


Abstract
Subdural hematoma (SDH) caused by rupture of a cerebral aneurysm is rare and is usually associated with delayed diagnosis and treatment. We present a patient of a posterior cerebral artery aneurysm presenting as subacute SDH. The incidence, mechanisms and treatment of this condition are discussed.
In most cases, subdural hematoma (SDHs) are caused by head trauma. Subdural hematoma secondary to intracranial aneurysm rupture is uncommon, which account for 0.5-7.9% of all intracranial aneurysm rupture.1,2 Aneurysms of the posterior cerebral artery (PCA) comprise approximately 0.7-2.9% of all intracranial aneurysms.3,4 We report a case of subacute subdural hematoma secondary to PCA aneurysm rupture. Stent-assisted coil embolization is thought to be a safe and effective treatment for this situation. Also, the reason for presenting this case is to remind us of this condition, avoiding diagnostic and therapeutic pitfalls.
Case Report
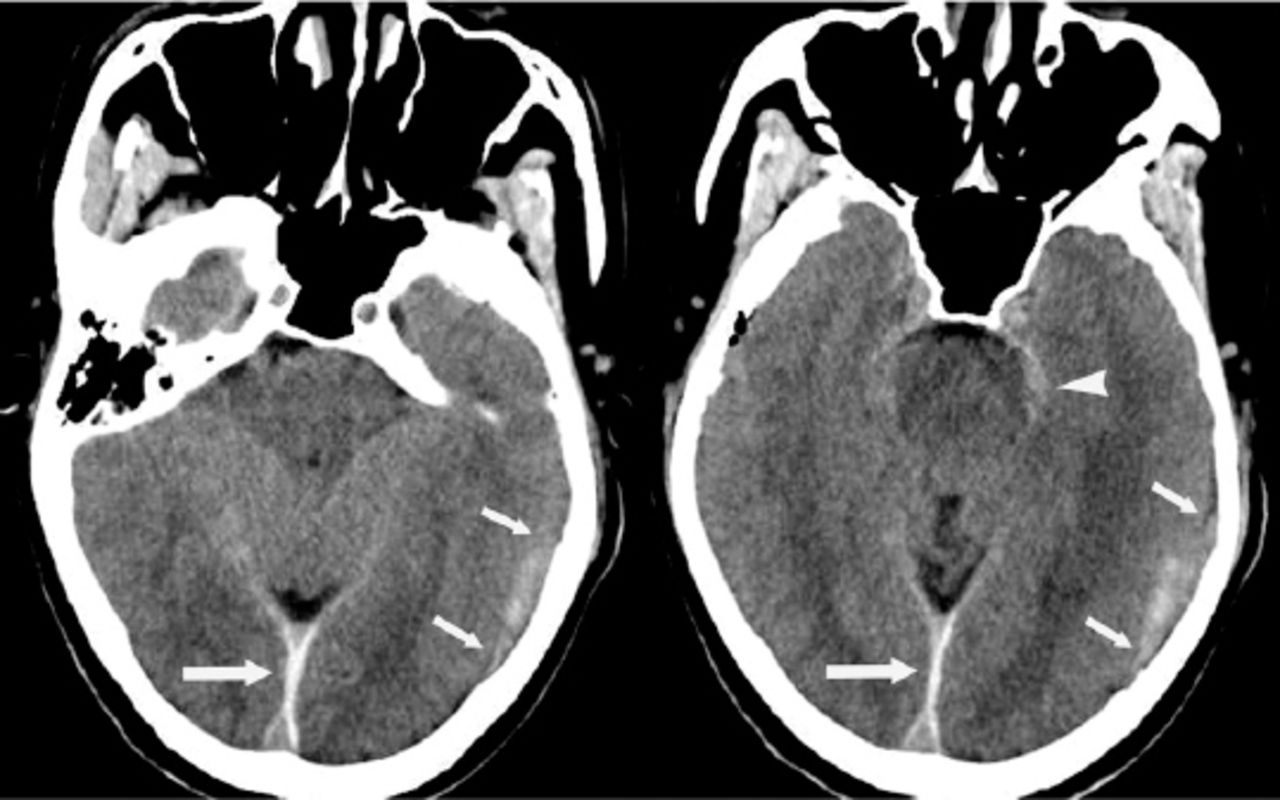
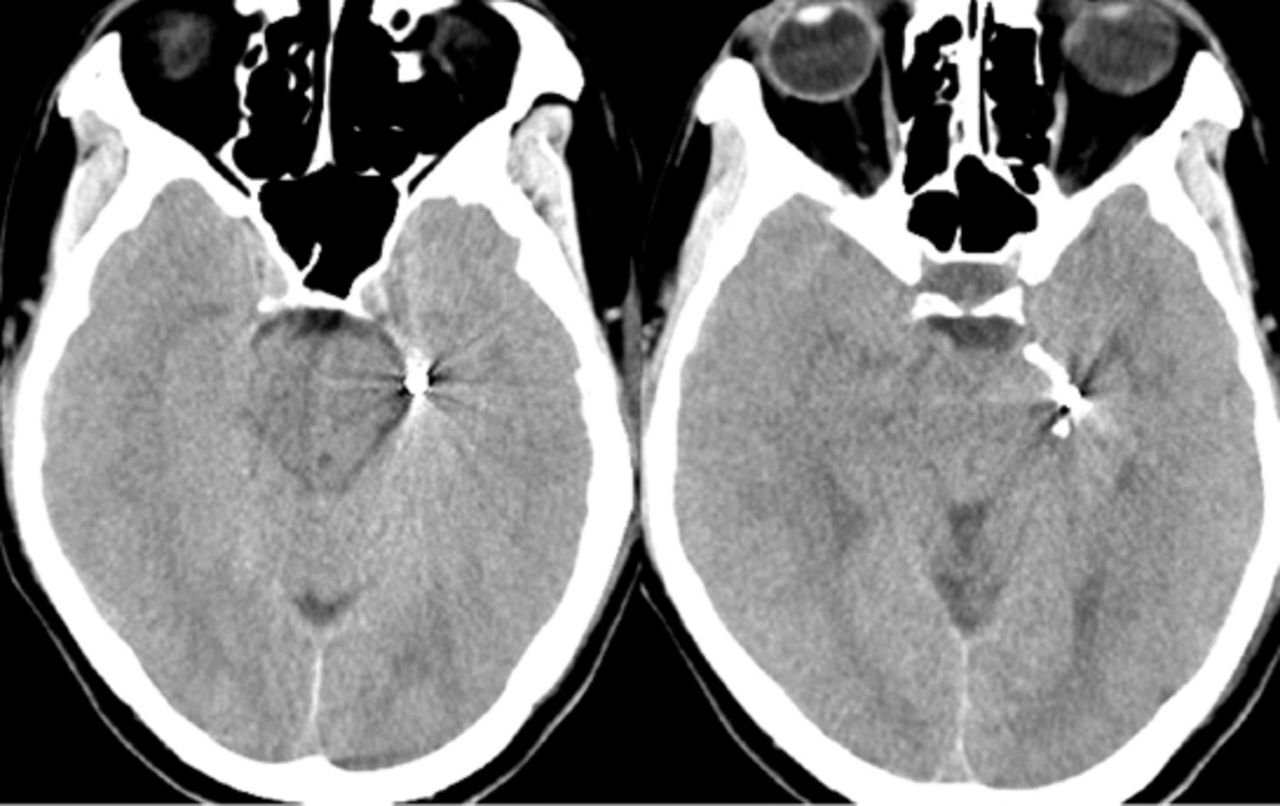
A 60-year-old hypertensive man with no history of head trauma presented with sudden headache and vomiting. four days later his symptoms suddenly worsened. He was admitted to our Department 5 days after the on-set of the symptoms. His past neurological history was unrevealing and there was no history of head trauma, blood clot disturbances, or anticoagulant therapy. His blood pressure was 172/100 mm Hg. Cranial computed tomography revealed subacute subdural hematoma in the left hemisphere, as well as interhemispheric subdural hemorrhage and minimal subarachnoid hemorrhage in the left perimesencephalic space (Figure 1). Computed tomography angiography (CTA) showed a fusiform aneurysm at the P2 segment of the left posterior cerebral artery (Figure 2A). He underwent stent-assisted coil embolization and post-embolization angiogram of the left vertebral artery showed the aneurysm was successfully occluded (Figures 2B&2C). But 3 days after the embolization of the aneurysm, he developed a change in mental status accompanied by slurred speech and narcolepsy. Emergency CT scan revealed enlargement of the left-sided subacute subdural hematoma with a new slight midline shift. Emergency drainage of the subdural hematoma SDH with a burr hole was performed. The patient’s neurological and functional status gradually improved and was transferred to local hospital for further rehabilitation 2 weeks after admission. Computed tomography scans 1 month after admission showing no abnormalities (Figure 3). And he was in further follow-up.
