


Abstract
Angiolipomas of the spine are rare benign tumors commonly presenting with compressive myelopathy. The present report describes a case of spinal angiolipoma with thoracic mediastinal extension in a 50-year-old woman. She presented with a long-standing history of mid-back pain with progressive lower extremities weakness. An MRI showed a heterogeneously enhancing mass located in the posterior epidural space of the thoracic spine with mediastinal extension. Histopathological examination demonstrated features consistent with spinal angiolipoma. This report emphasizes the diagnosis and therapeutic management options of infiltrating spinal angiolipomas.
Spinal angiolipomas (SALs) are benign lesions consisting of mature adipose cells and blood vessels that vary in size from capillary to sinusoid or venular to arterial.1 The SALs are a specific, but uncommon clinico-pathological entity,1,2 and account for approximately 0.14-1.2% of spinal axis tumors, and 2-3% of extradural spinal tumors.3 Most SALs arise in the thoracic epidural space.3-5 They are further subdivided into non-infiltrating and infiltrating subgroups.6 An infiltrating SAL is an extremely rare benign tumor that tends to invade the surrounding soft tissue, and may potentially be mistaken for an aggressive tumor.6 There is no universal consensus on treatment of this rare lesion. Currently, the main treatment is total resection. This sometimes would be an aggressive option and not always achievable. Due to the rarity of this tumor, the best management option is yet to be determined. We report a rare case of spinal angiolipoma with extension to the intra-thoracic cavity through the neural foramina. We adopted the concept of maximum safe resection in the treatment of this benign tumor. The management options of infiltrating SALs were reviewed. Our objective in presenting this particular case is to highlight the diagnosis and therapeutic management options of infiltrating spinal angiolipomas.
Case Report
History and examination
