


Abstract
Objectives: To investigate the neuroprotective effect of Astragalus injection in a spinal cord ischemia-reperfusion (I/R) injury model.
Methods: A total of 27 Sprague Dawley rats were randomly divided into 3 groups: control group (n=3), I/R group (n=12), and Astragalus injection group (Ast group, n=12). Spinal cord ischemia was induced by occlusion of the abdominal aorta above the right renal artery for 32 min. Animals in the Ast group were administered Astragalus injection (6.42 mL/kg) at 30 min before the induction of ischemia. After reperfusion for 8, 12, 24, or 48 hours, the serum neuron-specific enolase (NSE) concentration was measured by enzyme-linked immunosorbent assay (ELISA) and the aquaporin-4 (AQP4) protein level was detected by western blotting.
Results: The pathological changes, as assessed by hematoxylin and eosin (HE) staining, were milder in the spinal cords of the Ast group compared to the I/R group. Enzyme-linked immunosorbent assay demonstrated that the NSE concentration of the Ast group was significantly lower than that of the I/R group (p<0.05). However, the NSE concentrations of the I/R and Ast groups were significantly higher than that of the control group (p=0.05). Additionally, the expression of AQP4 in the Ast group was lower than that of the I/R group at each time point.
Conclusion: These findings indicate that Astragalus injection has a neuroprotective effect in spinal cord I/R injury by decreasing the AQP4 expression.
Spinal cord ischemia and the resulting paraplegia are devastating complications that can occur following thoracic and thoracoabdominal aortic interventions as well as decompression spinal canal stenosis.1,2 In addition to the physical impact, paraplegia is usually associated with psychological and economic burdens that affect patients as well as their family members. The past few decades have witnessed considerable medical advances that have decreased the rate of spinal cord ischemia and paraplegia.3,4,5 Various methods have been proposed to reduce the risk of paraplegia, including ischemic preconditioning, moderate hypothermia, antioxidants, steroids, and calcium channel blockers.6 Nevertheless, none of these methods can completely prevent the development of paraplegia, and the current incidence rate ranges from 5% to 10%. Astragalus injection is an aqueous solution extracted from the Chinese herb Astragalus membranaceus.7 The main components of Astragalus injection include Astragalus saponins (astragaloside I, astragaloside II, and astragaloside IV) and flavonoids (formononetin, ononin, calycosin, and isoflavane).8 Astragalus injection is a stable pharmaceutical product; the concentration of Astragaloside IV (C41H68O14) in Astragalus injection should be no less than 0.08 mg/mL, according to the quality control standard of the Ministry of Health of the People’s Republic of China.9 Astragalus has been widely used in China for a wide array of conditions, including the treatment of diabetes and stroke.10,11 Additionally, recent reports have suggested a possible neuroprotective effect for Astragalus injection.12,13 Therefore, in this study, we aimed to investigate the neuroprotective function of Astragalus injection in spinal cord ischemia-reperfusion (I/R) injury in rats and to explore the underlying mechanism.
Methods
Animals
A total of 27 adult Sprague Dawley rats were obtained from the Experimental Animal Center of Hubei University of Traditional Chinese Medicine (Wuhan, China) in July 2014. All animals were clinically healthy, weighing 0.3–0.4 kg (369.23±35.99 g) and were allowed free access to food and water. The rats were handled in accordance with the Guidelines for the Care and Use of Laboratory Animals, and the experimental protocol was revised and approved by the Ethics Committee of the Faculty of Medicine, Xiangyang Central Hospital (Affiliated Hospital of Hubei University of Arts and Science), China. All measures were undertaken to minimize animal discomfort.
