


Abstract
Objectives: To quantify the anatomic relationship between the Cervical pedicle screw (CPS), vertebral artery (VA), and related anatomic structures in the Saudi population.
Methods: This retrospective single center study included 50 consecutive patients (35 males) with normal neck findings on computed tomography angiography performed for trauma or vascular evaluation between 2012 and 2014. Radiologic parameters were assessed and correlated with age, weight, height, and body mass index (BMI).
Results: Mean age, weight, height, and BMI were 45.74±18.93 years, 79.72±21.80 kg, 164.74±11.53 cm, and 29.38±6.13 kg/m2, respectively. Mean cervical pedicle diameter (PD) increased from the cranial to caudal vertebrae (p=0.0001). Mean free zone (FZ) value, defined as the distance between the lateral CP border and medial VA border, was 1 mm (range 0.95–1.16 mm). The VA entry into the transverse foramina was at C6 level on both the right 92% and left side in most patients 94%. However, the right and left side level of VA entry differed in 14% of individuals.
Conclusion: The PD and FZ are smaller in Saudi Arabians than in western populations. Assessment of VA entry at each level should be performed on an individual basis as the level of VA entry can differ in the same patient. Anatomic variations between different geographic areas should be studied to provide better surgical guidance.
Cervical spine instrumented fusion is a common treatment for a variety of pathologic conditions.1 Several approaches for cervical spine stabilization have been developed, including anterior or posterior approaches.2-4 Currently, posterior fixation of the subaxial cervical spine is performed using lateral mass screws (LMS) or cervical pedicle screws (CPS).4 The CPS has the advantage of a stronger pullout strength than LMS.5,6 However, CPS is more technically demanding and is associated with a potentially higher risk of injury to the neurovascular structures.6-11 Precise anatomic knowledge is paramount for preventing a potentially life threatening vertebral artery (VA) injury during CPS insertion.12-15 The close proximity of the VA to the bony structures increases the risk of VA injury. Previously, anatomic studies identified a distance of 1–2 mm between the VA and the lateral wall of the cervical pedicle (CP).16 Additionally, the VA occupies one- to two-thirds of the axial diameter of the transverse foramen (TF), narrowing the space around the VA for potential screw misplacement.16,17 Additionally, variability in vertebral artery anatomy or osseous anatomy exists and should be assessed on an individual basis.16 Good knowledge of anatomic details combined with modern intra-operative imaging technology with navigation could reduce the risk of VA injury during CPS insertion.18,19 The purpose of this study was to quantify the relationship between anatomic structures of the subaxial spine and the VA and the CP in the Saudi population and to compare the results with published data from other geographic areas. These findings are relevant to the instrumentation of the spine, showing regional variations in the spinal anatomical structures measurement. Moreover, the data is critical for surgical planning, decision-making, and safety of cervical spine instrumentation.
Methods
Basic design and outcome
This retrospective study included 50 consecutive adult Saudi patients (35 males and 15 females) with normal computed tomography angiography (CTA) findings between 2012 and 2014. Indications for CTA served vertebral-basilar system evaluation in trauma, tumor, or suspected vascular insufficiency. Approval was obtained from the institutional review board prior to the beginning of the study. The main outcome of the study was the quantitative evaluation of the VA anatomy in relation to the CP and osseous structures relevant to CPS insertion from C3 to C7. A neuroradiologist, blinded to patient’s demographic data, assessed all CTA images for the included parameters. The CT machine used in this study was a GE LightSpeed 64-slice HD system (GE Healthcare, Wauwatosa, WI, USA) with targeted area slice thickness of 0.625 mm × 0.625 mm. Oblique axial and oblique sagittal reconstructions were performed using standard bone algorithm. Oblique axial images were reconstructed parallel to the superior and inferior border of each pedicle using AW VolumeShare 4.6 (GE Healthcare).
Demographic data including patients’ age, weight, height, and body mass index (BMI) were collected and correlated with anatomic variables of the cervical vertebrae. Height and BMI data were missing in 5 patients and weight was missing in 3 patients.
Radiologic variables. Assessment of osseous parameters
All included cervical spine levels, from C3 to C7, were assessed bilaterally. Cervical spine bony structures relevant to the VA, including the pedicle diameter (PD) at the isthmus, maximum transverse foramen’s coronal (TFC) and sagittal (TFS) diameters, maximum spinal canal’s coronal (SCDC) and sagittal (SCDS) diameters measured from bone boundaries, were evaluated.
