


Abstract
Objectives: To explore depression and its associated factors in a sample of primary headache patients with a history of head-neck trauma (Ph-nT).
Methods: A cross-sectional study of 120 conveniently sampled patients at Al Madinah Al Munawarah hospitals, Saudi Arabia during the period of June 2019 to December 2019 with Primary headache and history of head-neck trauma completed the depression subscale of the Depression, Anxiety and Stress Scale-21 (DASS-21), and a structured tool for demographics and clinical characteristics.
Results: Prevalence of moderate to extremely severe levels of depression was 15.8%. The majority of Ph-nT were female (64.2%), had migraine (with/without aura) (57.5%), recorded no sports-related activities (65.8%), and complained of insufficient sleep (67.5%). Primary headache patients with a history of head-neck trauma, and a family history of migraine/chronic headache, had higher depression scores (β=1.77, p=0.02).
Conclusion: Prevalence of depressive symptoms is higher in a sample of primary headache patients with a history of head-neck trauma than in the population that did not experience that trauma. Identification of predictors of depression in primary headache patients with a history of head-neck trauma may help in evolving targeted prevention and screening programs.
People affected by depression, a mood disorder, have unrelenting feeling of sadness, despair, and loss of interest in activities they previously enjoyed.1 According to the Diagnostic and Statistical Manual of Mental Disorders, fifth edition, a clinical diagnosis of depression depends on the presence of a sad frame of mind, or loss of interest along with a set of 3-4 additional symptoms for a minimum period of 2 weeks.1 These additional symptoms include both emotive and physical dimensions such as marked change in body weight or appetite, diminished thinking ability, decrease in physical activity, fatigue, lack of energy, feeling of guilt, unworthiness, reduced concentration, and suicidal thoughts.1 According to the World Health Organization, depression is a common mental disorder that affects approximately 5% of adults around the world.2 Depression decreases work output, quality of life, increases global burden of disease, and is a major cause of disability.2 A meta-analysis of 16 studies found that migraine and depression are sometimes comorbid. Therefore, future research to identify different subgroups of migraine patients who are usually affected by depression may help in creating targeted management and screening of depression and its negative psychological effects.3 A subgroup of primary headache patients that has not been studied extensively is those with a history of head-neck injury.
A large population-based study in Netherlands found many risk factors for chronic headache including psychiatric conditions, sleep problems, and history of head-neck injury.4 However, those with head-neck injury have not been studied widely. A recent review highlighted that absence of information such as clinical features, associated factors, biomarkers, and so on, is not allowing development of prospective treatment for patients with post-trauma primary headache.5 The outcome of prospective studies involving identification of risk factors, associated factors, and comorbidities may help in the early identification of subgroups who are more likely to progress to chronic migraine.6,7 Therefore, in this study, the application of a model to predict changes in the levels of severity of depressive symptoms and clinical presentation of primary headache and its prevalence were studied in a sample of clinically diagnosed primary headache patients with a history of head-neck trauma (Ph-nT).
Methods
The study, which was descriptive, observational, and correlational in design, was carried out at the out-patient Neurology Service Department, Madinah Al Munawarah, Kingdom of Saudi Arabia. All patients presenting at the outpatient division during the study period of June 2019 to December 2019, and who met the inclusion criteria after initial screening were asked to participate. Patients who agreed to participate were provided with a brief description of the study. This description explained the major theme, method and aim of the study in common language for prospective participants. Finally, all patients were required to be screened and meet all inclusion and exclusion criteria. Inclusion criteria: i) adults, 18 years of age and older, ii) patient-reported headache/migraine symptoms for at least 6 months, and iii) history of traumatic head/neck injury. Exclusion criteria included individuals diagnosed with secondary headaches. Data were collected for 165 interviewed patient and finally, a sample of 120 headache/migraine patients with history of head-neck injury (number: 120, and age: 18-48 years) completed a cross-sectional survey. Survey tools included the standardized and previously validated instrument, the Depression, Anxiety Stress Scale (DASS-21), to measure depression, and an elaborate set of questions to gather sociodemographic and medical history of participants.8,9 This survey was interviewer-administered during the patient’s visit to the Neurology Clinic.