Spinal cord I/R model
The spinal cord I/R model was established by occlusion of the abdominal aorta, as described previously.14,15 Briefly, rats were anesthetized by an intraperitoneal injection of 1% sodium pentobarbital (40 mg/kg) under sterile conditions. Next, spinal cord ischemia was induced by occlusion of the aorta above the right renal artery for 32 min. Reperfusion was performed by removing the blood vessel clamp for 8, 12, 24, or 48h. Finally, the rats were administered cefalotin immediately after the operation by intramuscular injection. The rats were divided into the following groups: control group (n=3); 32I/8hR group, 32 min of ischemia and 8 h of reperfusion (n=3); 32I/12hR group, 32 min of ischemia and 12h of reperfusion (n=3); 32I/24hR group, 32 min of ischemia and 24h of reperfusion (n=3); 32I/48hR group, 32 min of ischemia and 48h of reperfusion (n=3); Ast/32I/8hR group, Astragalus injection pretreatment, 32 min of ischemia, and 8h of reperfusion (n=3); Ast/32I/12hR group, Astragalus injection pretreatment, 32 min of ischemia, and 12h of reperfusion (n=3); Ast/32I/24hR group, Astragalus injection pretreatment, 32 min of ischemia, and 24h of reperfusion (n=3); and Ast/32I/48hR group, Astragalus injection pretreatment, 32 min of ischemia, and 48h of reperfusion (n=3). The animals in the Ast groups were administered Astragalus injection (6.42 mL/kg16, Shineway Pharmaceutical Group Co. Ltd., Z13020999) at 30 min prior to ischemia induction; while the rats in the groups without Asp pretreatment were intraperitoneally administered 0.9% sodium chloride (6.42 mL/kg) at 30 min prior to the induction of ischemia.
After the specific reperfusion interval (8, 12, 24, and 48h), the rats were deeply anesthetized for a thoracotomy. Homeostasis was maintained with 4 mL of blood extracted from the inferior vena cava. Next, the rats were transcardially perfused with 0.9% saline until the perfusate was clear and the liver as well as the sclera were pale. The L2–L4 segments of the spinal cord were dissected and divided into 2 portions. One part was preserved in -80°C for western blot analysis, and the second portion was fixed in 4% paraformaldehyde for hematoxylin and eosin (HE) staining. Blood samples were placed at room temperature for 2h and then centrifuged at 3500 rpm for 5 min to collect the serum, which was stored at -20°C until further analysis.
Hematoxylin and eosin staining
Spinal cord specimens were fixed in 4% paraformaldehyde for 48h. After dehydration in gradient ethanol solutions, samples were embedded in paraffin and sectioned at a thickness of 5 µm. Next, the slides were rehydrated and stained with HE, according to standard protocols. Neuronal injury was evaluated with light microscopy by an experienced pathologist in a blinded manner.
Measurements of neuron-specific enolase (NSE) by enzyme-linked immunosorbent assay (ELISA)
Assessment of NSE levels was performed using a commercially available Rat NSE ELISA Kit (Elabscience Biotechnology Co., Ltd.: E-EL-R0058c), according to the manufacturer’s protocol. The rat NSE antibody was coated on the enzyme-labeled plate, and the samples were added to the coated plate. Subsequently, the samples were incubated for 60 min with a horseradish peroxidase-conjugated secondary antibody, followed by colorimetric detection at 450 nm.
Western blotting
Western blot analysis was performed to investigate the expression of aquaporin-4 (AQP4) protein in the injured spinal cord extracted at 8, 12, 24, or 48h after spinal cord ischemia. Protein homogenates of the spinal cord samples were prepared by rapid homogenization in 10 volumes of lysis butter. Samples were centrifuged at 12,000×g for 5 min, and the protein concentration was determined. The prepared protein lysates (50 µg/lane for each sample) were fractioned on 10% sodium dodecyl sulfate-polyacrylamide gels and transferred to nitrocellulose membranes. These blots were incubated with the rabbit polyclonal antibody anti-AQP4 (1:800, Abcam: ab156924), and the AQP4-positve bands were visualized by an enhanced chemiluminescence kit (ECL kit, Boster Biological Technology Co. Ltd.: BA1054), according to standard protocols. The AQP4 protein bands and cytoplasmic actin bands were scanned using Bandscan software, and the gray-scale values of the bands were calculated.
Statistical analysis
Statistical analysis was performed using the Statistical Package for the Social Science version 16.0 (SPSS Inc., Chicago, IL, USA). Statistical evaluation of the data was performed by one-way analysis of variance and the t-test. Data are presented as the mean±standard deviation. A value of p<0.05 was considered statistically significant.