Assessment of VA parameters and the free zone
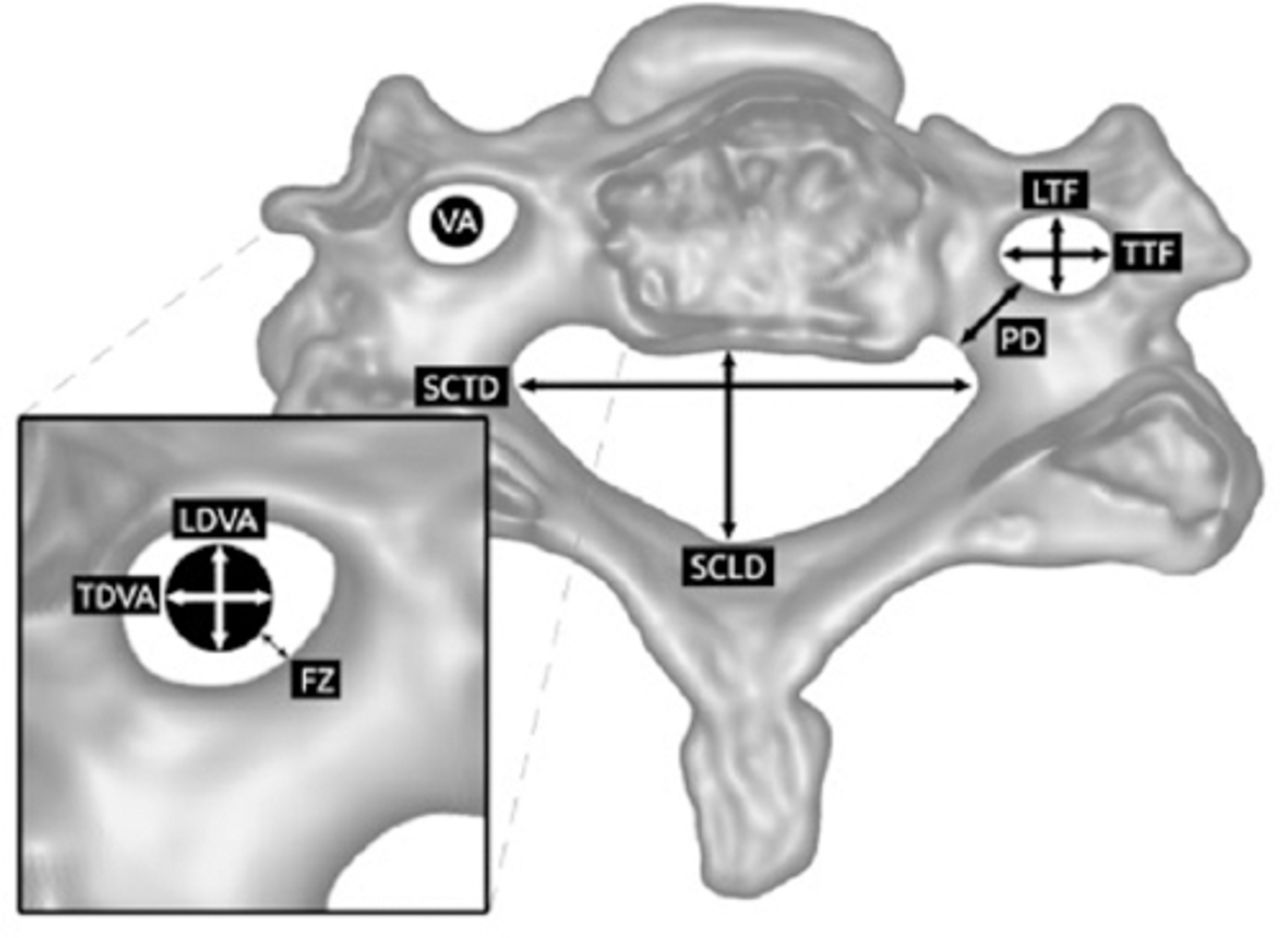
Variables concerning VA anatomy (Figure 1) were determined, including the lowest level of VA entry into the transverse foramina of cervical spine, and VA sagittal (VADS) and coronal (VADC) diameters. The free zone (FZ) (the space available for the CPS screw before it encroaches into VA following a perforation the lateral pedicle wall) was defined as the distance between the lateral pedicle border to the medial border of VA (Figure 1). Previous literature considered this space as a safety area for CPS.16,17 The FZ was examined from C3 to C6.
