


Abstract
Objectives: To describe the incidence rate, clinical presentation, relevant risk factors, and outcome of hemorrhagic transformation (HT) among ischemic stroke patients.
Methods: This retrospective study analyzed HT in patients with ischemic stroke admitted to King Abdullah Medical City from August 2011 to April 2019. Data were analyzed using SPSS. Patients characteristics, procedures, treatments, and outcomes were reported.
Results: There were 504 ischemic stroke patients. The HT was detected in 38 patients (8%). The median age was 66.5 (54.3 -77.5) years, and 24 (63%) were males. HT was classified as hemorrhagic infarction (HI) in 22 patients (58%) while 16 patients (42%) were parenchymal hematoma (PH). The most common risk factors noted were: hypertension (74%), diabetes mellitus (DM) (66%), hyperlipidemia (63%) and ischemic heart disease (IHD) (61%). Nine patients (23.6%) developed HT after receiving thrombolytic therapy. Only one patient (3%) died of HT patients.
Conclusion: HT accounted for (8%) of all ischemic stroke patients. Old age, DM, hypertension, and hyperlipidemia are frequently encountered with stroke patients who developed HT. Follow up CT brain could be of value and could identify HT early to get better outcomes.
Hemorrhagic transformation (HT) which is a spectrum of hemorrhage related to brain ischemia.1 The HT is a primary complications of acute ischemic stroke (AIS).2 Ischemia makes the cerebral vasculature fragile and more reliable to cause HT after AIS.3⇓–5 HT increases both morbidity and mortality rate in the ischemic stroke patients.2 The HT affects the outcomes with potential severe short- and long-term effects.6 The incidence of HT is between 10–40% and depends on many factors.1,7,8 Most of HT occurs within 2 weeks of an ischemic stroke.5 Previous studies considered old age, hypertension (HTN), diabetes mellitus (DM), large infarct (>2 cm), reperfusion time, lower platelet count and treatment with thrombotic- or anticoagulant-therapies as risk factors.9⇓⇓–12 The most effective treatment for AIS according to previous studies is recombinant tissue plasminogen activator (r-tPA),13 however, it appears to increase the risk of symptomatic or asymptomatic HT.1 Previous studies also suggest that the outcome of HT patients be strongly associated with HT type hemorrhagic infarction (HI) (Petechiae) or parenchymal hematoma (PH) (a space-occupying lesion), PH was a significant predictor of both mortality and neurological deterioration.14 Thus, it is critical to understand HT and its characteristics especially in our population. This retrospective study was designed to describe the incidence rate, clinical presentation, and relevant risk factors of HT among ischemic stroke patients. Identifying such knowledge could improve the outcome and decrease the risk of HT in AIS patients.
Method
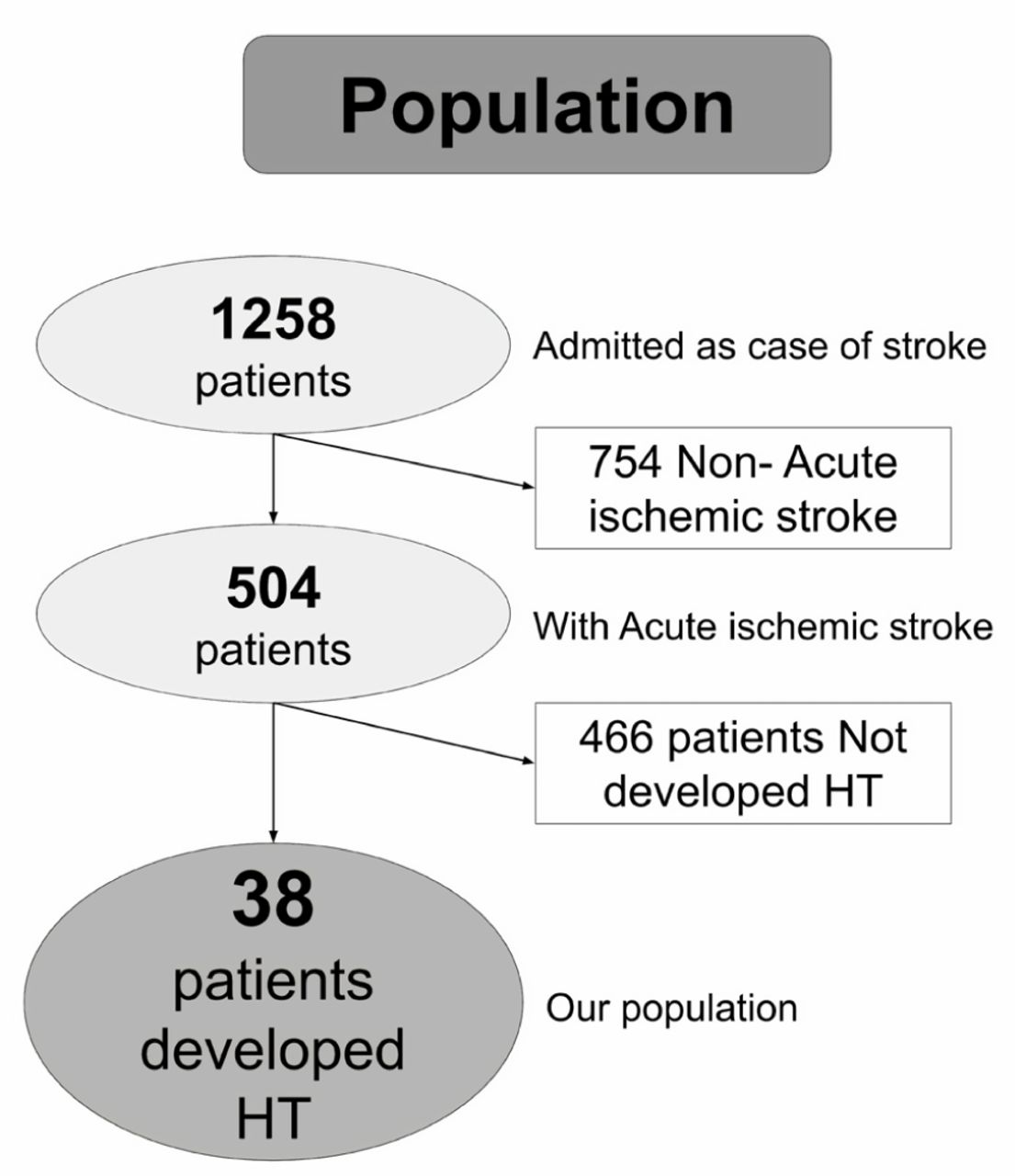
This is a retrospective study conducted in King Abdullah Medical City (KAMC)—a 500-bed hospital in Makkah, Kingdom of Saudi Arabia. We identified all patients admitted to KAMC as a case of ischemic stroke from August 2011 to April 2019. Patients who were diagnosed with conditions other than ischemic stroke and did not develop HT were not considered. All patients did a baseline brain computed tomography (CT) scan within 24 hours from symptoms onset and HT detected in follow-up CT imaging reviewed by a stroke neurologist. The HT was defined as ‘any degree of hyperdensity within the area of low attenuation’.4 The definition of small infarct size (lacunar infarct which is lesion <2 cm).15 We included all the patients who admitted as a case of AIS, and from those we have excluded all the patients who did not developed HT. Of the total ischemic stroke patients, we found 38 patients developed HT (Figure 1). The 38 records were reviewed, and the following data were collected: age, gender, nationality, risk factors, baseline stroke severity scores, laboratory results, radiological reports, vital signs, therapeutic interventions, prescribed medications, complications during hospitalization, stroke severity scores at discharge, length of hospital stay and hospital mortality. The data were collected by 6th-year medical students and supervised by a stroke neurologist.
