


Abstract
Tremor is the most common and frequently reported movement disorder in multiple sclerosis (MS). Paroxysmal dystonia (PD), also known as painful tonic spasm (PTS), is a relatively less common but well-recognized movement disorder in multiple sclerosis (MS). These are characterized by episodic attacks of involuntary flexion, extension movements of body. Such paroxysmal symptoms as an initial presenting feature raise many differential diagnoses and can often be mistaken as epileptic seizures as well as psychogenic events and may sometimes lead to delay in diagnosis as well. Diagnosis is clinical with the help of supportive investigations to rule out other paroxysmal disorders, especially epileptic seizures. We describe a case of a young lady, who was referred to us as a case of refractory seizure and diagnosed as having paroxysmal dystonia as a first manifestation of MS, with complete resolution of her symptoms after successful treatment with anti-epileptic drugs.
Paroxysmal dystonia (PD), also called Painful tonic spasm (PTS), is a well-recognized and the most frequently observed movement disorder in multiple sclerosis.1 The PD is classified as 4 types according to the precipitating factors, phenomenology, duration of attacks, and etiology. Paroxysmal kinesigenic dyskinesia (PKD) is induced by sudden movement, paroxys¬mal non-kinesigenic dyskinesia occurs spontaneously, paroxysmal exertion-induced dyskinesia appears after prolonged exercise, and paroxysmal hypnogenic dyskinesia occurs during sleep.2 These disorders have often been misdiagnosed as partial onset epilepsy initially and later identified as movement disorder secondary to MS. Treatment of underlying disease along with symptomatic treatment may alleviate the symptoms significantly. We described a case of a young lady who was referred to us as a case of psychogenic non-epileptic events. Diagnosis of MS manifesting with PD was established. She was started on disease modifying therapy for MS as well as Carbamazepine for her PD. She showed a remarkable improvement on these treatments and was followed up in MS clinic with no new MS relapse or recurrence of PD for 18 months after the initial presentation.
Case Report
A 31-year-old girl with no known comorbidities and insignificant family history presented with recurrent, sudden, painful, stereotyped episodes of movements affecting left upper and lower extremities leading to tonic posturing lasting between 15-30 seconds. There was no change in level of consciousness, hallucination, sphincter incontinence or post ictal manifestations reported by patient. The usual frequency was 15-20 times a day, shown in Table 1. These attacks occurred during the sudden change in position or movement as well as by emotional stress. She was able to predict the attacks and was able to trigger them by specific movements of her arm and leg. On close inquiry patient admitted to having left-side weakness and numbness about one year ago without residual sequel, as well as left eye blurring of vision about three months ago. No consultations and investigations were carried out for these complaints and these subsided over a short span of time.
Timeline of relevant past medical history and interventions.
Clinical findings