Results
Hematoxylin and eosin (HE) staining
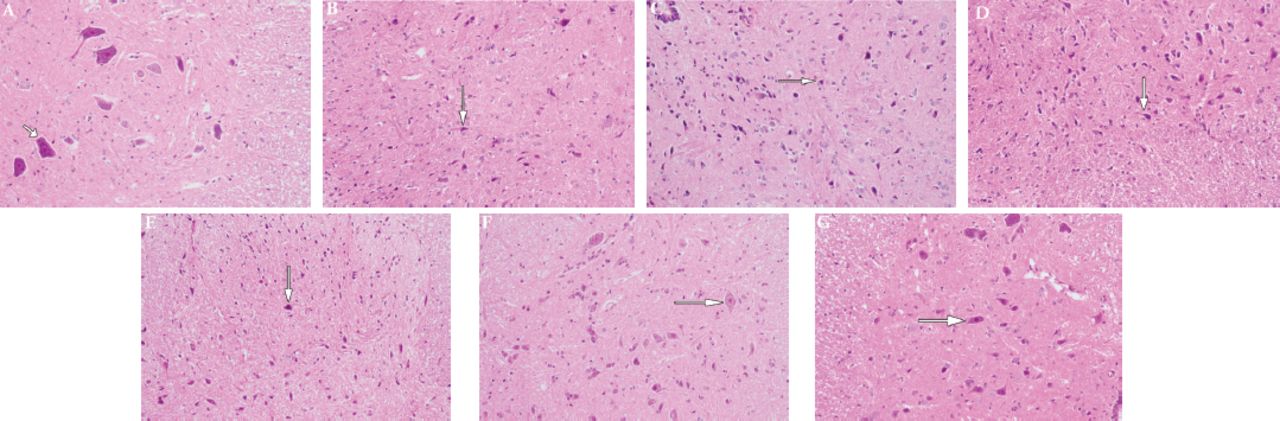
Spinal cord I/R injury was carried out by occlusion of the aorta followed by different reperfusion periods (8, 12, 24, and 48h). Hematoxylin and eosin staining was used to monitor the histopathological changes among the different groups. In the control group, HE staining demonstrated a normal spinal cord tissue structure without bleeding, edema, or other abnormalities. The nerve cells had a clear outline with round nuclei as well as clear and visible nucleoli. The Nissel bodies were stained as blue reticular structures that were arranged evenly around the nucleoli, and the cytoplasm was evenly stained (Figure 1A).

HE staining of rats spinal cord A) Representative HE staining of control spinal cord tissue. Representative HE staining of spinal cord tissue from the ischemic group when ischemia was induced for 32 min, followed by a B) 12-h, C) 24-h, or D) 48-h reperfusion period. Representative HE staining of spinal cord tissue from the Astragalus-treated group. Astragalus injection was administered 30 min before ischemia induction (32 min) followed by a E) 12-h, F) 24-h, or a G) 48-h reperfusion period. All images are shown at 400× magnification.
Following a 12-h reperfusion period, HE staining revealed shrunken and degenerated neuronal cells. Additionally, the neuronal cells had a necrotic appearance, with evident glial hyperplasia. Moreover, neutrophils were observed in the spinal cord tissue (Figure 1B). After 24h of reperfusion, neuronal necrosis was more evident in the rat spinal cord, with glial proliferation. Furthermore, signs of hemorrhage and neutrophil infiltration were observed in the spinal cord gray matter (Figure 1C). Following 48h of reperfusion, the pathological changes in the spinal cord were aggravated; the majority of neurons in the spinal cord gray matter showed evident necrosis, vacuolization, and neuronal degeneration, accompanied by the proliferation of glial cells and the infiltration of inflammatory cells (Figure 1D).
Next, we detected the histopathological changes of spinal cord tissues upon pretreatment with Astragalus injection. Compared to the I/R group (32I/12hR), degeneration, glial hyperplasia, and neutrophil infiltration were not noticeable in the spinal cord of the Ast group after 12h of reperfusion (Figure 1E). Following a 24-h reperfusion period, the pathological changes in the spinal cord of the Ast group were less severe compared to those in the I/R group at the same time point. The neuronal structure was relativity regular, the nuclei were visible, and the vacuolization was relatively smaller, without obvious hemorrhage (Figure 1F). After reperfusion for 48h, the structure of the gray matter was slightly disturbed, most of the neuronal cells were shrunken, and a relatively larger number of normal-shaped neurons were observed, compared to the I/R group (Figure 1G).
