


Abstract
Objectives: To investigate whether sleep spindles asynchrony (SSA) using scalp sleep electroencephalogram (EEG) among children below 2 years of age can predict future handedness.
Methods: This is a retrospective study conducted from October 2016 until June 2017 at the King Fahad Medical City (KFMC), Riyadh, Kingdom of Saudi Arabia. We retrospectively reviewed 300 EEGs recorded at our neurophysiology laboratory.We included EEGs performed during sleep for infants aged 2 months to 2 years who have already attained their handedness or those aged above 2 years. We excluded records of children younger than 2 months or above 2 years of age (at the time of the EEG) or those aged below 2 years (at the time of the interview), and severely abnormal tracings and those without sleep or enough SSA .
Results: The lateralization of Sleep Spindles (SS) was mostly right-hemispheric (52%) compared to left-hemispheric (36.4%). The overall SS laterality did not correlate with handedness (p=0.81). In the majority of right-handed (64%) and left-handed (60%) children, the SSA was contralateral to the side of hand preference; however, it did not correlate statistically (p=0.377).
Conclusion: We were unable to prove a statistically significant correlation between SSA and future hand preference. Further research involving larger cohorts is still needed.
Sleep architecture is an essential part of evaluating any electroencephalogram (EEG). Despite being recognized and described as early as the discovery of EEG, sleep features remain understudied. In most children, Sleep Spindles (SS) do not synchronize over the 2 hemispheres until the child develops Handedness, usually at 2 years of age. This coincidence of the establishment of Handedness and synchrony of SS makes the connection between the 2 maturational developments important. We planned to investigate the possibility of anticipating future hemispheric dominance and future Handedness using the concept of Sleep Spindles Asynchrony (SSA). The SS consist of bilaterally symmetric low to medium voltage bicentral synchronous rhythmic spindle-like waves, with frequency ranging from 12 to 16 Hz, which often appear along K-complexes lasting approximately 2-3 seconds.1 The identification of SS is easy in any sleep EEG due to their abundance in infants and children. Their typical location in adults is a synchronous burst of waves around the vertex; in children, it varies according to age.2⇓⇓⇓⇓–7 It is thought that the origin of sleep spindles is the thalamocortical network. However, there is no functional meaning definitively established for this mechanism so far, which makes our study relevant to this area.3 The SS are not seen in the first 2 months of life and start to appear afterward.8 The absence of sleep spindles during mid-infancy is considered a significant abnormality. However, their independent occurrence (asynchrony) below 2 years of age is common and a normal finding.9⇓⇓–12 These sleep milestones are consistent between subjects, and therefore they are an essential indication of functional maturation.13 Chatburn et al14 found that sleep spindle activity was associated with various aspects of maturation and is an integral part of brain development. It is suggested that sleep EEG may be a marker for intellectual ability.15 Specifically, SS are associated with the intelligence quotient (IQ).16 The SS are also found to be involved in procedural memory.17 There are a few speculations about how Handedness is created in individuals. Although antenatal mechanisms might be essential, analysis considering in utero development verified that Handedness was an extremely accurate indicator of hemispheric dominance after birth.18 Early hand preference does not develop before one-year of age, and the usual age at which Handedness appears is 2 years, coinciding electrographically with SS synchrony, making a causal relationship or mechanism between the 2 markers highly likely.19–20 There is no previously published research to date to have studied this area.21
Methods
This study was retrospectively conducted from October 2016 until June 2017 at King Fahad Medical City (KFMC), National Neuroscience Institute (NNI), Riyadh, Kingdom of Saudi Arabia. The study involved children aged between 2 months and 2 years who did an EEG during 2014 and 2015 that are approved to be reported independently by 2 qualified neurophysiologists.
The inclusion criteria (IC) were: children (males and females) who underwent sleep EEG at or after 2 months to 2 years of age, currently aged above 2 years to ensure Handedness. The EEG inclusion criteria were: EEG records were carried out in a neurophysiology laboratory for 20 minutes or more with achieved sleep tracing according to the standardized electrode placement system, which is the international 10-20 placement system with at least 2 montages (one bipolar montage and one unipolar/referential montage). The SS observed are those localized on frontocentral and centroparietal leads with a frequency of 12-16 Hz lasting for 1-5 seconds. Asynchronous SS were defined as spindles that appeared independently on either hemisphere with a time lag of at least half a second. The exclusion criteria were: patients underwent an EEG study before 2 months or after 2 years of age, current age of the patient was less than 2 years, and patients were deceased at the time of the interview. The EEG exclusion criteria were: grossly abnormal EEGs with abundant epileptiform discharges and electrographic seizures, EEG records acquired without sleep tracing, and in patients aged less than 2 months or more than 2 years. We also excluded EEGs with solely synchronous SS, spindles that do not fulfill the criteria of described SS or very few SSA defined by cut off of less than 10% difference. We then reviewed a total of 300 EEGs in 3 stages: 1) Analysis of the whole tracing, excluding the grossly abnormal EEGs. 2) Exclusion of records that did not meet our IC. During the first two stages, 267 EEGs were excluded. 3) Carefully analyzing the sleep spindles in the remaining 33 recordings by quantifying a total of 1115 recorded spindles, including left-sided asynchronous, right-sided asynchronous, and bilaterally synchronous SS.