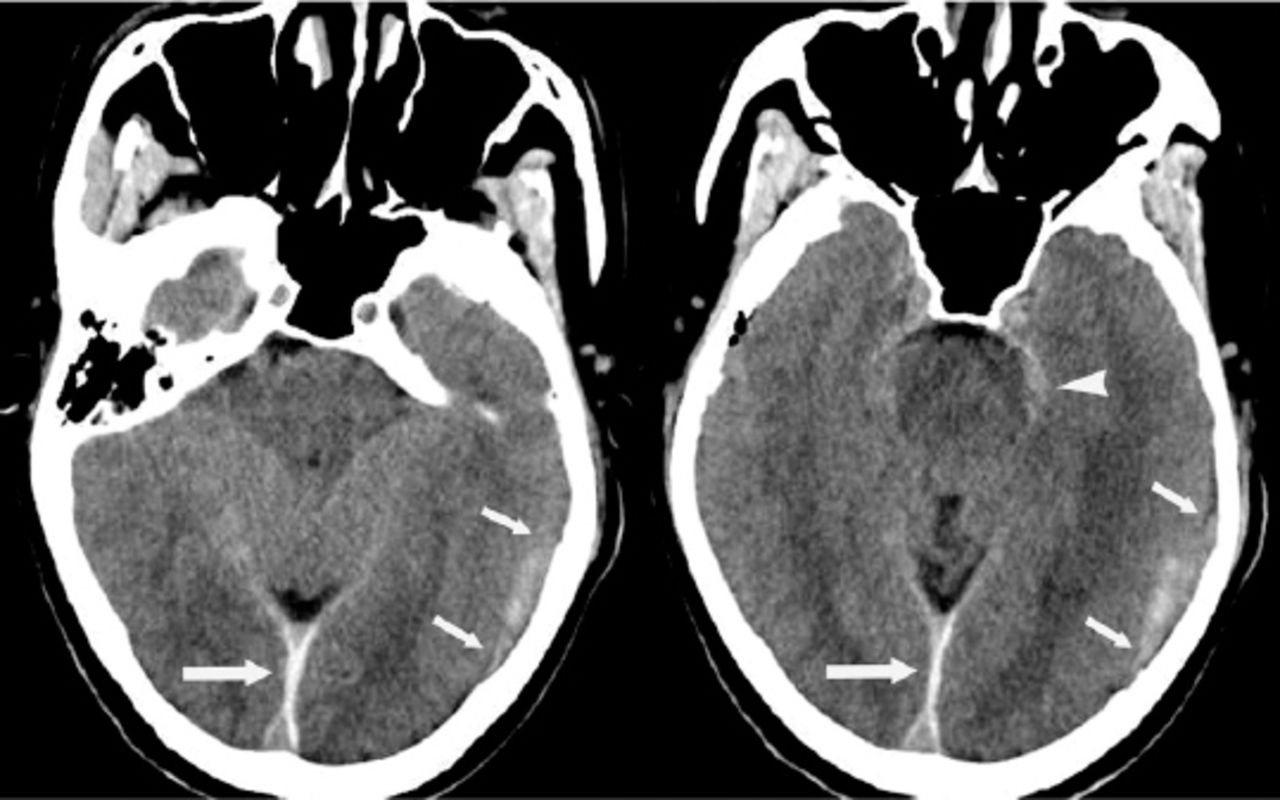
Computed tomography scans showing subacute subdural hematoma in the left hemisphere (short arrow), as well as interhemispheric subdural hemorrhage (long arrow) and minimal subarachnoid hemorrhage in the left perimesencephalic space (arrowhead).

