse health consequences, including respiratory issues, cardiovascular problems, and mental health disorders.6 Importantly, tobacco use has been associated with sleep disturbances, including difficulties in sleep initiation, disrupted sleep, daytime drowsiness, and overall poor sleep quality.7
The potential mechanisms underlying the relationship between tobacco use and sleep impairment are complex and not well understood. Nicotine, the primary psychoactive element in tobacco products, is a stimulant that can disrupt the body’s natural sleep-wake cycles.8 Additionally, the associations between tobacco use and other lifestyle factors, such as increased stress, sedentary behavior, and poor diet, may indirectly influence sleep patterns in adolescent population.9,10
Investigating the impact of tobacco use on sleep quality among adolescents in the “Gulf Cooperation Council (GCC)” countries is particularly important, as these countries have underwent rapid social and economic changes in recent decades.11,12,13 Such changes, including urbanization and technological advancements, can impact the health-related behavior and sleep patterns of young populations.14,15 In addition, tobacco use still constitutes a huge burden in GCC countries16,17 despite a long history of control efforts.11 However, research on sleep deprivation among adolescents in this region remains limited. The GCC countries—comprising Bahrain, Kuwait, Oman, Qatar, Saudi Arabia, and the United Arab Emirates (UAE)—share cultural, economic, and political ties. Therefore, understanding the regional patterns of tobacco use and its implications for adolescent sleep can inform targeted public health interventions and policies.
The GCC countries have implemented various tobacco control measures, including smokefree policies in public places, health warnings on tobacco products, and increased taxation.11 However, comprehensive policies specifically targeting adolescent smoking or addressing sleep health among youth are limited in the region. Cultural factors unique to the GCC region may influence both smoking behaviors and sleep patterns among adolescents. These include late-night social gatherings as a cultural norm, extended family living arrangements, and gender-specific social expectations. Additionally, the rapid socioeconomic changes in GCC countries have led to increased access to digital devices and social media, potentially affecting both smoking behaviors and sleep quality among adolescents.14,15
This study aimed to comprehensively examine the relationship between tobacco consumption and sleep quality among adolescents in the GCC countries, accounting for relevant sociodemographic and behavioral factors. The results from this study can add to the growing evidence on the impact of tobacco use on adolescent health, with significant implications for the health promotion strategies and policies in the region.
Methods
Study design
This study was conducted between June and August 2024 utilizing data from the most recent “Global School-based Student Health Survey” (GSHS) conducted in each of the GCC countries: “Bahrain (2016), Kuwait (2015), Oman (2015), Qatar (2011), and the UAE (2016)”. Saudi Arabia was excluded because GSHS data were not available. The GSHS is a standardized, cross-sectional survey developed by the “World Health Organization” (WHO) to assess various health-related behaviors and risk factors among school-attending adolescents.18 The GSHS utilizes a “two-stage cluster sampling design”. First, schools were selected using the “probability proportional size” approach. Classes were randomly chosen from these schools and all students were invited to participate.
The study population comprised school-going adolescents aged 11–18 years from the GCC countries. Students in grades equivalent to 8-12 (or the country-specific equivalent) were included in the survey.
Measures
The GSHS questions used in data collection have been validated in previous studies across diverse cultural contexts including GCC countries.19, 20 The outcome variable, sleep deprivation, was measured using the GSHS question: “During the past 12 months, how often have you been so worried about something that you could not sleep at night?” Responses were dichotomized, with “most of the time” or “always” indicating sleep deprivation. The primary explanatory variable, cigarette smoking, was measured using the GSHS question: “During the past 30 days, on how many days did you smoke cigarettes?” Responses were dichotomized, with “any smoking in the past 30 days” classified as current cigarette smoking. The GSHS data collection in each country occurred during the regular academic year, typically spanning 2-3 months. While seasonal variations could potentially influence sleep patterns, the standardized GSHS questionnaire asks about sleep experiences over the past 12 months, thus capturing year-round patterns rather than seasonal effects.
Additional variables included in the analysis were age, sex, physical activity (“During the past 7 days, on how many days were you physically active for a total of at least 60 minutes per day?”), food insecurity (“During the past 30 days, how often did you go hungry because there was not enough food in your home?”), being bullied (“During the past 30 days, on how many days were you bullied?”), and having close friends (“How many close friends do you have?”). These variables were chosen based on their potential relationships with both smoking and sleep patterns, as indicated by previous literature.21,22
Statistical analysis
Data analysis was carried out using Stata version 18. To account for the complex survey design, the ‘svyset’ command was used, with primary sampling units, sampling weights, and stratification incorporated to ensure accurate population-level estimates.