Serum NSE concentrations
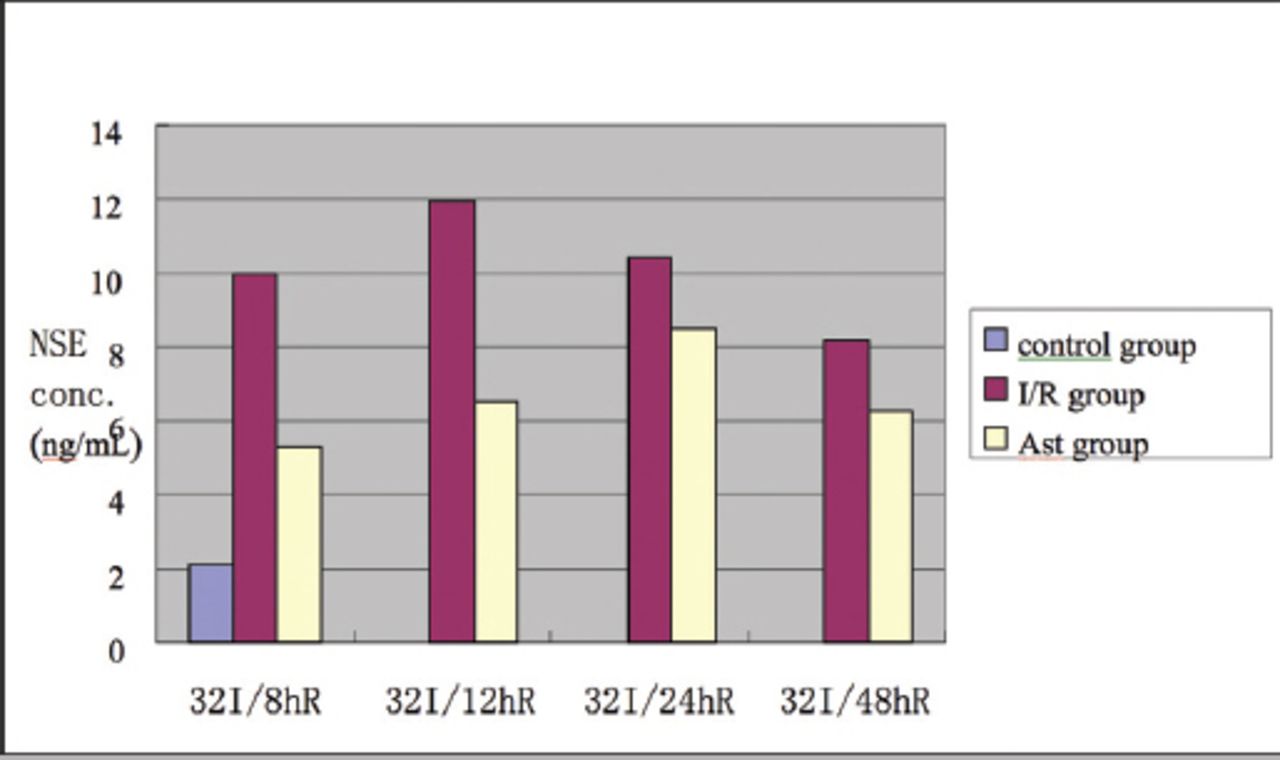
Next, we used ELISA to detect the NSE concentration in the rat serum among the different I/R groups. The serum NSE concentrations of the I/R and the Ast groups were significantly higher than that of the control group at each time point (p<0.01; Table 1, Figure 2). At all reperfusion time points (8h, 12h, 24h, and 48h), the serum NSE concentrations of the Ast groups were significantly lower than those of the I/R groups (p<0.01). The highest NSE concentration was observed in the I/R group at 12h following I/R injury. Whereas, the highest NSE concentration in the Ast group was observed at 24h following I/R injury. Compared with the I/R group, the NSE concentration in the Ast group after I/R was lower and had less fluctuation.

Serum neuron-specific enolase (NSE) concentrations among the different groups.