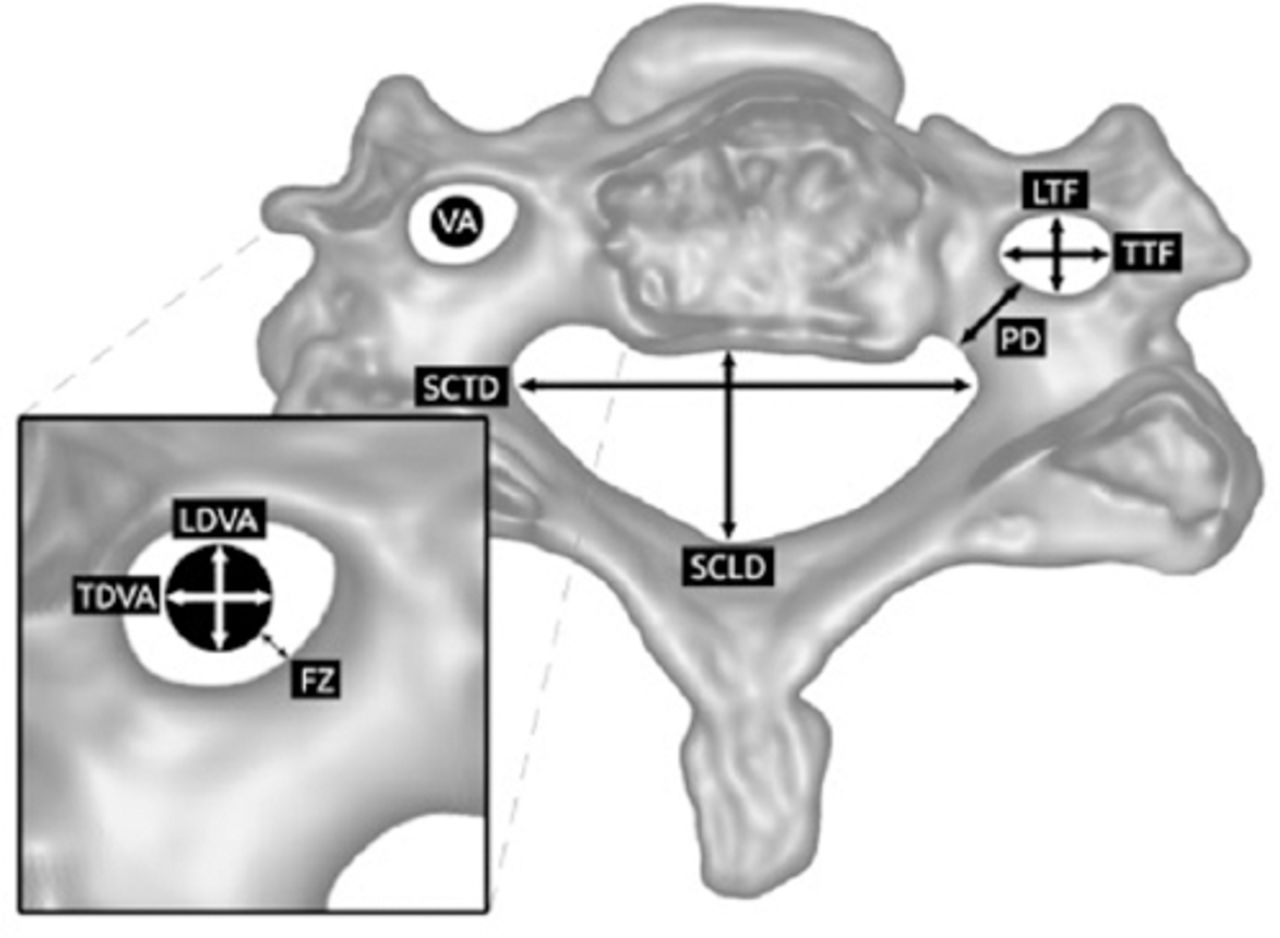
Radiological measurements of different parameters. TFC - transverse foramen on coronal image; FZ- free zone defined as the distance between the lateral border of the pedicle and medial border of vertebral artery (safe zone for pedicle screw insertion); PD - cervical pedicle diameter at the level of isthmus; SCDC - spinal canal diameter on coronal image; SCDS - spinal canal diameter on sagittal image, LTF - longitudinal diameter of transverse foramen, TTF - transverse diameter of transverse foramen, SCLD - spinal canal longitudinal diameter, SCTD - spinal canal transverse diameter, LDVA - longitudinal diameter of vertebral artery, TDVA - transverse diameter of vertebral artery
The VA occupancy was identified as the space in the TF that is occupied by VA. This was determined by determining the ratio of the VADC to the TFC. The following parameters were not measured due to technical considerations and were considered missing variables: SCDC in 4 patients, SCDS at C7 in 3 patients, and FZ at C6 in 5 patients.