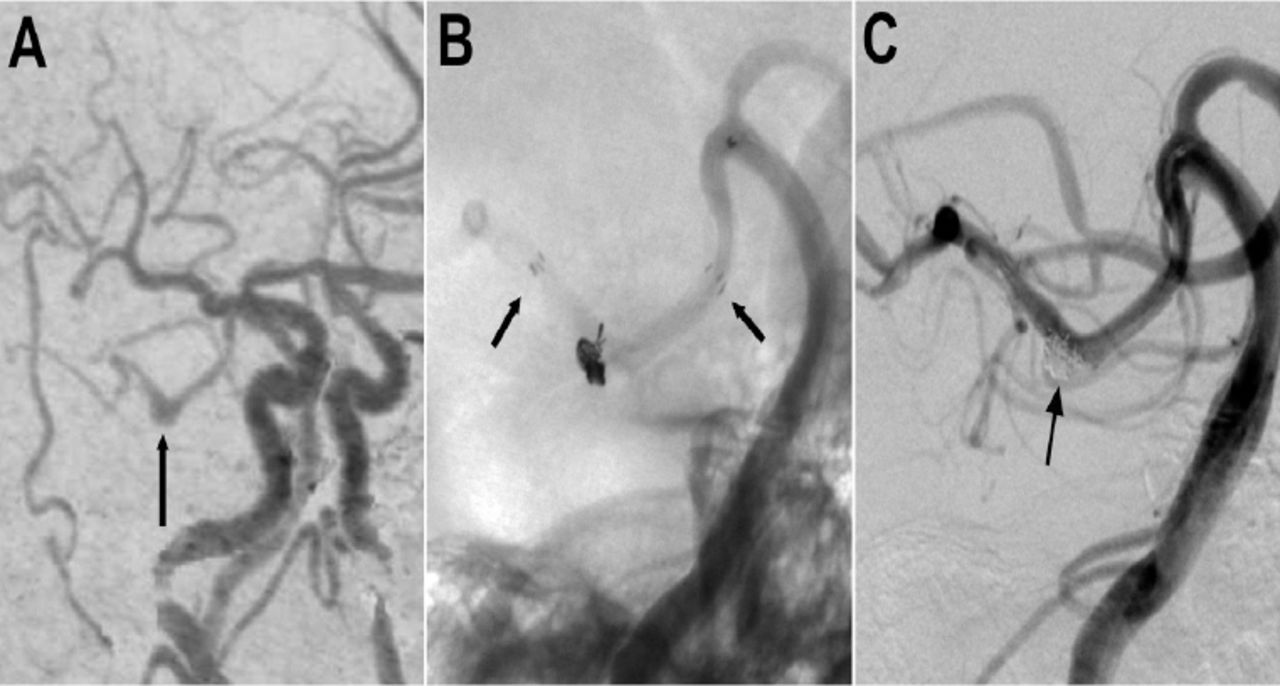
Computed tomography angiogram showing A) A fusiform aneurysm of the left posterior cerebral artery (arrow). B) Unsubtracted image before embolization showing the aneurysm treated by stent assisted coiling (arrows indicating the proximal and distal ends of the stent). C) Post-embolization angiogram of the left vertebral artery showing the occlusion of the aneurysm.
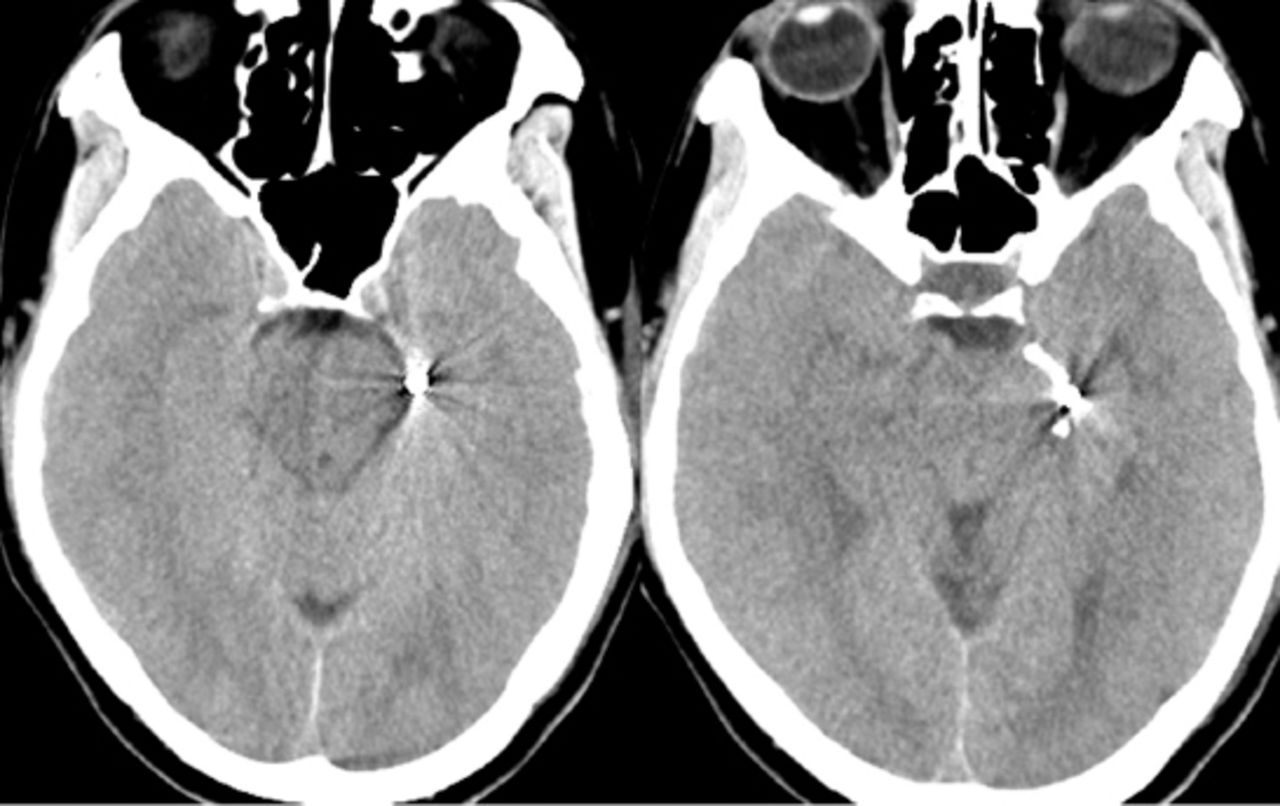
Computed tomography scans 1 month after admission showing no abnormalities.