Serum neuron-specific enolase (NSE) concentrations (ng/mL)
Assessment of AQP4 level
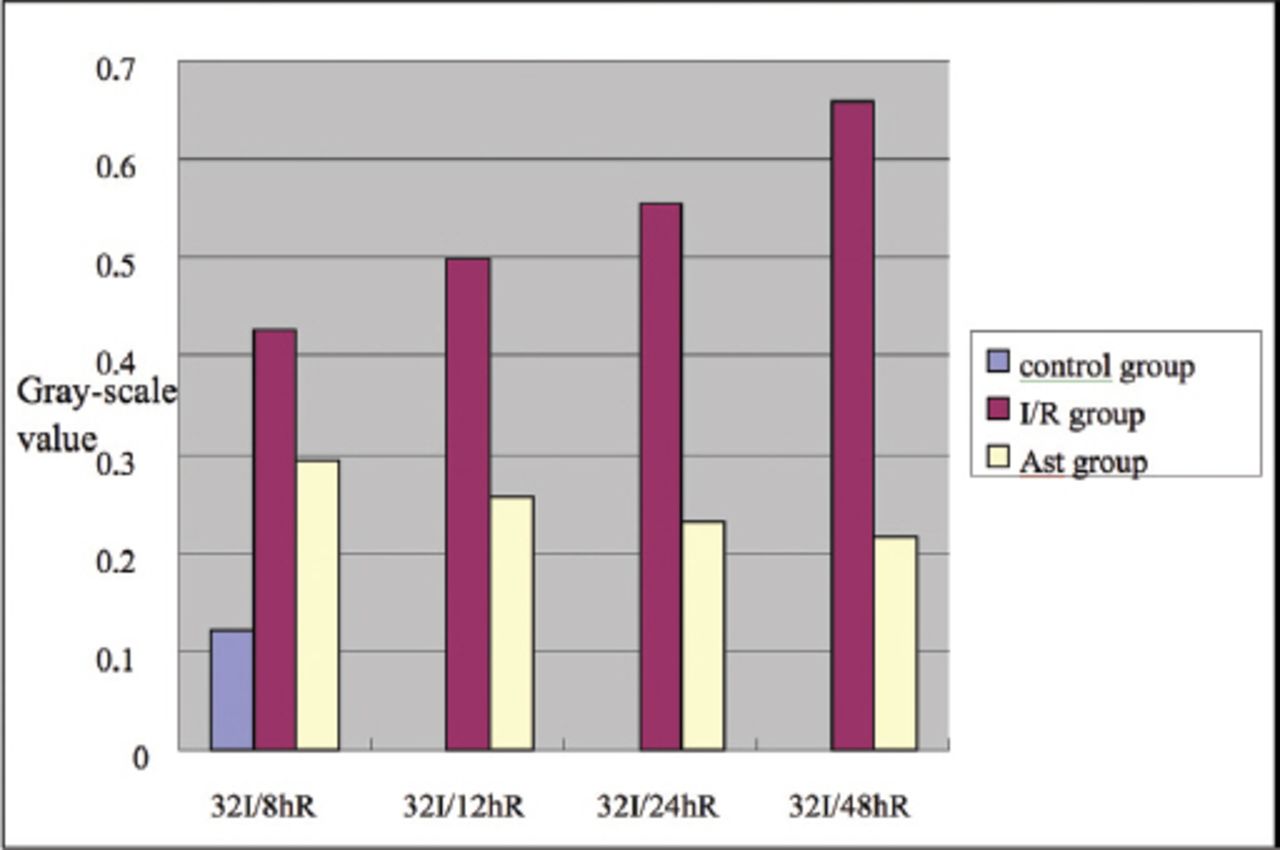
We investigated the expression level of AQP4 in the spinal cord by western blotting. The differences among the I/R groups, Ast groups, and control group were significant (F=10.482, p<0.01; Table 2, Figure 3). The expression levels of AQP4 in the spinal cord tissue in the I/R groups and the Ast groups were significantly higher than that of the control group. At 8, 12, and 24h, the difference in the AQP4 level was significantly higher in the I/R group than in the Ast group (t8h=2.86, t12h=3.611, t24h=4.72, p<0.05). However, the AQP4 level was not significantly different between the I/R and Ast groups at 48h (t=2.513, p>0.05). Among the I/R groups, the AQP4 level gradually increased between 8 and 48h after I/R, reaching its peak at 48h, while, among the AST groups, the expression of AQP4 was highest at 8h after I/R.
Aquaporin-4 (AQP-4) gray-scale values.

Aquaporin-4 (AQP-4) protein levels among the different groups.
Discussion
Astragalus injection has been used in traditional Chinese medicine as a general tonic and for the treatment of various pathological conditions.17 In this study, we examined the neuroprotective function of Astragalus injection in a model of spinal cord ischemia in rats. We observed that Astragalus pretreatment significantly improved the histological features of the spinal cord, decreased the serum concentration of NSE, and downregulated the AQP4 expression in a spinal cord I/R model.