Descriptive data analyses were performed to characterize the study participants. We used survey-weighted tabulations to estimate the prevalence of sleep deprivation across various demographic and behavioral factors, including age, sex, food insecurity, physical activity, bullying experiences, and friendships. Pearson’s chi-squared test with the “Rao and Scott second-order correction” was used to assess bivariate associations.
Missing data across variables varied from 0.4% to 5.7%. To address potential bias from missing data, multiple imputation was implemented using a chained equations approach. Imputation models were run separately for each country, creating 10 imputed datasets per country. The imputation process incorporated all the variables that were subsequently included in the final models. The analysis examined the association between sleep deprivation and cigarette smoking using imputed survey-weighted multiple logistic regression. The model adjusted for sex, age, hunger status, physical activity, bullying experiences, and friendships. Potential effect modification was tested for using interaction terms. No significant interactions were detected.
To synthesize results across the GCC countries, we conducted a meta-analysis. Country-specific odds ratios and their 95% confidence intervals were extracted from the imputed data analyses. These were then combined using a random-effects meta-analysis, with results presented in a forest plot. The significance threshold was set at p<0.05, with all analyses using a two-tailed approach. Odds ratios with 95% confidence intervals are reported to quantify the strength of associations. The degree of heterogeneity was evaluated using Cochran’s Q test, I² statistic, and τ² (tau-squared). We roughly followed the suggested thresholds in the Cochrane handbook23 considering I² values of <30%, 30-50%, 50–75%, and >75% as “not important, moderate, substantial, and considerable heterogeneity”, respectively. We assessed potential outliers and no country-specific effect sizes were identified as statistical outliers.
Ethical considerations
The GSHS protocols were approved by both the WHO and the respective ministries of health or education in each participating country. All participants, as well as their parents or guardians, gave informed consent to participate in the study.
Results
Sample characteristics
The study included a total of 21,105 adolescents from 5 GCC countries. Table 1 presents the baseline attributes of the sample stratified by sleep deprivation status. Overall, 17.9% of the participants reported experiencing sleep deprivation (defined as “feeling so worried that they could not sleep at night most of the time or always”). Sleep deprivation was more prevalent among older adolescents, with 21.1% of those aged 16–18 years reporting sleep issues compared to 13.2% of those 12 years or younger (p<0.001). Sex variations were observed, with boys reporting higher rates of sleep deprivation (22.9%) compared to girls (12.8%, p<0.001). Food insecurity was strongly associated with sleep deprivation. Among those being hungry most of the time or always, 31.9% reported sleep deprivation, compared to 14.2% among those never being hungry (p<0.001). In addition, bullying experiences were also significantly associated with sleep deprivation, with 26.2% of bullied adolescents reporting sleep issues compared to 13.6% of non-bullied peers (p<0.001). Interestingly, physical activity levels were not significantly associated with sleep deprivation (p=0.523).
- Characteristics of the study population stratified by sleep deprivation status among adolescents in Gulf Cooperation Council countries (n=21,105).