A 50-year-old female patient was admitted to the hospital with a long-standing history (>10 years) of back pain in the mid-dorsal area. Eight months prior to admission, she experienced progressive lower limbs weakness and stiffness, the right leg more than the left. Functionally she remained able to walk with a support-walker frame. She also complained of pins and needles sensation in both thighs, and hesitancy in voiding. Physical examination revealed paraparesis more on the right side with hip flexion and knee flexion 3/5 pyramidal weakness, foot dorsiflexion 2/5, plantar flexion 2/5, whereas on the left lower limb there was hip flexion knee flexion, foot dorsiflexion, and plantar flexion 4/5. Sensory level was at D8 and below in the form of hypoesthesia, with severely impaired position sensation in the right lower limb, absent abdominal reflexes, hyper-reflexia in both lower limbs, and bilateral Babinski. Anal tone was preserved but with weak voluntary anal contraction.
Imaging findings
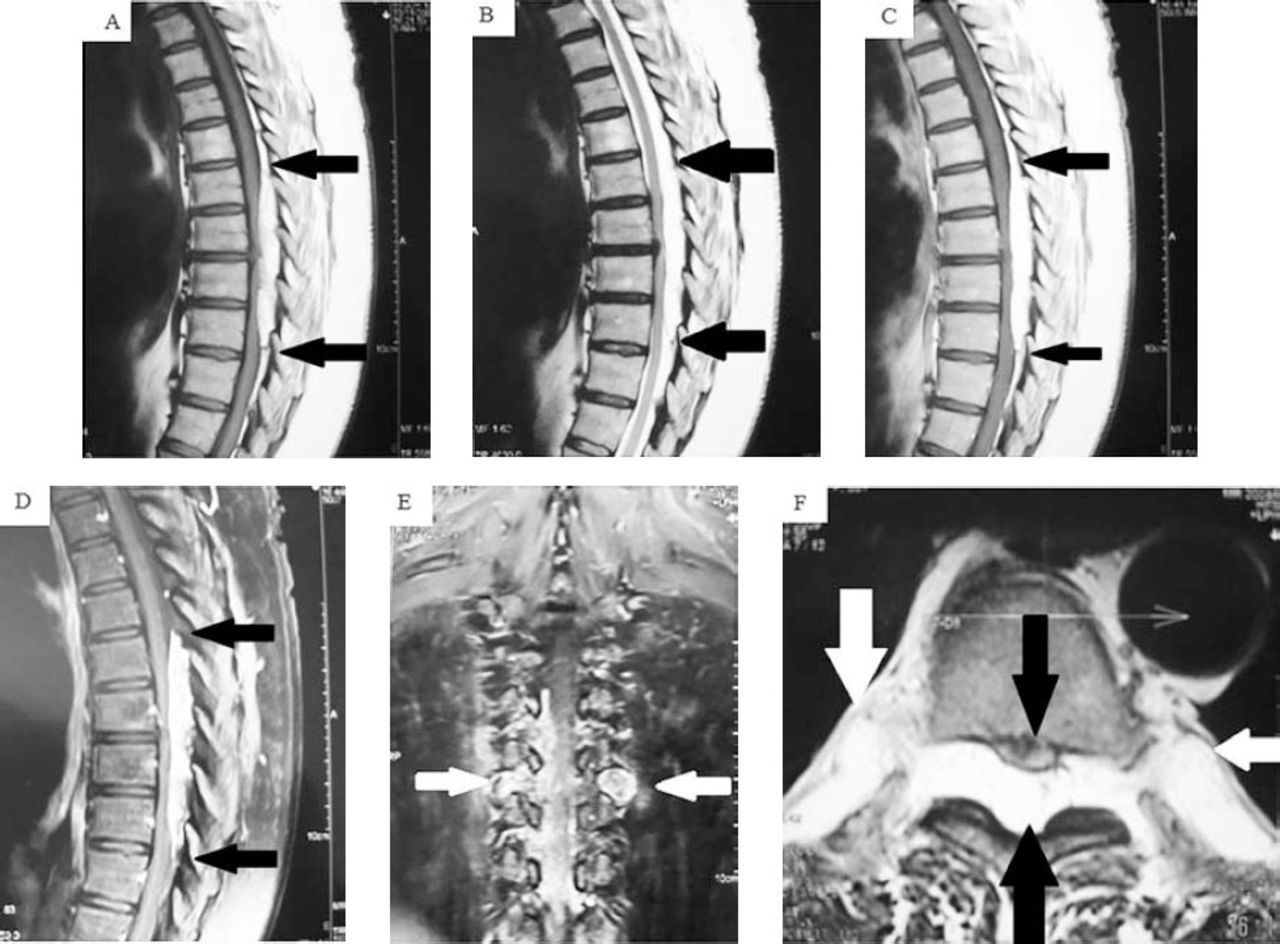
The MRI study showed a fusiform posterior epidural mass compressing the thoracic spinal cord over 4 vertebral body segments, T6 through T9. The mass was inhomogeneous, hyperintense on T1-weighted images (T1WI) (Figure 1A), hyperintense on T2WI (Figure 1B), inhomogeneously enhancing without and with fat-suppression T1WI (Figure 1C & 1D). The lesion’s long axis paralleled the long axis of the spinal cord, tapering at both ends. Compression and displacement of the spinal cord on the axial T2WI (Figure 1E) with extension into the thoracic cavity through the neural foramen were also depicted (Figure 1F).

Pre and post MRIs of the spine showing: A) Non-enhanced T1-weighted sagittal MRI of the mid-thoracic spine demonstrating an inhomogeneous mass, extending from T6-T9. The tumor shows predominant hyperintense fat component with small hypo-intense foci at the periphery. B) T2-weighted sagittal MRI again demonstrates predominant fat component of the lesion (between the black arrows). C) and D) Post-contrast T1-weighted sagittal MRI without and with fat-saturation showed avid inhomogeneous enhancement of the lesion. E) T2-weighted axial illustrates the mass along the posterior epidural spinal canal of the thoracic spine (lower black arrow), compressing and displacing the spinal cord anteriorly (upper black arrow), with bilateral extra-spinal extensions of the tumor (white arrows). F) Post-contrast coronal T1-weighted MRI with fat-suppression shows the bilateral extra-spinal extensions of the tumor (white arrows).