Discussion
Intracranial aneurysm rupture is classically characterized by subarachnoid hemorrhage (SAH), and it is often complicated by intracerebral hematoma (ICH) and intraventricular hematoma (IVH). But the clinical incidence of SDH complication is very low, which was reported to be 0.5-7.9%.1,2 And the most frequently reported site of aneurysm location is the internal carotid artery (ICA)-posterior communicating artery, which is followed by aneurysms of middle cerebral artery and distal anterior cerebral artery.2,5 We described a case of ruptured PCA aneurysm presenting as subdural hematoma, which is relatively rare.
Several mechanisms have been proposed to explain the occurrence of SDH after aneurysm rupture:1,2,5,6 1)Successive minor bleedings case the developing of adhesions, resulting in final rupture into the subdural space; 2) high-pressure hemorrhage may lead to rapid accumulation of blood from the leaking aneurysm, rupturing the arachnoid membrane; 3) intracerebral hemorrhage may rupture through the cortex and cause a tear of the arachnoid membrane; 4) a carotid artery aneurysm arising from the part of carotid artery within the subdural space may rupture and cause subdural hematoma directly; and 5) the acute enlargement of the intracavernous aneurysm may erode the cavernous sinus wall. As in this case, the patient had suffered headache since 4 days before he was admitted to hospital, this warning sign may reflect the presence of successive small bleedings.
Whatever the cause, most cases of aneurysmal SDH show SAH on the CT scans, and this will address the diagnosis upon a vascular cause of hemorrhage. In a small percentage of cases, however, aneurysmal rupture can cause a subdural blood collection without SAH, a rare condition called pure SDH, which may lead to inappropriate diagnosis and management.1,7 Since cranial CT cannot reveal the cause of these pathologies, it is potential for such patients to undergo CTA or digital subtraction angiography as soon as possible to reveal the source of bleeding. Then appropriate therapy should be conducted depending on the location of the aneurysm and the clinical situation promptly.
Aneurysms of the PCA are rare. Because of the presence of complex perforating branches and adjacent to the cranial nerves, the surgical approach and exposure of the PCA is technically challenging.8 So endovascular treatment is relatively a safe and effective approach with low mortality and morbidity for these aneurysms.8,9 In this case we performed stent-assisted coil embolization to treat the aneurysm in the P2 segment of the PCA. Compared with the parent artery occlusion, the advantage of stent-assisted techniques is not only that the tight aneurysm packing with coils is attainable with less risk of coil migration or coil bulging into the parent artery, but that can preserve the parent artery, avoiding ischemic neurological events.10
Even though the patient did not undergo direct surgery, the subarachnoid hemorrhage in the left perimesencephalic space and the extravasation of the blood along the interhemispheric subdural space all suggest a causal association between the subdural bleeding and the aneurysm.
In conclusion, spontaneous arterial SDH due to a P2 segment of PCA has been rare reported earlier. We should be reminded that cerebral aneurysm rupture should be considered in spontaneous subdural hematoma, especially those with no evidence of subarachnoid hemorrhage, and the appropriate treatment should be planned with expediency
Footnotes
Disclosure
Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 12, 2015.
- Accepted July 8, 2015.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.