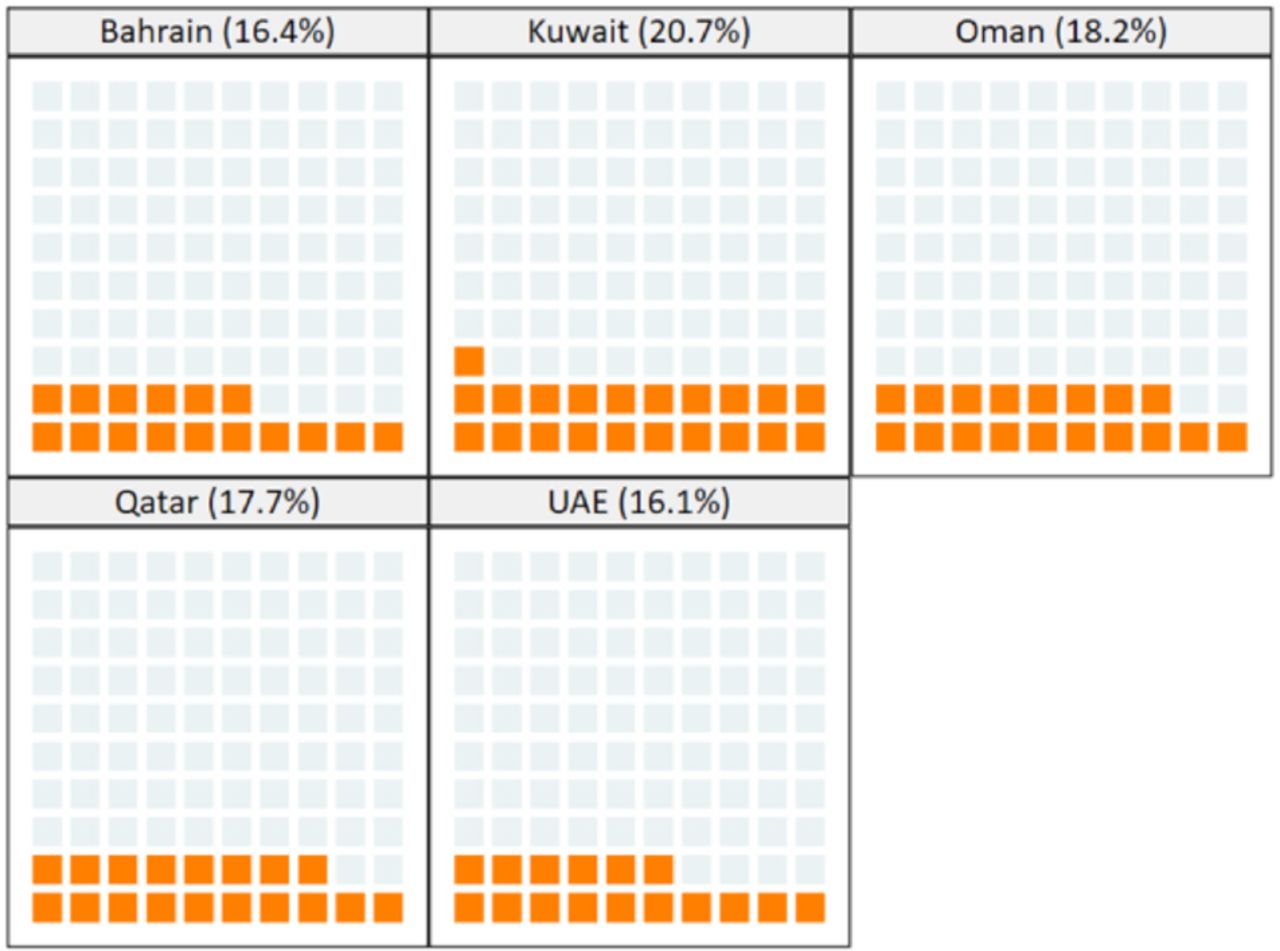
Figure 1 illustrates the prevalence of sleep deprivation across the 5 GCC countries using a waffle plot. Kuwait reported the highest prevalence of sleep deprivation (20.7%), followed by Oman (18.2%), Qatar (17.7%), Bahrain (16.4%), and the UAE (16.1%).