Statistical analysis
Statistical analysis was performed using the Statistical Package for Social Science software (SPSS PC+ version 19.0; SPSS Inc., Chicago, IL, USA). Descriptive statistics (mean, standard deviation) were used. Paired t-test was used to compare between males and females and right and left sides. Pearson’s correlation coefficient was calculated to explore the relationship among different parameters and patient’s age and height at different levels from C3 through C7. A p-value < 0.05 was considered statistically significant.
Results
Patient demographics
The mean patients’ age, weight, height, and BMI were 45.74±18.93 years, 79.72±21.80 kg, 164.74±11.53 cm, and 29.38±6.13 kg/m2, respectively.
Relevant cervical vertebrae anatomy as demonstrated in Table 1, the mean PD increased significantly from the cranial to caudal vertebrae (from 4.29±0.81 mm at C3 to 5.78±1.02 mm at C7, p=0.0001). The TFC was significantly larger in the upper levels than in the lower levels (p=0001) (for example TFC measured 6.09±0.68 mm at C3 compared to 5.89±0.77 mm at C6 and 3.90±1.48 mm at C7).
Patients’ bone anatomy parameters at different levels of the cervical spine.
Spinal canal diameter variability between males and females at different cervical spine levels.
The mean SCDS, which represents the anterior-posterior diameter of the spinal canal, was significantly larger in males than in females at all levels (Table 3). The SCDC, which represents the transverse diameter of the spinal canal, was significantly larger in males at C4, C5, and C6 (Table 3). However, sex differences in spinal canal measurements were not adjusted for patients’ height, weight, BMI, or age.
