


Abstract
Citrobacter koseri is a gram-negative bacillus that causes mostly meningitis and brain abscesses in neonates and infants. However, brain abscess caused by Citrobacter koseri infection in an adult is extremely rare, and only 2 cases have been described. Here, we reported a 73-year-old male presenting with a 3-week headache. A history of diabetes mellitus was noted. The images revealed a brain abscess in the left frontal lobe and pus culture confirmed the growth of Citrobacter koseri. The clinical symptoms improved completely postoperatively.
Citrobacter koseri, formerly known as Citrobacter diversus, is a gram-negative bacillus that causes mostly meningitis and brain abscess in neonates and infants.1 However, brain abscess caused by Citrobacter koseri in an adult is extremely rare and only 2 cases have been described in the literature.2,3 Herein, we report another rare case of brain abscess caused by Citrobacter koseri in an elderly male. The relevant literature is also reviewed. Our objective in presenting this particular case is to share our experience in the management of this rare brain abscess caused by Citrobacter koseri.
Case Report
A 73-year-old male was admitted to our hospital with a 3-week history of mild headache and general malaise. He had been treated for urinary infection for one month at a local clinic before admission and an empirical oral antibiotic was prescribed. Urine culture was not performed. His past medical history was significant for diabetes mellitus, and he had been treated with oral anti-diabetic agents. At admission, he was afebrile, alert, and oriented. No neck stiffness or focal neurology was found. The remainder of the general examination was unremarkable. The peripheral blood white cell count was 9730/µl (4000~10000/µl). The C-reactive protein level was 0.665mg/dL (0.010~0.500mg/dL) and the erythrocyte sedimentation rate level was 41mm/h (0~20mm/h). No bleeding diathesis was noted.