- Prevalence of sleep deprivation (most of the time or always) among adolescents across five Gulf Cooperation Council countries
Association between sleep deprivation and cigarette smoking
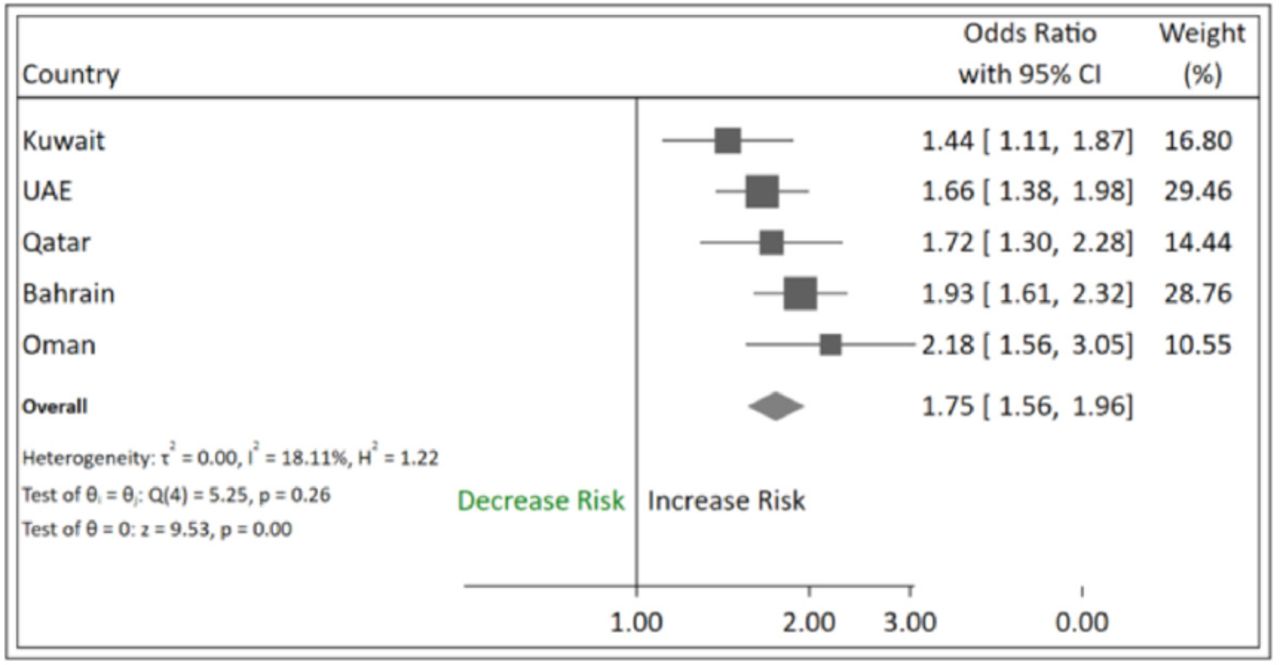
Figure 2 presents a forest plot of the association between cigarette smoking and sleep deprivation across the 5 countries, adjusted for potential confounders. The meta-analysis revealed a significant positive association across all countries.

- Forest plot showing the association between cigarette smoking and sleep deprivation among adolescents in Gulf Cooperation Council countries.
The pooled odds ratio (OR) for the cigarette smoking association with sleep deprivation was 1.75 (95% CI: 1.56–1.96), indicating that adolescents who smoked cigarettes had 75% higher odds of suffering sleep deprivation in comparison to non-smokers, after adjusting for covariates.
The strength of this association varied somewhat across countries. Oman showed the strongest association (OR: 2.18, 95% CI: 1.56–3.05), while Kuwait showed the weakest, yet still significant, association (OR: 1.44, 95% CI: 1.11–1.87). The heterogeneity across countries was low, as evidenced by the overlapping confidence intervals as well as heterogeneity statistics (I²=18.1%; Cochran’s Q test p=0.26).
Discussion
The results presented provide important insights into the relationship between cigarette smoking and sleep deprivation among youth in GCC countries. The observed significant positive association, with 75% higher odds of sleep deprivation among adolescent smokers compared to non-smokers, is consistent with previous research conducted in other regions.22,24,25 While point estimates varied somewhat across GCC countries, the overlapping confidence intervals and low heterogeneity statistics (I²=18.1%) suggest a consistent association throughout the region. The wider confidence interval observed in some countries, such as Oman, likely reflects sampling variation rather than true differences in the strength of the association.
The significant association between sleep deprivation and other factors, such as food insecurity and bullying, underscores the importance of addressing the broader determinants of adolescent health and well-being. Sleep deprivation has been linked to various adverse consequences, including reduced academic performance, mental health problems, and increased risk-taking behavior. The importance of addressing these underlying factors through comprehensive public health interventions cannot be overstated.
The underlying mechanisms linking cigarette smoking and sleep disturbances are not well established but multiple potential mechanisms have been proposed. Nicotine, the primary psychoactive component in cigarettes, is a stimulant that can significantly disrupt sleep architecture and quality.26 Nicotine’s effects on the central nervous system are multiple, including its ability to increase physiological arousal and suppress “rapid eye movement (REM)” sleep.27 This can contribute to difficulties in falling asleep, frequent nighttime awakenings, and reduced overall sleep quality and quantity.21,24,28 Nicotine’s stimulant properties can lead to hyperarousal, making it challenging for the body to transition into the relaxed state necessary for restorative sleep. Additionally, the suppression of REM sleep, which is essential for cognitive and emotional processing, can further exacerbate the impact of nicotine on sleep health. A prospective cohort study that measured sleep parameters using actigraphy found that nicotine use in the evening was linked to both lower sleep quality and increased awakenings after sleep onset.26 Moreover, secondary analysis of a randomized controlled trial showed a dose-response relationship where higher nicotine consumption was associated with more sleep disruption.29
Cigarette smoking has also been associated with a higher risk of obstructive sleep apnea. This can further exacerbate sleep disturbances by causing fragmented and poor-quality sleep, leading to adverse health consequences. Smoking-related inflammatory changes in the upper airway, impaired respiratory control, and increased deposition of fat in the neck region are potential contributary mechanisms to the development and worsening of sleep apnea.