Surgery and postoperative course
She underwent T5 through T10 laminectomies. Total excision of the intra-spinal epidural component down to the neural foramina was achieved. The intra-thoracic part was left in place. Although the tumor was well vascularized, there was minimal blood loss during the tumor resection. At the time of surgery, the lesion was felt to be infiltrative in nature with ill-defined margins extending through the neural foramina and no discernible capsule was appreciated. After operation, she showed drastic improvement, and ambulated on the first post-operative day. The postoperative course was uneventful. At 6-months, 12-months, and 36-months follow-ups, she had mild residual spasticity and lower limbs hyper-reflexia with normal bladder function.
Histopathology
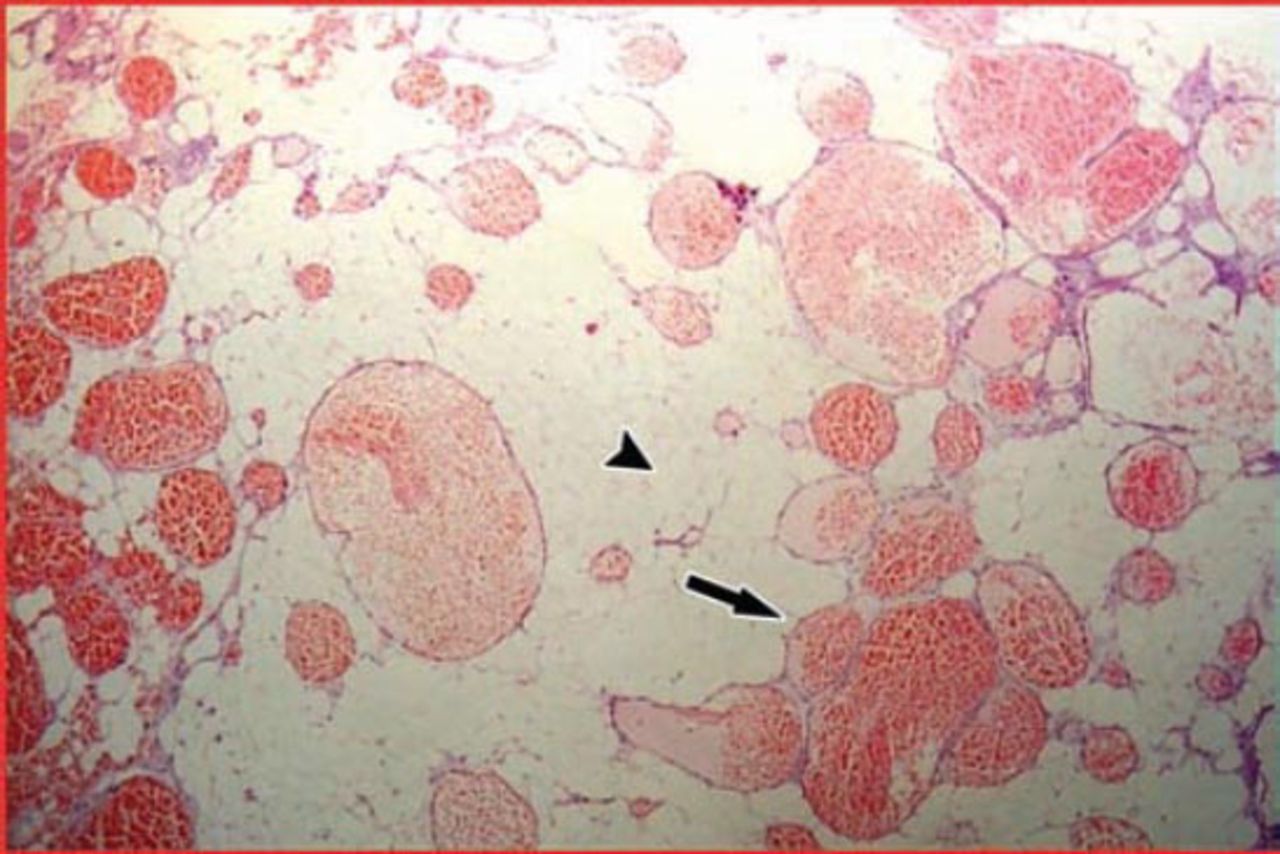
The sections revealed mature adipose tissue with many dilated vascular spaces containing blood, and lined by bland endothelial cells. A few blood vessels were capillary-sized with occasional fibrin thrombi; the majority was cavernous like. The features are consistent with angiolipoma (Figure 2).