Neuron-specific enolase is a cytoplasmic enzyme specific to neurons and neuroendocrine cells.18 Under normal physiological conditions, the serum NSE concentration is extremely low owing to its relatively large molecular weight and, hence, its inability to penetrate the blood-brain barrier and the cerebrospinal fluid-brain barrier. Elevated serum NSE levels reflect neural necrosis and damage to the blood-brain barrier or cerebrospinal fluid-brain barrier.19,20 Following spinal cord I/R, neuronal necrosis and disintegration are induced by ischemia, hypoxia, and other post-reperfusion effects, leading to elevation of the NSE concentration in the serum. Previous research has demonstrated that following spinal cord I/R, the permeability of the spinal cord barrier begins to increase within 2-6h and continues to do so in the next 12-48h.21,22 Within the first 48h after I/R injury, the neural and glial cells are necrotic and NES seeps into the blood, thereby augmenting the serum NSE level. In this study, our results showed that the serum NSE concentration peaked during the first 12-24h after spinal cord I/R, followed by a tendency towards a gradual reduction during the 24-48-h window. Therefore, it is plausible to speculate that neuronal necrosis and disintegration peaked during the first 12 to 24h. Next, owing to the recovery of the spinal cord blood supply and the elimination mechanism of harmful factors (namely, ischemia and hypoxia), neuronal necrosis and disintegration gradually decreased after the 24-h reperfusion, accompanied with a subsequent slow decrease of the NSE serum concentration. The NSE serum level peaked at 12h after I/R in the I/R groups, while the serum NSE level peaked at 24h following I/R in the Ast groups. Moreover, the serum NSE values were significantly lower in the AST groups than those of the I/R groups. Additionally, it has been proposed that an increase of the serum NSE level in the early stage of spinal cord I/R is closely correlated to the degree of neuronal damage in the spinal cord.23 Taken together, these results support the neuroprotective effect of Astragalus injection on neural cells in spinal cord I/R injury.
Fluid equilibrium is crucial for maintaining homeostasis in a living organism. In the early 1980s, Agre et al identified AQP in erythrocyte membranes.24 Later, 13 types of AQP were discovered in different tissues of numerous animals. Aquaporin monomers, usually about 26-34 kD per unit, are located on the cell membrane and mediate the transmembrane transportation of water molecules. Some AQPs also can transport small nonpolar molecules, including glycerol and urea.25 The aquaporin-4 is widely distributed in the central nervous system, especially in astrocytes. It plays an important role in maintaining homeostasis of the central nervous system and the blood-brain barrier.26 Furthermore, AQP4 plays a significant role in the development of edema following central nervous system injury.27 Following spinal cord injury, alteration of AQP4 expression has been correlated to changes in the water content of the spinal cord and, hence, the development of spinal cord edema.28 Indeed, in the present study, we observed that the AQP4 expression in the I/R groups gradually increased during the first 8-48h following spinal cord I/R injury. In addition, AQP4 expression was significantly higher in the I/R groups compared to the control group. These results indicate that the expression of AQP4 can promote the formation of spinal cord edema in the early phase of spinal cord I/R injury. Similarly, it has been demonstrated previously that an elevated expression of AQP4 in the acute phase of spinal cord I/R injury is accompanied by aggravation of spinal cord edema.29 Pretreatment with Astragalus injection successfully downregulated the expression of AQP4 at 12, 24, and 48h following reperfusion, and the AQP4 expression in the Ast groups was significantly lower than that of the I/R groups at each time point. Secondary edema that follows spinal cord I/R injury aggravates ischemia and hypoxia in the spinal cord lesion. Therefore, treatment of spinal cord I/R injury can reduce edema of the spinal cord lesion and alleviate secondary effects.
In conclusion, the results of the present study suggest that Astragalus injection can alleviate edema and mitigate secondary pathological damage of spinal cord tissue by downregulating AQP4 expression. Nevertheless, this study had a few limitations, including the relatively small number of animals, the lack of behavioral assessment, and the absence of sufficient evidence to elucidate the exact molecular mechanism. Future studies are required to elucidate the underlying molecular mechanism and the impact of Astragalus on the AQP4 pathway. Additionally, we need to determine the optimal dose of Astragalus injection to achieve the maximal therapeutic effect.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received August 17, 2017.
- Accepted January 24, 2018.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.