Other potential mechanisms linking cigarette smoking to sleep deprivation among adolescents include the impact of smoking on mental health and stress levels. Chronic cigarette use has been linked to elevated risks of anxiety and depression, which can contribute to difficulties in the ability to initiate and sustain sleep. Smoking may also serve as a coping mechanism for some adolescents to manage stress and negative emotions. However, this can further exacerbate sleep problems by leading to nicotine dependence and withdrawal symptoms during the night.30 The associated routines and rituals associated with smoking mean the act itself can disrupt sleep patterns and circadian rhythms, making it harder for adolescents to establish a consistent and healthy sleep-wake cycle.
The observed association between sleep deprivation and smoking raises the possibility of “reverse causation,” where sleep deprivation may contribute to the initiation and maintenance of smoking among adolescents.31 Sleep disturbances can lead to increased daytime fatigue, impaired cognitive function, and emotional dysregulation, all of which may drive adolescents to use cigarettes as a means of coping or self-medicating.32,33 Nicotine, the primary psychoactive component in cigarettes, can have a temporary alerting effect and may be perceived by some adolescents as a way to counteract the negative consequences of poor sleep.32 Additionally, chronic sleep deprivation has been linked to increased impulsivity and risk-taking behaviors,34,35 which could lower the threshold for experimenting with and becoming addicted to cigarettes. This potential reverse causation highlights the need to understand the complex and bidirectional relationship between cigarette smoking and sleep deprivation among adolescents.36 Further longitudinal research is necessary to elucidate causal pathways and potential feedback loops.
Our findings suggest the need for integrated interventions that simultaneously address both smoking prevention and sleep health in GCC countries. These interventions could include school programs combining tobacco prevention with sleep hygiene promotion, and healthcare provider training for screening and counseling about both behaviors. However, implementation of such interventions in GCC countries may face unique challenges, including traditional late-night social gatherings that affect youth sleep patterns and the need to balance modern public health approaches with cultural values. The experiences of GCC countries in addressing these challenges could provide valuable lessons for other rapidly developing regions facing similar transitions in youth health behaviors, particularly given the strong and consistent association between smoking and sleep deprivation observed.
The strengths of this study include its large, multinational sample across the GCC countries, which provides robust and generalizable findings on the association of cigarette smoking with sleep deprivation in this region. The use of standardized survey protocols and analytical methods, such as the meta-analysis approach, further enhances the reliability and validity of the results. Additionally, the study’s consideration of important confounding factors, such as sociodemographic characteristics, food insecurity, and bullying experiences, provides a more holistic perspective of the complex relationships involved. The findings have important public health implications, as they emphasize the need for interventions to address both cigarette smoking and sleep-related issues in the GCC countries.
Limitations of this study include the cross-sectional design, which impedes the establishment of causal relationship, and the utilization of self-reported data, which may be susceptible to recall bias and social desirability. Additionally, the use of secondary data from the GSHS means that the researchers had limited control over the data collection methods and the measurement of key variables. Further research employing longitudinal designs and objective sleep assessment tools would help establish the temporal relationship between cigarette smoking and sleep deprivation in the GCC region.
Conclusion
The findings of this study demonstrate the strong association between sleep disturbances and cigarette smoking among GCC adolescents. The complex neurobiological mechanisms underlying this relationship and the potential for reverse causation emphasize the need for comprehensive interventions to address both cigarette use and sleep-related issues. Future research should prioritize longitudinal studies employing objective sleep assessment tools to establish temporal relationships between smoking initiation and sleep difficulties among GCC adolescents. Intervention trials testing integrated approaches to smoking prevention and sleep promotion are needed, particularly those adapted to the region’s cultural context.
Acknowledgments
We would like to thank Cambridge Proofreading LLC (proofreading.org) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received September 4, 2024.
- Accepted December 29, 2024.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.