The KFMC ethics committee approved the study design and proposal. Informed consent was obtained during the voluntary participation in the study by text message followed by a phone call to confirm the parents’ willingness to participate in the research study. Parents were later contacted again by phone to confirm Handedness. They were also asked about current age and developmental milestones, family, and personal history of Handedness by asking the parents about the daily behaviors of the child, such as eating, drawing, and coloring. In the end, 33 patients met our IC, and their data were tabulated in Excel sheets, and statistical analysis was performed using SPSS 17 (SPSS, Inc., Chicago, Illinois, United States). Categorical data were described as frequency (percent), and the metric data was measured as the mean (standard deviation). The association between sleep spindles and all the independent factors was measured by chi-squared test (χ2) and Kendall’s tau b correlation. All the inferences were drawn at a 95% confidence interval, and Statistical significance was defined as p<0.05.
Results
After reviewing 300 EEG records, 33 EEGs during sleep and wakefulness met our IC in which we analyzed 1115 bursts of synchronous and asynchronous sleep spindles. Of these, 344 (31%) started over the right hemisphere, 411 (36.8%) started over the left hemisphere, and 360 (32.3%) were synchronous. A total of 33 patients met our IC (19; 57.6% females and 14; 42.4% males). Patient characteristics are summarized in Table 1.
Patient characteristics.
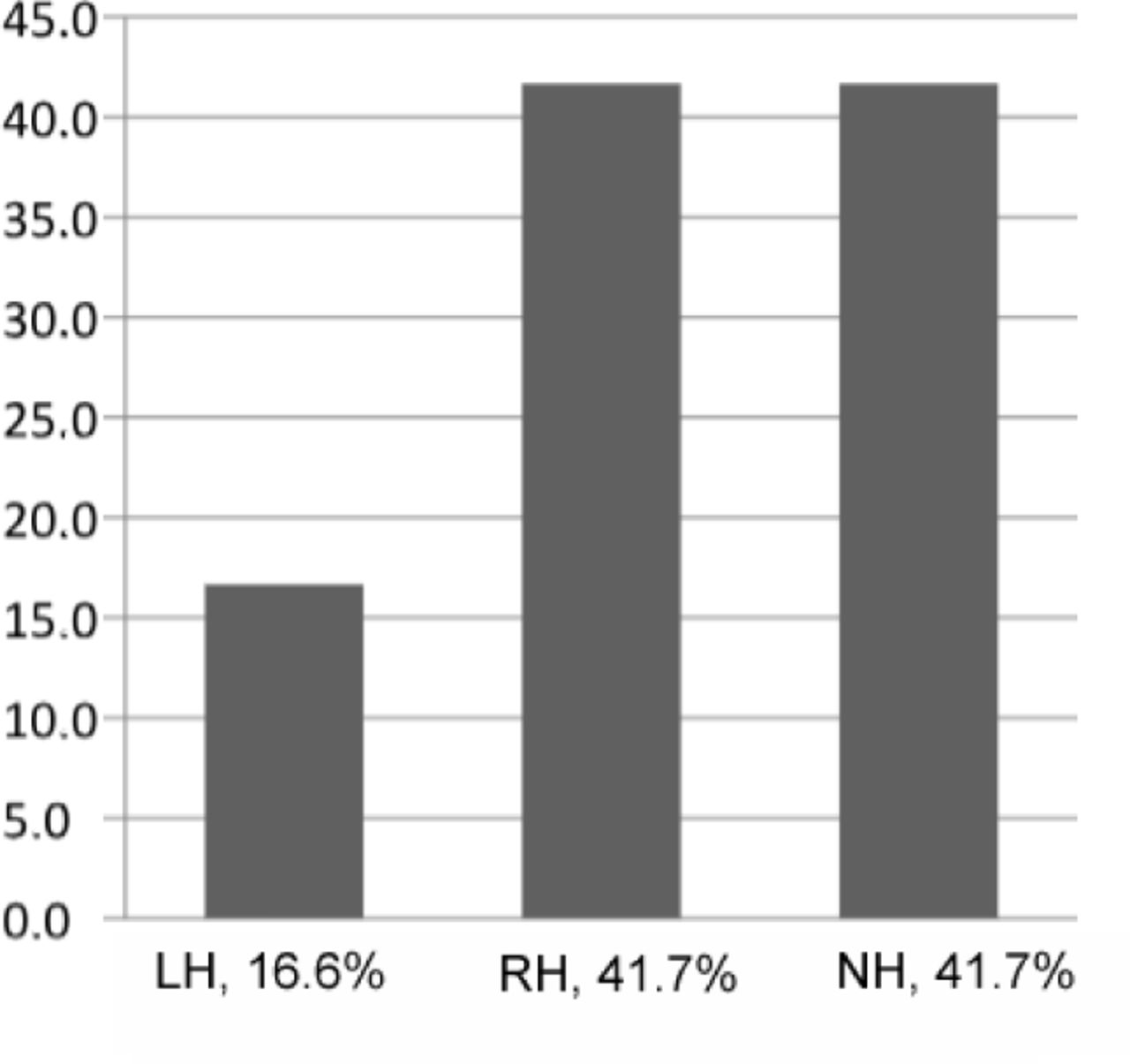
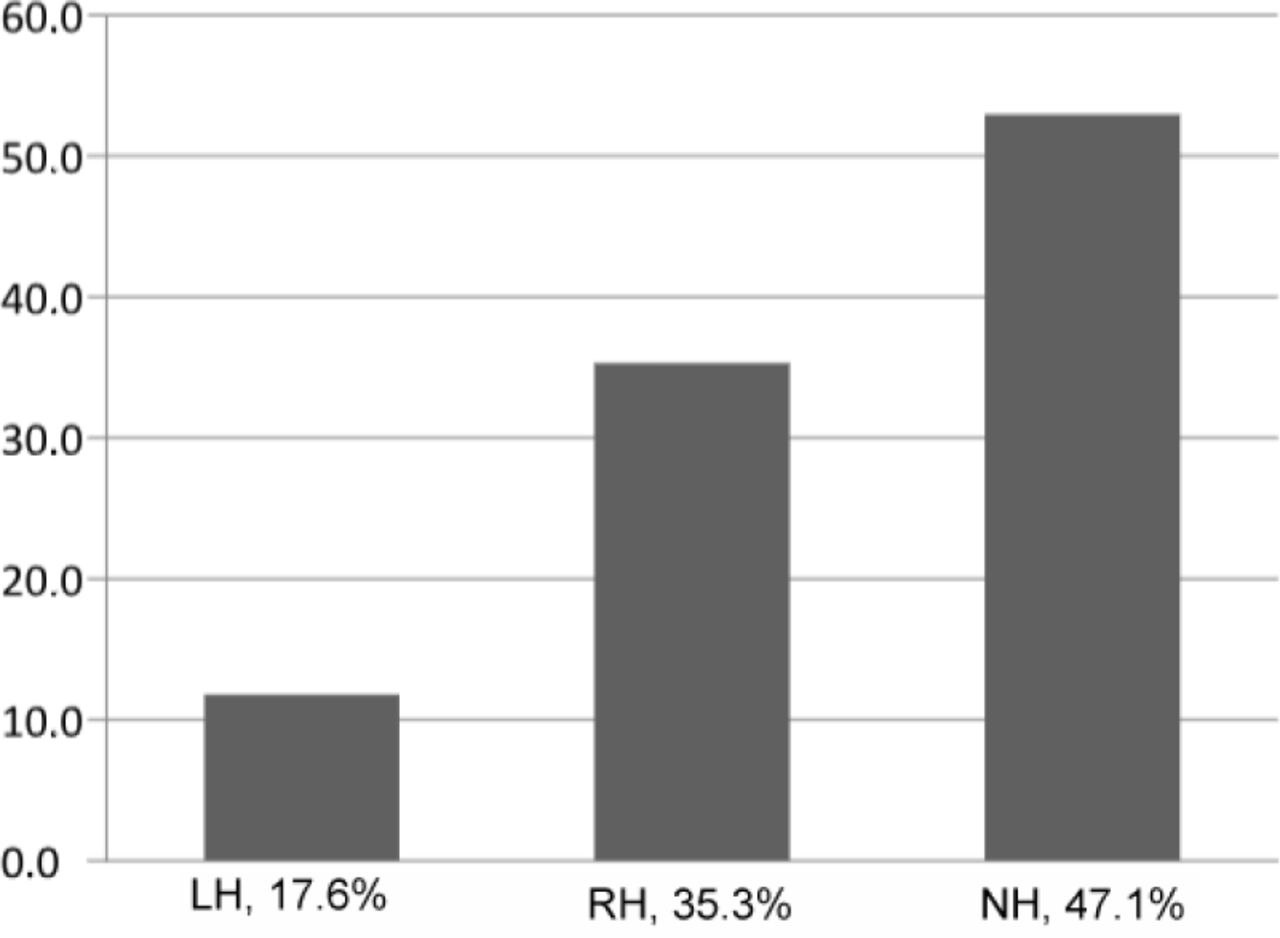
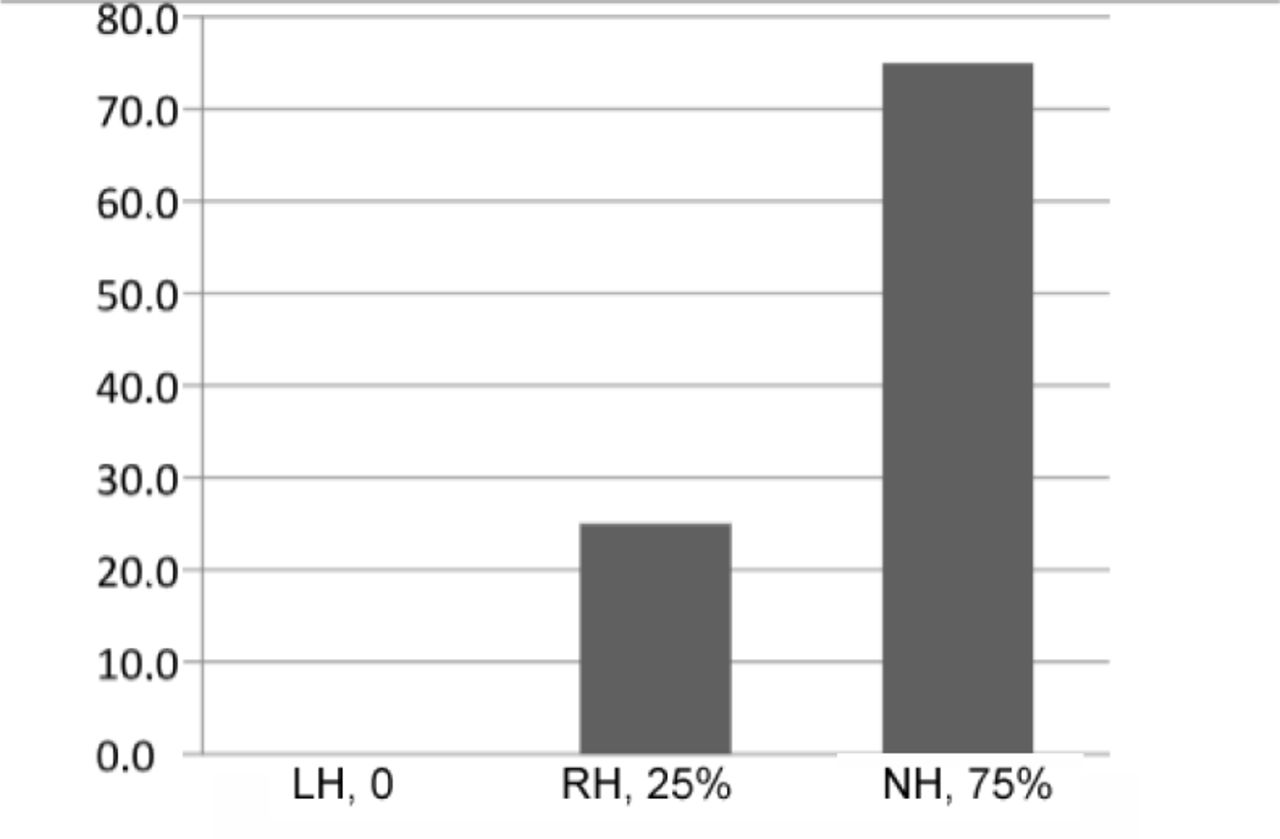