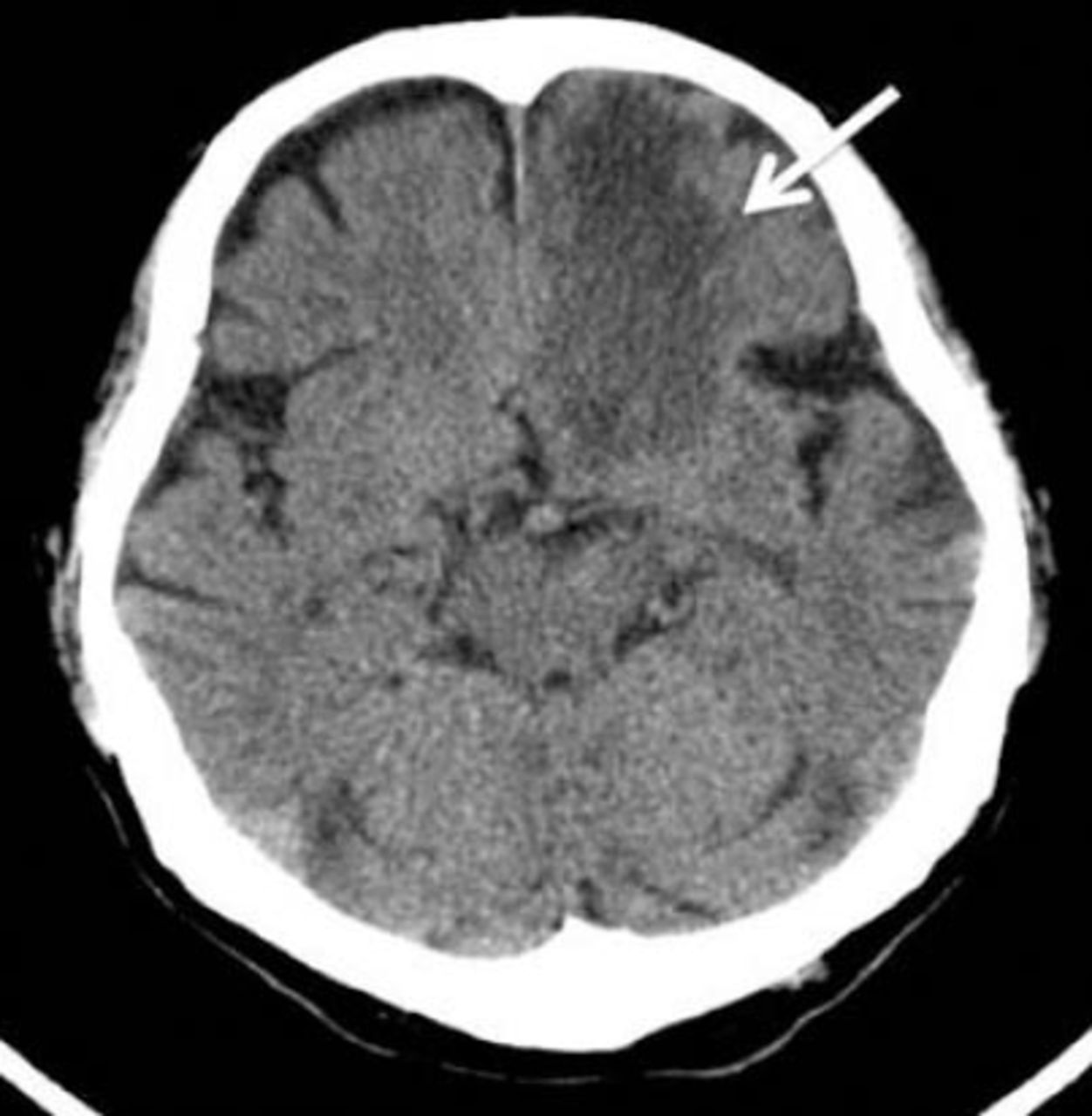
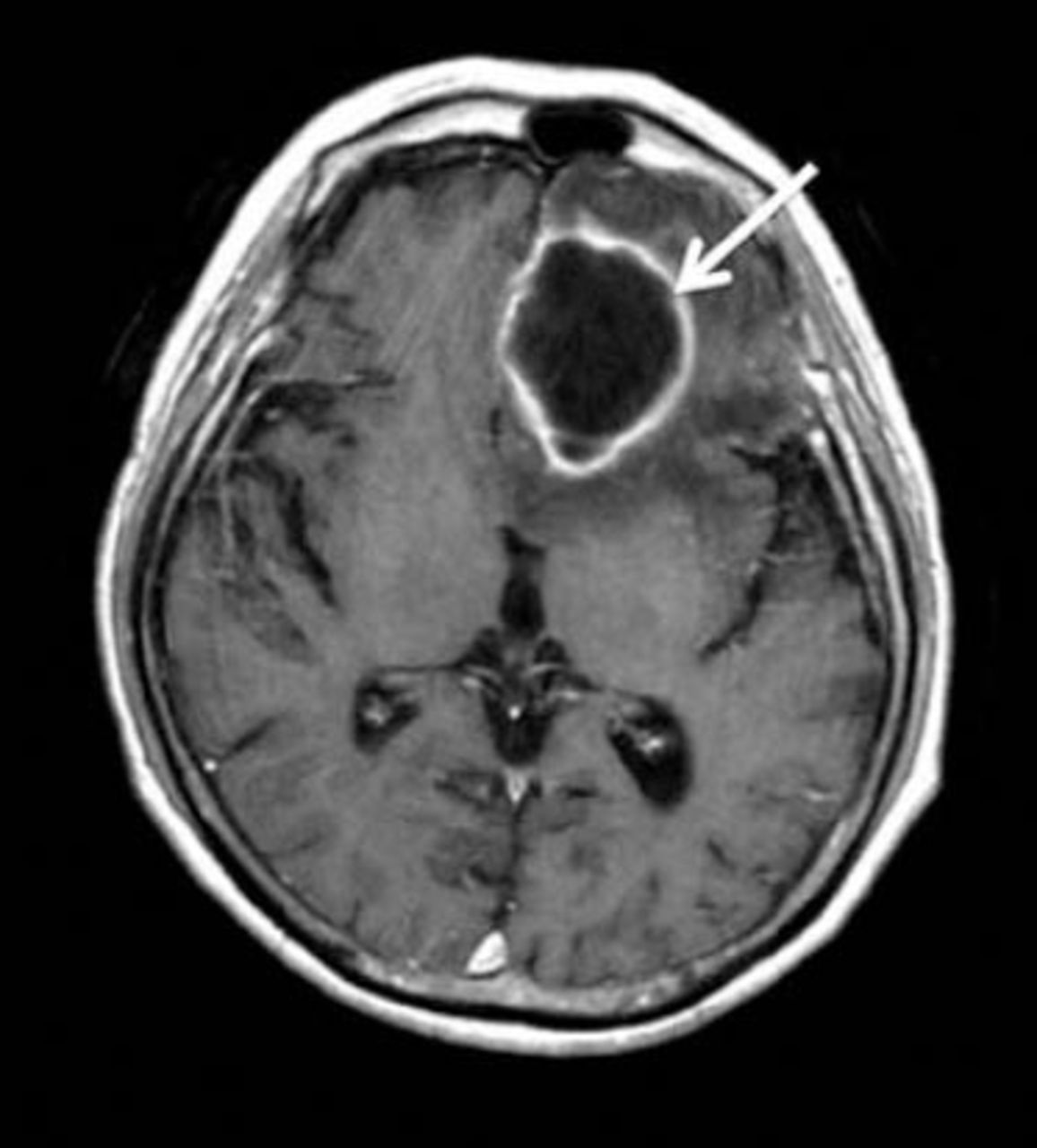
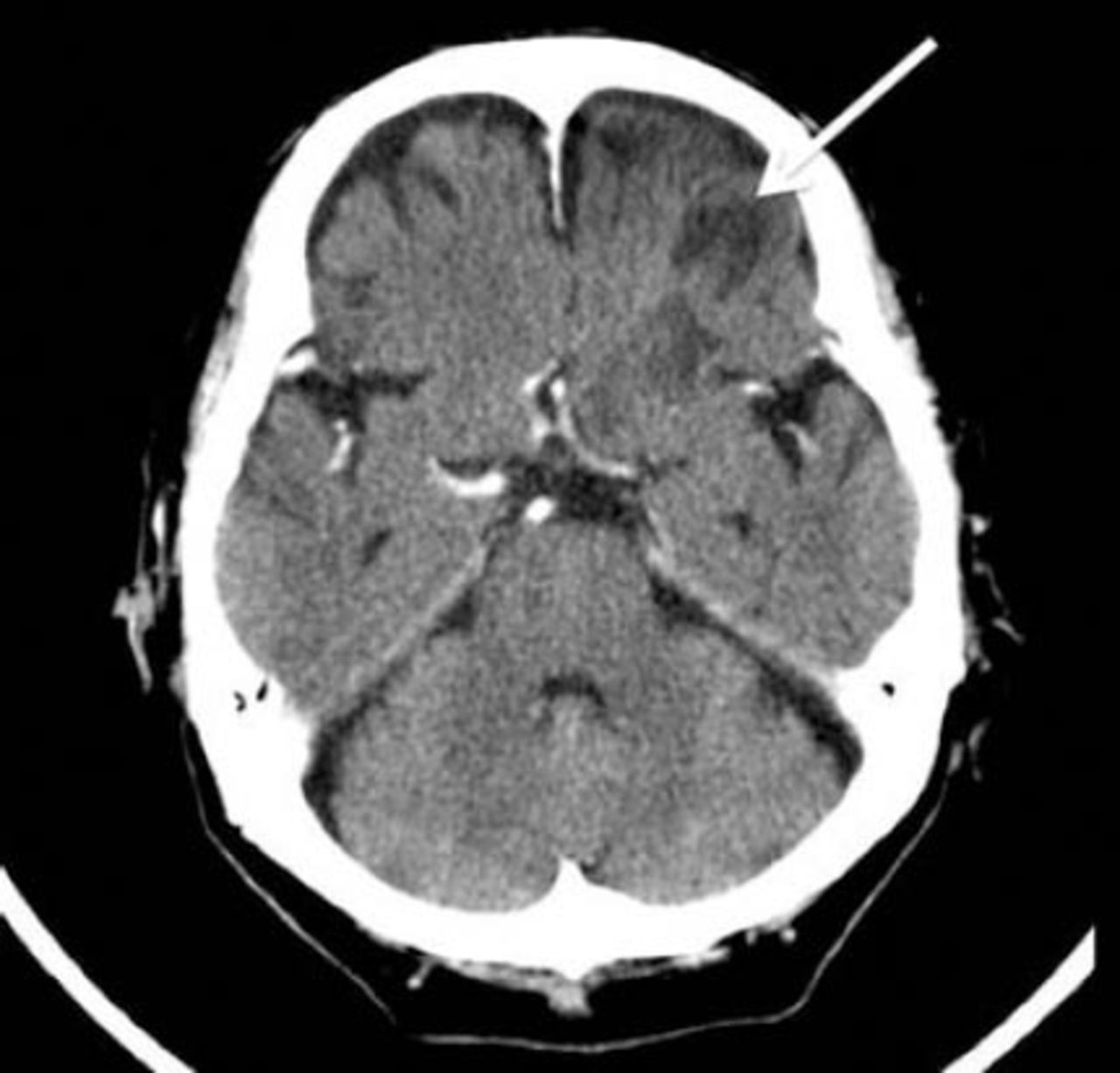
A CT scan of the brain revealed a hypodensity lesion in the left frontal lobe (Figure 1). The MRI of the brain revealed a ring-enhanced lobulated mass approximately 4.5 cm in diameter, located in the basal area of the frontal lobe (Figure 2). The mass appeared as low intensity in T1-weighted, and high intensity in T2-weighted images, which were consistent with a brain abscess. He then underwent a left frontal craniotomy with removal of the mass 2 days after the imaging study. During operation, a well-encapsulated mass was located in the left frontal lobe. After opening the capsule of the mass, the yellowish turbid pus within the mass was explored. The wall of the abscess was partially removed, and a surgical drain was placed in the cavity of the abscess. The surgical drain was kept in situ for 5 days. The previous symptoms recovered gradually postoperatively. Culture from the abscess confirmed the growth of Citrobacter koseri. In the antibiotic susceptibility test, the Citrobacter koseri revealed resistance to ampicillin and sensitivity to cefazolin, gentamicin, imipenem, ciprofloxacin, cefmetazole, ceftazidime, aztreonam, ceftriaxone, cefepime, levofloxacin, and meropenem. He was treated with intravenous ceftriaxone 2 g every 12 hours for 6 weeks. The subsequent CT scan of brain revealed no enhanced residual abscess 2 months after surgery (Figure 3). In the follow-up 3 months later, the patient was found to be completely healthy.

The axial view of the CT scan of the brain revealed a hypodensity mass (white arrow) in the left frontal lobe.

The MRI of the brain revealed a mass (white arrow) in the left frontal lobe that was ring-enhanced in the T1-weighted image.

The axial view of the CT scan of the brain revealed no enhanced residual abscess (white arrow) in the left frontal lobe.