Data was obtained with signed informed consent from participants in accordance with standard research practices. Participants were informed they would not get any financial rewards; participation would have no bearing on their treatment, they would experience no exposure to harmful/invasive procedures, and they were free to discontinue participation at any stage of the study. The survey study and subsequent data entry ensured complete confidentiality of participants’ information. The study was carried out in accordance with the recommendations of the institutional ethics committee, the Declaration of Helsinki 2002, and the principles of good medical practice.
The short form of DASS-21
Depression, Anxiety Stress Scale is a widely cited and rigorously validated questionnaire tool to assess perceived depression, anxiety and stress.8,9 The questionnaire has 3 dimensions, each consists of 7 items and measures severity levels of depression, anxiety, and stress.8,9 All questions are scored on a Likert scale of 0 to 3, where higher scores imply increasing weekly frequency of mental health-related symptoms. Depression, Anxiety Stress Scale has been previously used in the Saudi population.10 The dimension scores of depression, anxiety and stress are derived by adding the scores of these subscales. Higher scores of these dimension/subscales indicate increasing severity of symptoms of mental health problems. The reliability of depression subscales was very good McDonald’s omega (maximum likelihood approach) values of 0.84 in this study sample.11 In this study, only questions regarding the depression subscale were used.
Set of questions to record patients’ information: social, demographic and medical history
A set of 9 questions was employed to gather patient information related to sociodemographics and clinical history. Information regarding clinical classification of the headache/migraine, obtained from the medical records after obtaining permission, was based on the clinical diagnosis. The question of age was open ended; there were 7 closed-ended questions regarding gender, marital/social status, sports activity, using medication for other conditions, insufficient or sufficient sleep, family history of chronic headache/migraine, and frequency of use of migraine medication.
Statistical analysis
Data was entered to an Excel spread sheet and transferred to SPSS, version 26.0 (IBM Corp, Armonk, NY, USA). OMEGA macros were used to perform all statistical analysis in this study.12 Descriptive statistics, psychometric tests-McDonald’s omega, and multivariate association tests of multiple linear regression were used. McDonald’s omega was calculated separately for 3 dimensions/subscales of depression, anxiety, and stress of the DASS-21 using factor loadings derived from the maximum likelihood factor analysis for forced single-factor solutions.12 For multiple linear regression: total scores of the depression subscales were used as the dependent variable. While socio-demographics and clinical history were used as independent variables.
Results
In this study, participants’ average age 33.24±8.63 years and depression scale was 4.47±2.90 (Table 1). According to the clinical diagnosis, chronic tension headache (40.8%), and migraine without aura (39.2%) were the 2 most prevalent types of headache. Females (64.2%) formed the larger group of headache patients with a history of head-neck trauma. Most participating (Ph-nT) were married (54.2%), and did not habitually participate in sports activities (65.8%). More than one-third of study participants (34.2%) were under treatment for comorbid conditions. Approximately two-third of the participating Ph-nT complained of insufficient sleep (67.5%). More than two-fifths of study participants had a family history of migraine headache or chronic headache, and frequently (often-very often) used drugs to manage migraine. The prevalence of moderate to extremely severe levels of depression was 15.8% (Table 1).
- Characteristics of participating headache/migraine patients with history of head-neck injury.