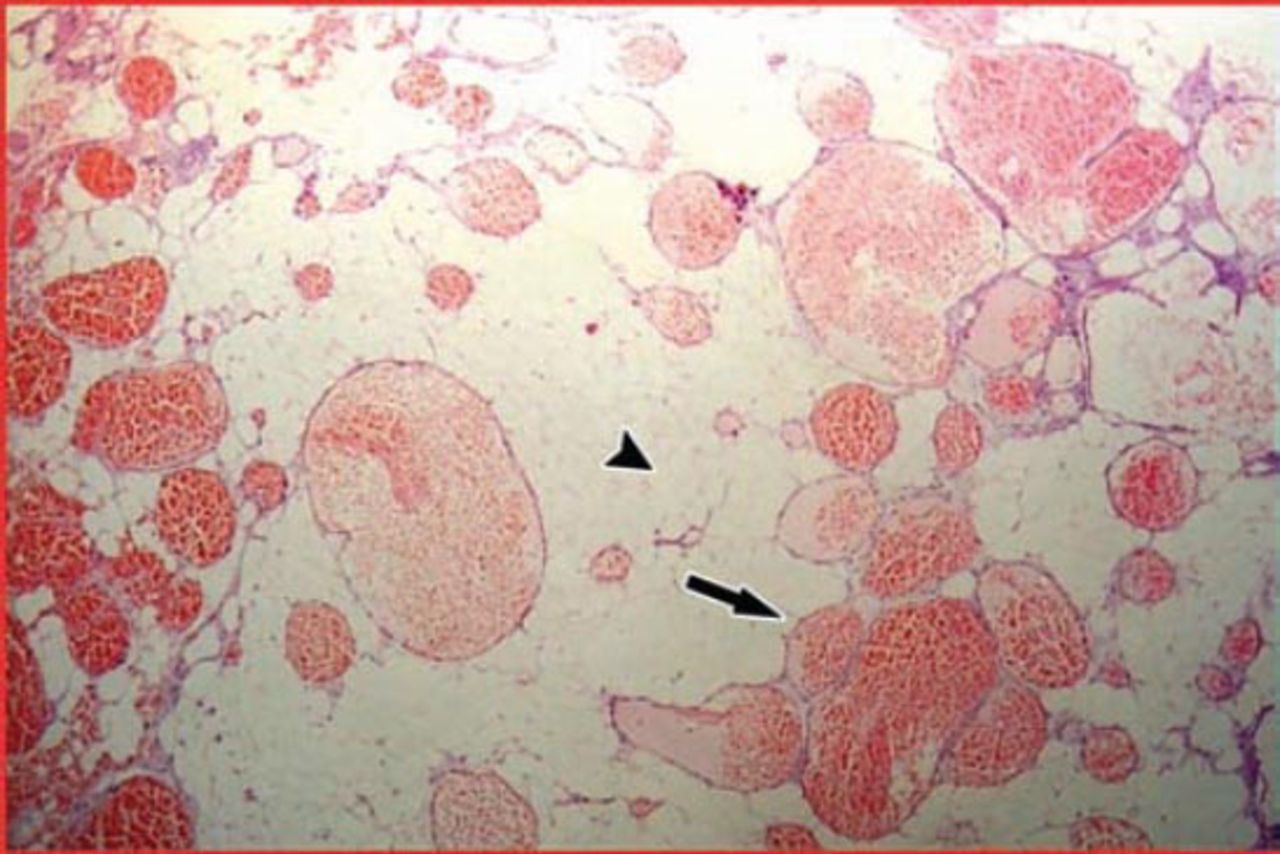
Surgical specimen. Hematoxylin and eosin stain; magnification × 40; microscopically, the tumor showed mature adipose tissue (arrowhead) interlaced with numerous blood vessels ranging from capillary to cavernous in size, and a few are irregular in shape (arrow).