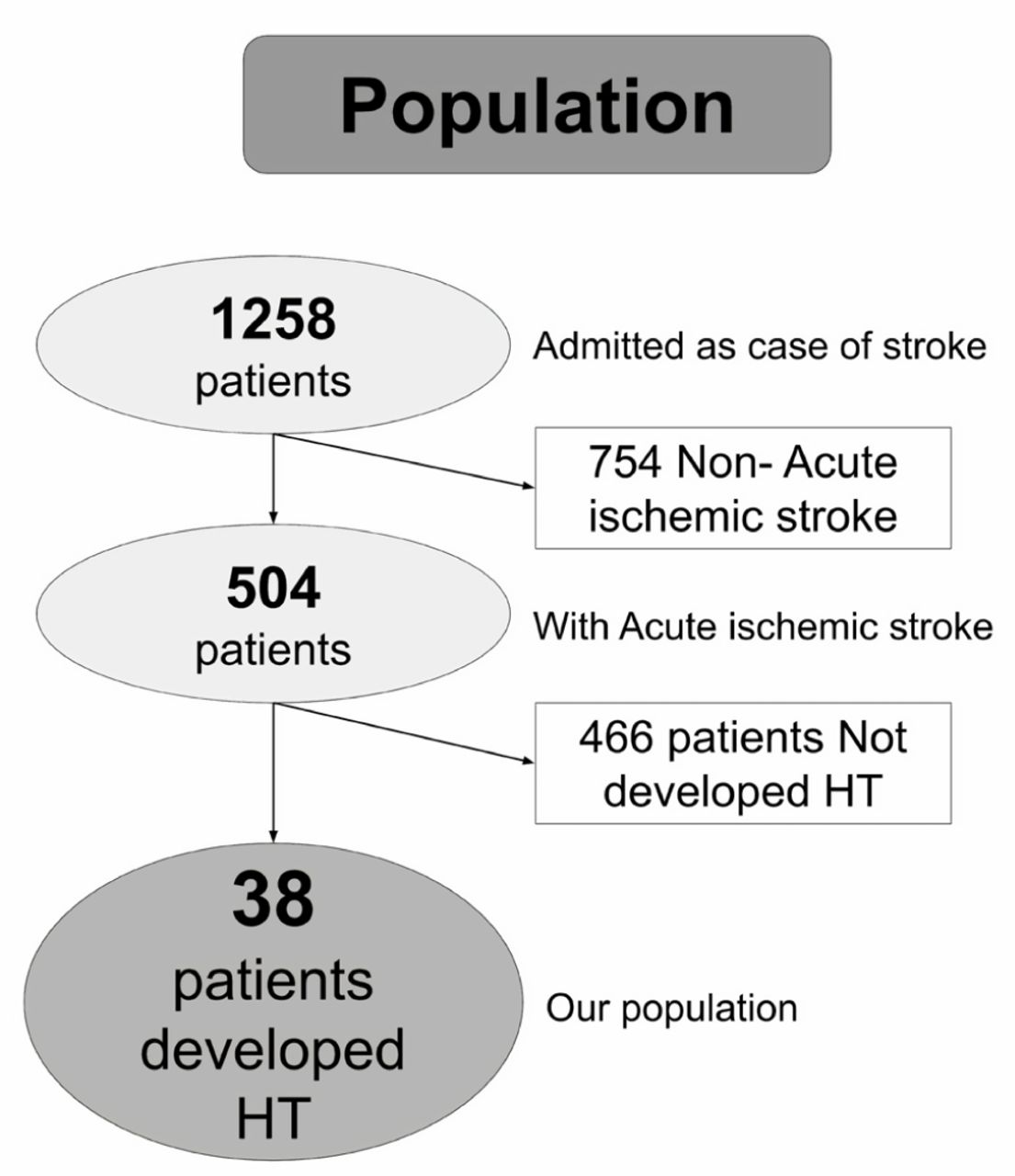
Population.
Data were analyzed using SPSS version 23. Univariable distributions were examined for anomalies, and errors were corrected. Discrete variables were reported using counts and percentages. Continuous variables were examined for normality of distribution visually and by assessing the measure of skewness. Most of the variables were skewed, which indicates that they are not behaving like normal distribution. We also used the Kolmogorov-Smirnov test and Shapiro-Wilk test to test whether the distributions are normal. Almost all the continuous variables have p-values that are well below 0.05. The low p-values imply that there is strong evidence that most of the continuous variables are not perfectly normal. Thus, continuous variables were presented as the median and quartiles. The institutional review board (IRB) of King Abdullah Medical City in Makkah approved the study.
Results
A total of 504 ischemic stroke patients admitted to the hospital during the research period. HT was detected in 38 patients accounting for 8% of all ischemic stroke patients. Patients who developed HT median 66.5 (54.3–77.5) years of age and 24 (63%) were male. The median National Institutes of Health Stroke Scale (NIHSS) at admission was 10 (5.0–14.2), and the median Glasgow coma scale (GCS) was 14.5 (13.0–15.0). Hypertension (73.7%), DM (65.8%), hyperlipidemia (63.2%), and atrial fibrillation (A-Fib) (36.8%) were the most frequent comorbidities. The other comorbidities are listed in (Table 1). The most commonly used medications were antiplatelets (50%), antihypertensive (86.4%), and hypoglycemic agents (42.1%). Regarding stroke etiology, 21 patients (55.3%) were cardioembolic (Table 1).
Demographics and baseline characteristics of patients with HT.
Vital signs and lab findings of patients with HT at admission.