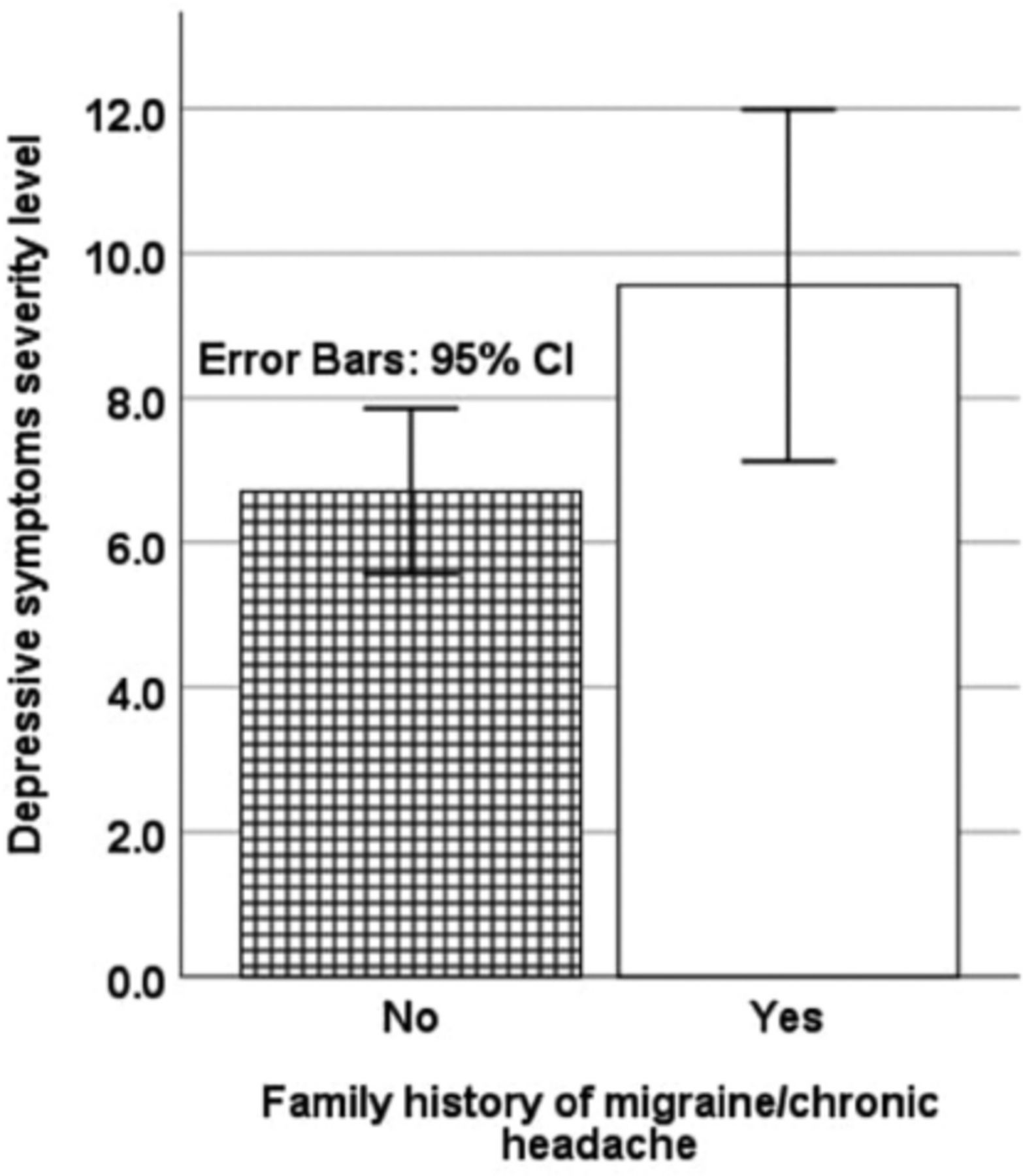
Multiple linear regression-predictors of the severity level of depressive symptoms in headache/migraine patients with history of head-neck injury. A multiple linear regression model with a depression score as a dependent variable, and headache clinical diagnosis, such as, migraine with aura, migraine without aura, chronic-tension type headache, new daily persistent headache; sports activity (Yes/No); using medication for other conditions (Yes/No); family history of migraine headache or chronic headache (Yes/No); use of migraine medication (Yes/No); marital status (married, single, divorced, widowed); complaint of insufficient sleep (Yes/No); gender, age were statistically significant, F(9, 108)=1.95, p=0.05, R2=0.07 (Table 2). Family history of migraine/chronic headache (p=0.02) significantly predicted depression severity level (Table 2). Those with family history of migraine headache or chronic headache had higher depression scores (Figure 1).