Discussion
The first case of spinal angiolipoma (SAL) was reported in 1890 by Berenbruch et al3 in a 16-year-old patient with numerous cutaneous lipomas, while the first pathological report was made by Howard et al in 1960.7 Lin et al in 1974 classified SAL as non-infiltrating and infiltrating.8 The former is encapsulated and well demarcated, not infiltrating the dura or the vertebrae, often within the posterior epidural space. Whereas, the latter is entirely or partially unencapsulated, situated in the anterior or anterolateral aspect of the spinal canal with ill-defined margins and infiltrating the surrounding tissues. The origin and pathogenesis of SALs are unknown. There are several excellent reviews in the literature that discussed different aspects of SALs.3,6 To date, 145 cases of SAL have been reported.6,9 Approximately 70 of cases were diagnosed since the introduction of the MRI.6 Only 14 out of these 70 cases were infiltrating SAL, 13/14 were in the thoracic area (Table 1), and only one case (1/14) in the lumber region.6 Several other reports for infiltrating SALs (Gonzales-Crussi et al 1966,10 Pearson et al 1970,11 and Rivkind et al 198612) were reported before the MRI era, and they are well documented in Gelabert-Gonzalez et al 2009.3
Reported cases of infiltrating spinal epidural angiolipomas depicted with magnetic resonance imaging.
Histologically, the lesion is composed of mature fat cells and blood vessels. The fat composition is similar to the general adipose tissue, and the vascular components consist of capillaries, sinusoids, thin-walled blood vessels, or thick-walled blood vessels with smooth muscle and occasionally well-developed small arteries seen. A diagnostic feature is the presence of fibrin thrombi in the lumen of capillaries. Degenerative changes (myxoid changes and fibrosis) may be present in some longstanding cases.6 The SAL is considered a specific entity, different from pure spinal lipomas that may be associated with spinal dysraphism. The angiomyolipoma is a variant of angiolipoma characterized by vascular smooth muscle proliferation extending into the surrounding fat.
Clinical presentation
Most SAL occur in adults with an age range of 4 to 85 years.13 The peak incidence is in the fifth decade, with a mean age at presentation of 46 years.3 The SALs have been found to occur more predominantly in females (70 females, 48 males in one review3 that included all patients reported with SAL, and 22 females, 17 males in a review encompassing patients diagnosed with MRI studies6). The onset of presentation may be acute, subacute, or chronic in nature. The most common initial symptoms are lower extremity weakness and numbness and/or back pain (thoracic or lumber pain). Other symptoms like sciatica and gait disturbance have been reported. Progressive neurological symptoms secondary to spinal cord or nerve root compression may develop later. The symptoms usually evolve over months to years with a mean interval of 20.2 ± 9.6 months.3 However, vascular steal phenomena, vascular engorgement, venous stasis with thrombosis and bleeding into the tumor have been reported as causes of sudden deterioration and acute paraplegia.14 This was not the case in our patient.