Patients’ vertebral artery parameters at different levels of the cervical spine.
Quantified assessment of cervical VA anatomy
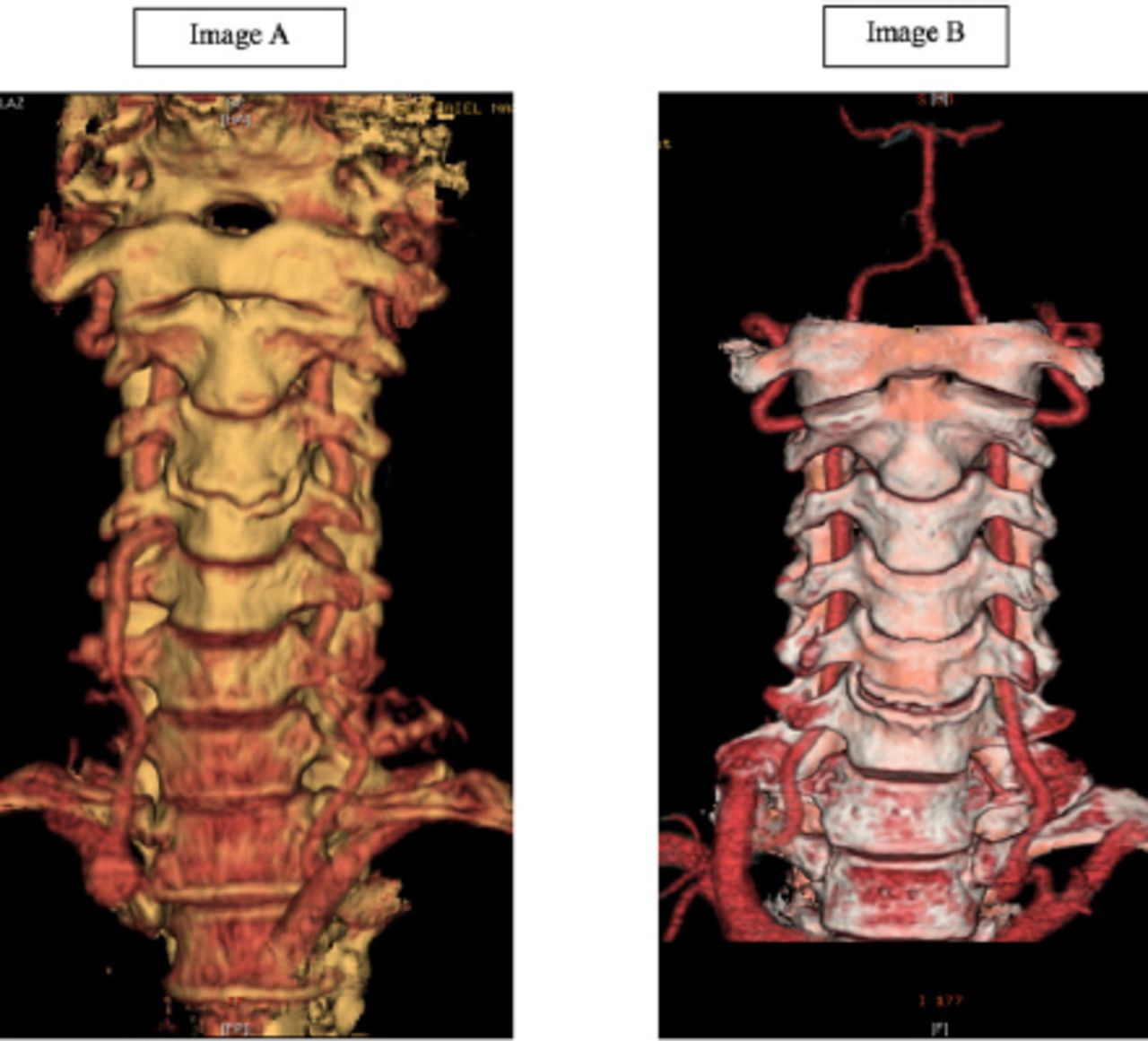
A summary of included parameters is presented in Table 1. The transverse diameter of the VA (represented in this study on the coronal view as the VADC) was significantly variable among the different levels, for example VADC measured 3.83 mm at C7 compared to 3.58 mm at C3 (p=0.001). This sub-millimeter difference in VA status however, could be attributed to VA pulsation difference during image acquisition. The VADC was significantly larger in males than in females in both the right (p=0.001) and left sides (p=0.005) (Table 2). The level of VA entry into TF on the right side was mostly at C6 (92%) followed by 4% at C5, and 2% at both C4 and C7. On the left side, VA entry was mostly at C6 (94%), followed by 4% at C5, and 2% at C4. Within individual cases, VA level of entry was variable in 14% when comparing right to left sides (Figure 2A and B).
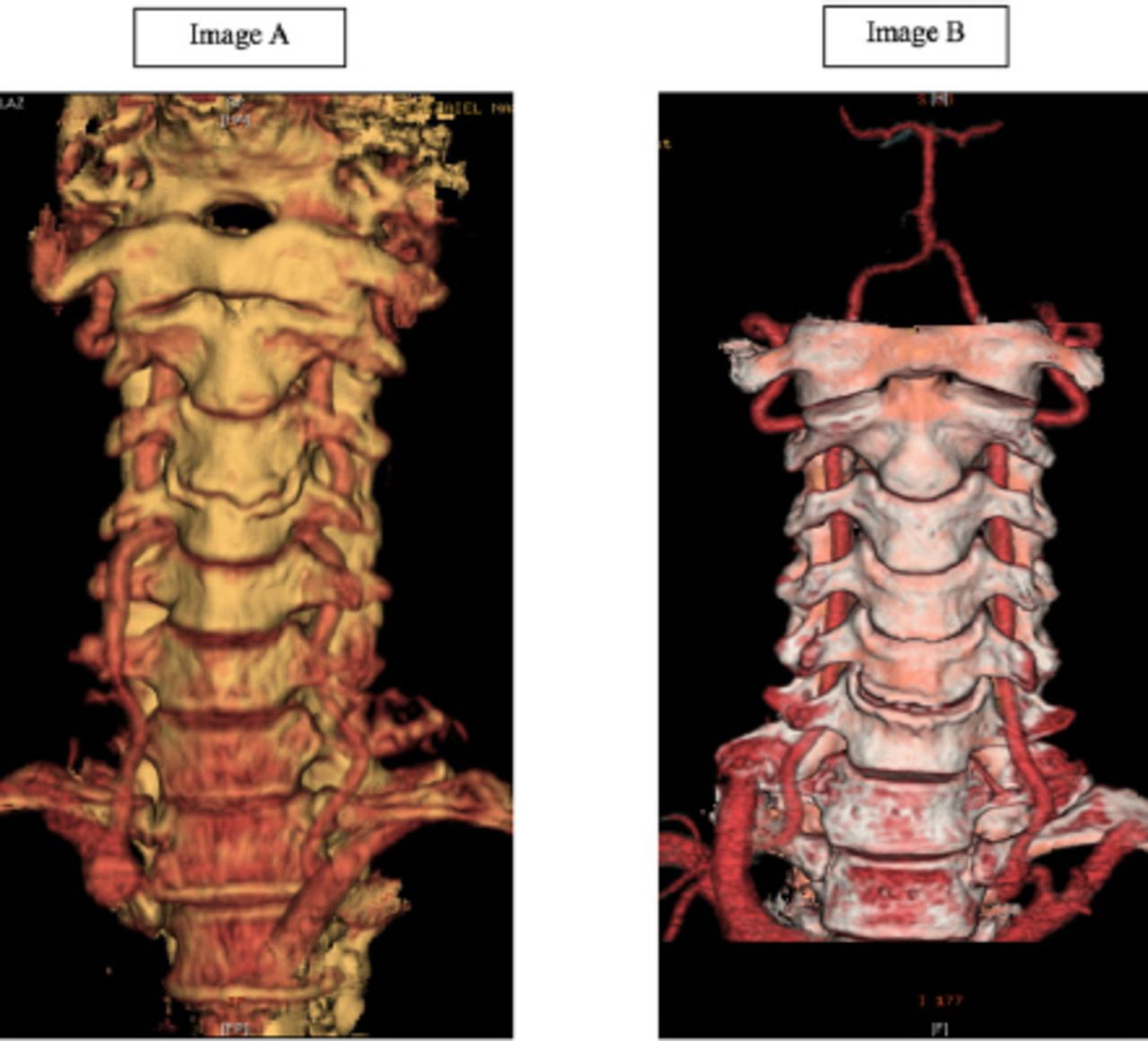
Vertebral artery entry to the transverse foramina of the cervical spine at different levels within the same patients. Image A shows VA entry at C6 level on the left side and at C4 level on the right side. Image B shows another patient with VA entry at C5 level on the left side and at C6 level on the right side.
Significantly more space surrounded VA within TF in the upper cervical spine compared to lower cervical spine (VADC/TFC ratio was 58.78% at C3 vs. 63% at C6, p=0.028). This is probably related to the decreasing diameter of the transverse foramen (TFC) from cranial to caudal direction (Table 1). On the other hand, FZ was around 1 mm across all levels (Table 1), with no significant differences between the right and left sides (Table 3).