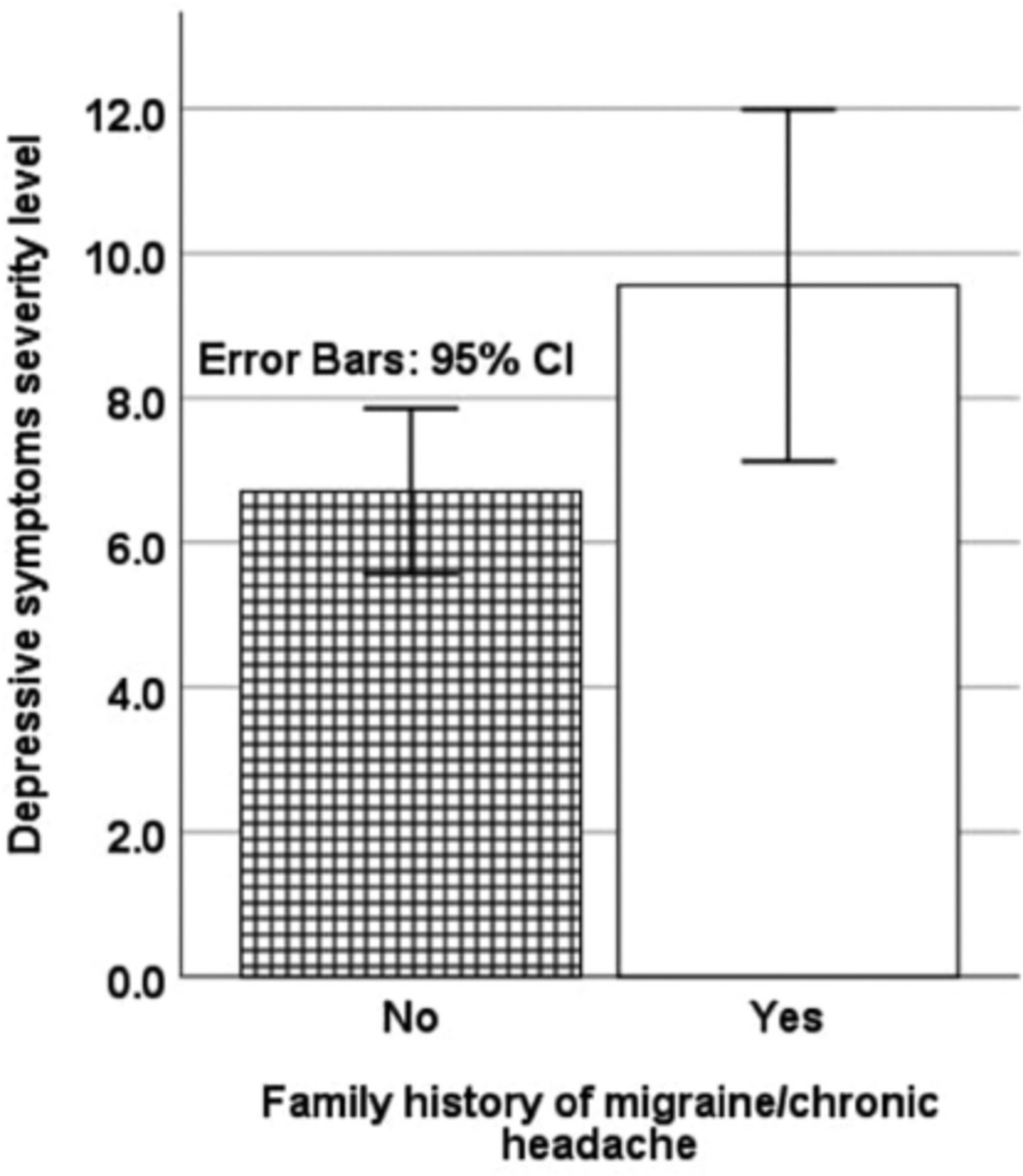
- Variation with family history of migraine/chronic headache in depressive symptoms severity level (assessed by DASS-21: Depression anxiety stress scale-21) in migraine-headache patients with history of Head-Neck injury
- Multiple Regression Predictors of the depressive symptoms severity level in headache/migraine patients with history of head-neck injury
Discussion
This study investigates different types of clinical presentations of primary headache and their prevalence in a sample of Ph-nT in Saudi Arabia. It also showed moderate-extremely severe level of depressive symptoms was seen in approximately 16% of (Ph-nT). This study sample revealed a majority of participants had migraine (with/without aura) followed by chronic-tension-type headache. The majority of (Ph-nT) were female, recorded no sports-related activities, and complained of insufficient sleep. Many in the study sample were under treatment for comorbid medical illnesses, had a family history of migraine-chronic headache, and regularly used (often-very often) migraine medications. Finally, Ph-nT and a family history of migraine/chronic headache had higher depression scores.