A small infarct size (<2 cm) was found in 5 patients (13.2%) and 33 patients (86.8%) had medium to large (>2 cm). The HI occurred in 22 patients (57.9%), while PH was seen in 16 patients (42.1%). Thirty-one patients (81.5%) had anterior circulation, and 6 patients (15.7%) had posterior circulation. Only one patient (2.6%) had both anterior and posterior (Table 3).
Radiological feature in patients with HT.
Nine patients (23.7%) received tPA, and 6 patients (15.8%) underwent endovascular therapy. Twenty-five patients (65.8%) were admitted to the intensive care unit (ICU). A foley catheter was applied to 18 patients (47.4%), and 5 patients (13.2%) were intubated; 37 patients (97.4%) received antiplatelets, and 34 patients (89.5%) received deep venous thrombosis (DVT) prophylactic. Eleven patients (28.9%) received anticoagulant, and 36 patients (94.7%) received lipid lowering agents (Table 4).
Management parameters and prescribed medications for patients with HT.
Other neurological complications were reported as depression (18.4%) and epileptic seizure (13.2%); DVT developed in 2 patients (5.3%). The median NIHSS score at discharge was 5 (3–10.2). Five patients show 4 points drop in NIHSS score after HT. There were 11 patients (28.9%) who required a hospital stay less than one week, 10 patients (26.3%) were between 8 to 14 days, and 17 patients (44.7%) were more than 2 weeks. Only one patient (2.6%) died during hospitalization and accounted for (2.6%) of the total HT in patients with ischemic stroke (Table 5).
Complications and outcomes data among HT.
Discussion
The HT is one of the major complications of AIS, which can severely affect the outcome. This retrospective study describes the incidence rate, risk factors, clinical presentation, and outcomes of HT in patients with AIS admitted to a tertiary hospital in Kingdom of Saudi Arabia from August 2011 to April 2019. There were 504 patients with AIS: 321 males (63.69%) and 183 females (36.31%). Of those, HT was detected in 38 patients (8%): 24 males (63.2%) and 14 females (36.8%). The incidence of HT is (7.48%) in males and (7.65%) in females in our sample. Studies show the incidence of HT is variable depending on many factors including the study design and inclusion criteria. The incidence of HT after r-tPA is 10–30%.4,12 However, the incidence rate is (15%) in our population. Accordingly, most patients who received r-tPA therapy had a better prognosis compared to patients who did not receive r-tPA therapy.13,16 Some studies consider r-tPA as a risk factor for PH.17,18
We found that HTN (73.7%), DM (65.8%), hyperlipidemia (63.2%), and A-Fib (36.8%) are the most common comorbidities. Several studies reported that DM and HTN are risk factors for HT.16,19 In our study, hyperlipidemia was seen in 24 patients (63.2%). Other studies showed a relation between low LDL level and HT and explained this via the involvement of cholesterol in the integrity of blood vessel; therefore, low cholesterol levels lead to the weak blood vessel and subsequent rupture resulting in hemorrhage.19,20 However other studies showed no association between the level of cholesterol and HT and mentioned that the relation between HT & dyslipidemia remains controversial.
We also found HT was encountered more in our sample with patients who were found to have large infarct size (86.8%). This could be because cardiac embolism is accompanied by large vessel occlusion. This leads to a large infarct size which considered to be a risk for HT.19,21 In our study, half of the HT patients (47.4%) were on dual antiplatelet therapy. We cannot determine if such treatment is a risk factor or not. In a match study which took 18 months, they found that patients with ischemic stroke who had both clopidogrel (Plavix) and aspirin together had an insignificant decrease in major vascular events, while they were found to have an increasing risk of life threatening events, and major bleeding.22
There are some limitations of our study: First, our study conducted in one center so our population may not be representative in large scale. Second, our sample is small, so it is hard to come to conclusion about the clinically significant of different variables. Thus, further large sample size, prospective studies of HT will provide more significant clinical information. Future research idea to take the HT patients and compare them with the non-HT patients across all the different variables.
In conclusion, old age, DM, hypertension, and hyperlipidemia are frequently encountered with stroke patients who developed HT. The HT was detected in 38 patients accounting for 8% of all AIS patients. Follow-up brain CT could be of value even if the patient is asymptomatic to identify the HT early to get a better outcome.
Acknowledgement
The authors would like to thank (www.americanmanuscripteditors.com) for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 26, 2020.
- Accepted June 10, 2020.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.