Correlation between patient demographic data anatomic variables
The PD was larger as the patient’s height increased; only C3, C4, and C5 demonstrated a significant correlation (p=0.002, 0.023, and 0.014 respectively). On the other hand, PD did not correlate significantly with the patients’ weight or BMI. The TFS and TFC increased significantly with increased patients’ height at all levels (p=0.005 and 0.0001 for TFS and TFC respectively at C3 level; p=0.005 and 0.0001 for TFS and TFC, respectively, at C4 level; p=0.008 and 0.004 for TFS and TFC, respectively, at C5 level; p=0.004 for both TFS and TFC at C6 level) except for C7 level (p=0.588 and 0.436, respectively).
Parameters for spinal canal diameter were smaller with advancing age; however, significant correlations were identified only for SCDS at C3 level (p=0.025) and SCDC at C6 level (p=0.045). The spinal canal diameter (both SCDC and SCDS) significantly increased with increasing patient height at all levels (p=0.018 for SCDC at C3 level; p=0.0001 and 0.047 for SCDC and SCDS, respectively, at C4 level; p=0.0001 and 0.023 for SCDC and SCDS, respectively, at C5 level; p=0.001 and 0.019 for SCDC and SCDS, respectively, at C6 level; p=0.038 and 0.041 for SCDC and SCDS, respectively, at C7 level) except for SCDS at C3 level (p=0.86). On the other hand, significant positive correlation between patient’s weight and spinal canal measurements was only found for the levels of C5 (p=0.031) and C6 (p=0.043). No correlation was found between spinal canal diameter and BMI. The FZ was not related to patient’s age, height, weight, or BMI.