Diagnosis
The MRI is the imaging modality of choice for detecting angiolipomas.6 The lesion signal characteristics vary greatly depending on the tissue components. It showed predominant high signal intensity on T1WI and T2WI due to the presence of adipose tissue and blood vessels. However, it is also reported to appear as an iso or even hypo-intense mass lesion on either sequences if the fatty component is less dominant than the vascular and fibrotic parts.4,6,15 Fat suppressed sequences, and post-contrast imaging are thus of tremendous help in diagnosing SAL in addition to the differentials, which usually include: spinal hemangiomas, melanomas, subacute hemorrhage, and extradural lipomatosis. The multiplanar acquisition is also very helpful in demonstrating the extra-spinal and trans-spatial tumoral extension (Figure 1E & 1F). Before the era of MRI, multiple other imaging modalities had also come into play including plain x-ray, CT, myelography, and others. Plain films are usually the primary tools for investigating non-specific back pain. However, in most cases they fail to detect any abnormalities, whereas in some cases, minor bony changes with flattening or even erosions of the pedicles and widening of the neural foramina might be appreciated. The CT scan can illustrate a fat density mass with possible linear enhancement of the vascular component. Bony changes are also better depicted by CT than by MRI or x-ray. However, CT appearances are often non-specific and may be misleading in some cases.
Treatment options
There is no clear consensus on what combination of therapy is optimal for SALs. The infiltrating and non-infiltrating SAL implicates different treatment approaches. Currently, the main treatment is total resection. Most non-infiltrative SALs are amenable to complete excision through a posterior approach via laminectomy. The extent of tumor resection in infiltrative SAL has been the subject of debate; the maximum safe resection is the most acceptable concept among most of the authors.3 Total removal of infiltrating SALs that involve the vertebral body has been recommended using the anterolateral transthoracic approach and stabilization of the affected vertebrae is desirable.3,6 The combined microneurosurgical posterior approach, and thoracoscopic approach whether in one session or as two-stage surgery, were used by Negri et al,16 and Gámez Garcia et al.17 This is the recommended approach especially for SALs with extra-spinal extensions “dumbbell lesions”.18 Several other authors reported good results by performing laminectomy via a posterior approach. A summary of therapeutic and surgical approaches for the 14 cases of infiltrative SAL is presented in Table 1.
Despite vascularization of the tumor, significant bleeding has been rarely reported.14 However, therapeutic pre-operative embolization was used by Rabin et al19 as the pre-operative tentative diagnosis of hemangioma. In case of recurring SALs, another resection is the main treatment. Although postoperative radiotherapy was administered in very few cases,3 no adjuvant radiation should be applied to this benign pathological entity, since even in the infiltrating group, the prognosis is very good. In fact, the recurrence is extremely rare even in cases in which a complete resection could not be attained.3
Most patients have a good prognosis, as SALs are usually slow growing and do not undergo malignant transformation. Most authors report good outcomes after surgical excision of SALs despite severe pre-operative neurological deterioration.3 In our case, we opted for a less aggressive surgical intervention by performing total excision of the intra-spinal canal component only. The patient’s clinical symptoms improved postoperatively. There were no signs of tumor recurrence, and no new neurological deficits during the 36-months follow-up period.
In conclusion, infiltrating SAL is an extremely rare tumor. It is considered a subgroup of SAL, which is a specific, clinico-pathological entity. The infiltrating type is entirely or partially unencapsulated. Typically, SALs show iso- or hyperintensity on T1WI, hyperintensity on T2WI and most lesions enhance with gadolinium administration. The recommended treatment is total surgical resection. The surgical approach can be individualized according to tumor extension and the bony and/or soft tissue involved by the tumor. Good results have been achieved by tumor subtotal excision. The adjuvant radiation therapy should not be used in treatment of patients with SALs, since the prognosis of the infiltrating group with incomplete resection, is very good.
Footnotes
Disclosure
The authors have no affiliation or financial involvement with organizations or entities with a direct financial interest in the subject matter or materials discussed in the manuscript. No funding was received for this work from any organization.
- Received July 16, 2014.
- Accepted February 16, 2015.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.