Our findings show that, of 33 patients, 5 (15.2%) were left-handed, 12 (36.4 %) were right-handed, and 16 (48.5%) patients had no preferred handedness. The EEG results showed that: 12 (36.4%) patients had left-sided sleep spindles, 17 (51.5%) patients had right-sided sleep spindles, and 4 (12.1%) patients had inconclusive sleep spindles (Table 1). As for EEG laterality (Table 2), we observed that: A) of 12 patients with predominantly left-sided SS, 5 (41.7%) attained right-handedness, 2 (16.6%) attained left-handedness, and 5 (41.7%) did not attain Handedness (Figure 1). B) of 17 patients with predominantly right-sided SS, 6 (35.3%) attained right-handedness, 3 (17.6%) attained left-handedness, and 8 (47.1%) did not attain Handedness (Figure 2). C) of the remaining 4 patients with inconclusive sleep spindles, 1 (25%) attained right-handedness, none (0%) attained left-handedness, and 3 (75%) had undetermined Handedness (Figure 3). We investigated the Handedness observed across EEG laterality (p=0.377) (Table 2). Out of 33 patients: A) of 5 left-handed patients, 2 (40%) had left-sided SS and 3 (60%) had right-sided SS; B) of 12 right-handed patients, 5 (41.7%) had left-sided SS, 6 (50%) had right-sided SS, and 1 (8.3%) had inconclusive SS; C) of 16 patients who did not develop handedness, 5 (31.3%) had left-sided SS, 8 (50%) had right-sided SS, and the last 3 had inconclusive SS. Excluding the 4 inconclusive patients, further dichotomous analysis of the 29 patients with right-sided or left-sided spindles revealed that, among the 11 right-handed children, the majority (7/11; 64%) had SS predominantly leading from the contralateral left hemisphere, and among the five left-handed children, the majority (3/5;60%) also had SS predominantly leading from the contralateral right hemisphere. Finally, among the remaining 13 children who were not handed, the majority (7/13;53.8%) of the spindles were synchronous (Table 3).
EEG laterality observed across handedness.