Discussion
Cervical pedicle diameter at the level of isthmus and FZ
Instrumentation of the cervical spine requires precise knowledge of the patient’s anatomy, inclusive geographical anatomical variations. The findings of the present study agree with those of previous studies in terms of variability in the anatomy of the cervical spine in different geographic areas.6,11,21-23 The PD in the current study population was smaller than that reported by western literature (4.29 mm at C3 level and 5.78 mm at C7 level vs. 4.5 mm at C3 level and 6.5 mm at C7 level).6,16 The PD in our study population was also smaller than that reported in the Korean publication (4.29 mm vs. 5.67 mm at C3 level).24 Furthermore, the FZ, measured during CPS insertion, was smaller in the current study population than that reported in published data on western populations. For example, FZ at C6 level was 0.99 mm in the current study and 1.7 mm in western population.16 On the other hand, FZ measurement from this study was comparable to data for the Chinese population.25 In addition, the current study demonstrated a higher ratio of TF occupation by the VA, from C3 to C6 level, compared to that in published data (58.8% to 64.3% vs. 36.5% to 34.5% respectively).16 The smaller pedicle size and narrow FZ demonstrate a potentially higher risk for CPS insertion. While larger sample size may be more representative of the true measurements of cervical spine anatomy in a particular population, the current study demonstrates that knowing regional antomic differences is essential when planning for instrumentaion.
Variability in the entry of the VA into the cervical spine
Careful study of the anatomy of individual cases is necessary to avoid VA injury during anterior or posterior cervical spine instrumentation.26 Variability in VA anatomy was found in the current study and in published literature.16 VA entry into the TF of the cervical spine was found mostly at the C6 level (93% of patients) in the present study and in up to 95.6% of patients in publishes studies.16, 27 However, both sides should be carefully assessed given the 14% variability in the VA entry into the TF within the same patient. The left VA was dominant in 64% of our cases, which is similar to that in published data.16
Outcome of cervical pedicle screws
Cervical pedicle screws technique was first used clinically by Abumi et al28 in 1994 for cervical spine fractures. Cervical pedicle screws insertion for cervical spine fixation has several advantages and potential risks. Cervical pedicle screws fixation provides better biomechanical stability and pullout strength.3 It has a significantly higher load-to-failure resistance than LMS fixation, with a lower risk of screw loosening.6 However, CPS fixation is not without risks, VA injury being the most critical and life-threating complication.20 In their study of 207 pedicle screws in 64 patients, 78.5% of CPS insertions in the subaxial spine were associated with pedicle wall perforation within 2 mm.29 Three of their patients had VA injury, which resulted in death in one case. In a systematic review, Yoshihara et al20 reported superior biomechanical properties for CPS than LMS fixation with a higher risk of VA injury (0.15% vs. 0%, p=0.012).3
Relevance of patient demographic data
The PD was found to correlate with the height of the individual in our study population. Ample literature is available regarding stature estimation from bone measurements in different geographic areas in forensic literature since 1952.30-36 Many studies used CT and magnetic resonance imaging measurements.37-39 Estimation of individual’s height was possible from analyzing the cervical and lumbosacral vertebrae.37-41 Considering the current study findings, the relatively smaller measurements of the concerned anatomic bony structures could be related to the smaller population height in this study’s geographic area compared to western population.42
Study limitations
The present study was limited by several factors that have to be considered when interpreting the results. The number of patients recruited may not represent the population at large. However, it brings the attention of the operating surgeons to review individual patient’s characteristics and not rely only on published data. It also encourages larger studies addressing spine anatomy variability. In addition, measurement reliability was not addressed and variability could exist between different individuals. The measurement of the VA diameter could also be variable, given the variability of the arterial pulsation. However, such variability is not possible to assess using current imaging technology. The surgeon should keep such factors in mind while addressing the exact location of the VA during cervical spine surgery.
In conclusions, PD is smaller in the Saudi population than in western populations. An approximately 1 mm safety zone is available for CPS insertion in the subaxial cervical spine. The PD has a direct relationship with body height. Assessment of VA entry in each level should be performed on an individual basis, as different levels of VA entry in the same patient can occur. Further studies in different geographic areas with larger sample sizes are necessary for better assessment and guidance of cervical spine surgical procedures.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.This research was supported by the College of Medicine Research Center, Deanship of Scientific Research, King Saud University, Riyadh, Kingdom of Saudi Arabia.
- Received September 25, 2017.
- Accepted November 29, 2017.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.