With regards to the prevalence of moderate to extremely severe levels of depressive symptoms in this study, there are no directly similar studies to compare outcomes. However, Lucas et al13 reported similar results, such as, a prevalence of 15% for depression at baseline among patients with mild traumatic brain injury. Both studies employed standardized questionnaires to assess depressive symptoms. Lucas et al13 operationalized depression as a score ≥10 on the Patient Health Questionnaire-9, while in this study, moderate-extreme levels of severe depressive symptoms were defined as a score ≥14 on the depressive subscale of the DASS-21.8,9
The majority of cases in this study suffered from migraines followed by those with chronic-tension-type headaches. A recent systematic review on prevalence and clinical presentation of chronic post-traumatic headache in children and adolescents found that migraine is the most prevalent complaint, followed by tension-type headache seen in approximately 25% of cases in this group.14 In this study, we found slightly higher values, such as, 41% for tension-type headache. This difference may be explained by the differences in the sample characteristics of the 2 studies. Shaw et al14 presented clinical feature of primary headache in children and adolescents; in this study, clinical presentation of primary headache was investigated in a sample of patients aged 18-48 years. In this study, females comprised the majority of Ph-nT. A recent review pointed out conflicting reports on the influence of gender on post-traumatic primary headache; though the majority of the articles point toward a female majority.15 This has been explained by a difference in gender-related reporting and endocrine physiology, such as—higher estrogen levels increasing peripheral nociception, affecting bradykinin B2 receptors and μ-type opioid receptors, and an estrogen-related decrease in levels of nociceptive pathway’ neurotransmitters in females.15
The relationship between no sports activity and Ph-nT in this study, is similar to previous studies.16 The effects of long-term habitual physical activity may help in life-style related migraine prevention. This may be explained by a surge in plasma β-endorphins and brain-derived neurotrophic factor associated with habitual physical activity.16 In this study, a majority of the study sample recorded insufficient sleep, similar to a conclusion drawn in a recent review on the global prevalence of insufficient sleep. The review summarized that complaints of insufficient sleep were significantly higher in migraine patients compared to those with sufficient sleep and non-migraine headache groups.17 A recent study on the phenotypes of unremitting post-traumatic headache in patients with mild traumatic brain injury found that 69% of migraine episodes were triggered by a lack of sleep.18 These previous reports and findings from this present study reaffirm the relationship between sleep insufficiency and migraine in general, and migraine-related to trauma in particular. The latter finding is a novel outcome of this study.
Additionally, this study found a significant model to predict changes in depressive symptoms. This model is based on 3 broad categories of predictors, such as, social, demographic, and clinical characteristics. A family history of migraine-headache was the only significant determinant of increasing depressive symptoms in this study sample. The novel findings of this study, on the identification of a significant model as well as significant determinants of depressive symptoms among Ph-nT elaborates and builds upon the previously established relationship between depression and migraine.3
Generalizations from this study are hampered by limitations in the study design and sampling strategy. Future studies should employ randomized sample selection instead of a non-probabilistic sample selection method. Future studies with multi-centric data collection, longitudinal designs and randomized sampling methods may better establish and elaborate on the findings of this study. Nevertheless, it is important to note that unlike some previous studies based on subjective evaluation only; in this study, a sample of clinically diagnosed Ph-nT was recruited.
In conclusion, the severity of depressive symptoms was higher in primary headache patients with a history of head-neck trauma as well as with a family history of migraine headache. Therefore, early screening and targeted delivery of mental health counseling may help prevent depressive symptoms in this group. Additionally, the majority of Ph-nT were female, recorded no sports-related activities, and complained of insufficient sleep. Therefore, early screening programs may target these groups for preventive treatment strategies against development of chronic migraine.
Acknowledgment
I would like to thank Ms. Gail Guterl for the English language editing.
Footnotes
Disclosure. Author have no conflict of interests, and the work was not supported or funded by any drug company.
- Received March 31, 2022.
- Accepted June 1, 2022.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.




{kind=link}