Handedness among those with predominantly left-sided sleep spindles. RH - right handed, LH - left handed, NH - Not identified Handedness.

Handedness among those with predominantly right-sided sleep spindles. RH - Right Handed, LH - left handed, NH - Not identified Handedness.

Handedness among those with predominantly inconclusive spindles. RH- Right Handed, LH - Left Handed, NH - Not identified Handedness
Asynchrony observed across handedness.
Discussion
In this study, we hypothesized that SSA might anticipate Handedness during the first 2 years of life as a new readily available clinical tool, considering the daily medical practice and current literature. The purpose of this paper was to find an easy and non-invasive predictor or a biomarker of hemispheric dominance. Handedness was chosen as a clinical sign of cerebral lateralization to help in future decision-making during the evaluation of young children undergoing epilepsy surgical intervention as a pivotal practical implication. Some studies addressed question on spindles in adults whose synchronization of SS has already been achieved.22 Analyzing these results showed that more than half of the left-handed patients had right-sided sleep spindles, and most of the right-handed patients previously had left-sided SS. More than half of our sample had not developed Handedness, which could be attributed to most of the included children being referred to tertiary care centers for developmental delay, seizures, or mental/neurological disability. Our results did not show a statistically significant correlation between SSA and Handedness, thus cannot be a reliable predictor of hemispheric dominance. Other studies found a relationship among gender, age, type of sleep spindle, and their distribution over the cerebral hemisphere, showing that young females are characterized by left-hemispheric dominance in fast sleep spindling and older males are