Discussion
Citrobacter koseri, a facultatively anaerobic, lactose-fermenting, gram-negative bacillus, belongs to the family Enterobacteriaceae.4 It is commonly found in soil and water, and in the intestinal tracts of animals and humans.1 Unlike Citrobacter freundii, which is usually associated with hepatobiliary tract infections, Citrobacter koseri has a strong propensity to cause meningitis and brain abscess in neonatal and infants, with higher morbidity and mortality rates.4,5 Abscess caused by Citrobacter koseri infection in adults is infrequent, and only 12 cases have been reported in the literature.1 However, brain abscess caused by Citrobacter koseri is extremely rare, and only 2 cases have been described.2,3 The first case, reported by Booth et al in 1993,2 was that of a 66-year-old female with a history of headache, confusion, and mild photophobia. She had a history of diabetes mellitus. A previous urinary infection caused by Citrobacter koseri was treated one month before admission. The brain abscess in the right parietal lobe and ventriculitis was diagnosed by CT scans. The patient was treated with an 8-day surgical drainage and a 16-day netilmicin and cefotaxime regimen. Her clinical recovery was incomplete. The other case, reported by Lind et al in 2005,3 was that of a 78-year-old female who presented with a 6-month history of confusion and personality changes. Her medical history included paroxysmal atrial fibrillation and a 10-day course of high-dose dexamethasone. A parasagittal tumor at the anterior frontal base was seen in the images. The peritumoral abscess was aspirated at operation. Atypical meningioma was diagnosed, and the pus culture confirmed the growth of Citrobacter koseri. Five days of intravenous ceftriaxone followed by 6 weeks of meropenem at a dosage of 1 g every 8 hours were prescribed. At the 9-month follow-up, she had recovered well, except her cognitive functioning.
The pathophysiology of central venous system infection caused by Citrobacter koseri remains unclear. In neonates, the immature blood-brain barrier and a specific 32 kD outer membrane protein of Citrobacter koseri contributes to the tendency of Citrobacter koseri to form a brain abscess.1 However, in adults, Citrobacter koseri is most commonly isolated from the urinary tract.6 A history of head trauma, a previous neurosurgical procedure, bacteremia, diabetes mellitus, or urinary infection have been proposed as the risk factors.7 Although the pathogen of the previous urinary tract infection was unknown, it may have been the origin of our patient’s infection, similar to the case reported by Booth et al.2
Because of the rarity of the cases of adult brain abscess caused by Citrobacter koseri infection, the “gold standard” of treatment remains unknown. Although conservative treatment with antibiotics alone has been reported to be successful in the management of pediatric Citrobacter koseri brain abscesses, early aggressive surgical intervention followed by medical management is highly recommended, especially when encapsulated or multi-lobulated brain abscesses form.4 In general, Citrobacter koseri is usually resistant to ampicillin, and has variable susceptibility to aminoglycosides.4 Despite the antibiotic susceptibility tests, third-generation cephalosporin, aminoglycosides, or trimethoprim are the recommended antimicrobial agents. When resistance to beta-lactam induction is found, imipenem, chloramphenicol, or multidrug therapy is alternatively advised. Intravenous antibiotics may be prescribed for a minimum of 6-8 weeks, and may be extended based on clinical response.
However, the outcome of pediatric Citrobacter koseri brain abscess remains unfavorable. Nearly one-third of patients with this infection have died, and more than 50% have residual neurological deficits.5,8 The prognosis of the 2 adult patients with Citrobacter koseri brain abscesses reported in the literature was unequal.2,3 The former may be the first case of an infection involving the cerebrospinal fluid system, and the treatment with intravenous antibiotics was too short (only 16 days).2 The latter case involved a good recovery after complete excision of the tumor and abscess lesion following management with full-course antibiotics.3 In our case, partial excision of the encapsulated wall and aspiration of the abscess were performed, and the patient achieved complete recovery following a full course of intravenous antibiotics.
In conclusion, although brain abscess caused by Citrobacter koseri infection in adults is extremely rare, it may be the possible causative microorganism of brain abscesses in immunocompromised adult patients or following previous urinary infection by Citrobacter koseri.
Footnotes
Disclosure
The authors have no affiliation or financial involvement with organizations or entities with a direct financial interest in the subject matter or materials discussed in the manuscript. No funding was received for this work from any organization.
- Received November 30, 2014.
- Accepted March 16, 2015.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.