characterized by more pronounced left temporal/orbitofrontal dominance of fast sleep spindling.22 Our study was limited by a few factors, including the small sample size and the fact that patients were mostly neurologically impaired. Some patients were not included in the data analysis due to difficulty reaching the caregiver, death of the patient, or poor EEG recording. All our patients were referred for a tertiary care evaluation; thus, the majority (25/33; 76%) was developmentally impaired. While conducting this study, only the side of SS onset was taken into consideration for asynchrony assessment; we have not used other measurement parameters, including density, frequency, and amplitude. Although a p-value of 0.377 suggests no statistically significant correlation, we hope that our study inspires further work in this area, and we believe that if our sample size was 100 or more children with normal development, it might have shown a more significant conclusion. Future research directions include recruiting many children with normal development who are referred for sleep EEG for either benign seizures or seizure mimickers. Also, additional waveform features other than timing (synchrony), such as amplitude, frequency, and duration should be added to future work.
In conclusion, although a potential significance has been shown by this paper, analyzing sleep spindle asynchrony (SSA) did not yield statistically significant values to predict future Handedness. Further research on larger cohorts is still needed to determine the final implications of clinical practice.
Acknowledgements
The authors would like to thank Mr. Wani TA for statistical analysis. We want to thank Editage for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received December 29, 2019.
- Accepted February 29, 2020.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.