Current physical examination was remarkable only for mildly reduced power (4+/5) and hyperreflexia in left upper and lower limbs. Rest of examination was unremarkable.
Diagnostic assessments
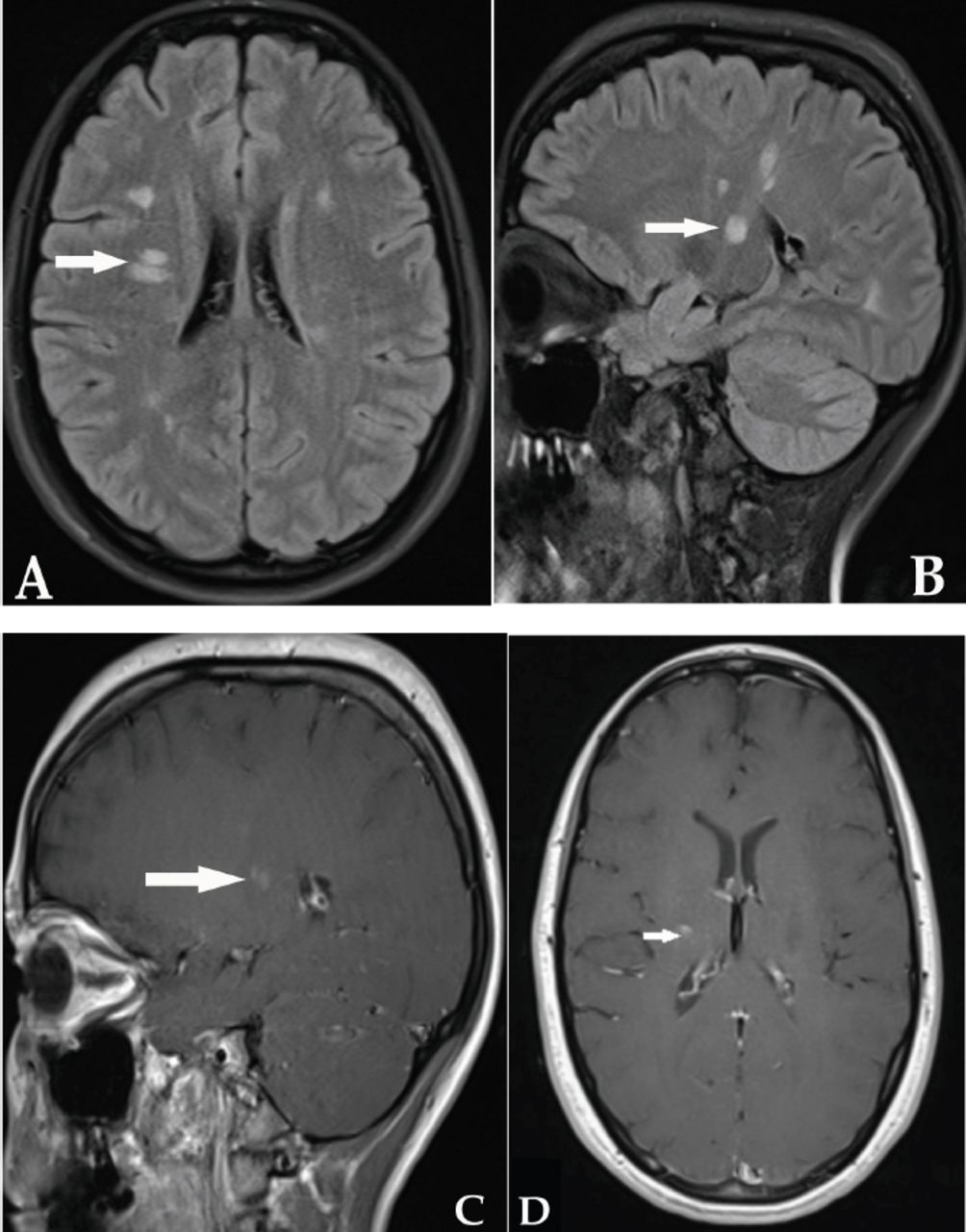
Magnetic resonance imaging (MRI) of brain showed multiple foci of high signal intensity in T2/FLAIR weighted image along periventricular and juxta cortical region of both cerebral hemispheres, with pathological enhancement in one lesion representing interval disease activity, shown in Figure 1 & Table 1. Only the right subcortical white matter area (corona radiate) showed gadolinium enhancement and it was the possible causative lesion for this presentation. Cerebrospinal fluid analysis showed mildly elevated protein (62.8 g/L), slightly high white blood cell count (21), with predominant lymphocytes and normal glucose. Oligo clonal bands were not detected. Paraneoplastic panel and anti-aquaporin 4 antibodies were also negative. No electrographic abnormalities were found in Electroencephalograms (EEG). Complete routine and immunologic investigations and serological tests including HIV, thyroid function tests, vitamin B12 level, ESR and vasculitis workup were normal. The diagnosis of MS was made based on McDonald’s (2017) diagnostic criteria.3

Axial FLAIR shows A) hyperintense subcortical lesions, some of them are perpendicular and periventricular. B) Sagittal FLAIR image shows hyperintense subcortical lesions. C & D) T1 weighted images axial and sagittal showing post gadolinium enhancement of right subcortical lesion at corona radiata.
Therapeutic intervention
A five-day course of methylprednisolone was given to her. She was started on Carbamazepine 200 mg twice daily
Followup and outcomes
Her spasms reduced to one per day in less than 24 hours and disappeared completely the very next day. She also received 5 days’ pulse therapy with intravenous methyl prednisolone (1g/day). Patient was given follow-up in multiple sclerosis clinic for further management.
Discussion
The MS is an autoimmune inflammatory demyelinating disease of the central nervous system characterized by multiple areas of focal demyelination and scarring. The clinical diagnosis of MS requires dissemination of lesions in space and time. Typically MS has a relapsing, remitting course presenting with ataxia, hemiplegia, optic neuritis or brainstem syndromes. Movement disorders are traditionally thought to be rare in MS but recently there is more recognition of these paroxysmal disorders presenting as first episode of MS.4,5 Their prevalence is reported less than 2% in the literature.2 Recognition of paroxysmal phenome as an initial presentation of MS is of utmost importance as it helps not only in timely diagnosis of the primary disease but long term management with DMDs to avoid permanent brain damage as well.
Although not common, sometimes mild weakness and other symptoms of clinical relapse without residual deficit and fast recovery can be ignored by the patient, and these paroxysmal disorders may urge them to seek medical advice, as happened in our case. Tremor is the most frequently reported movement disorder in MS.5 Paroxysmal dystonia, also called PTS, are the second most frequently reported movement disorder in MS. Diagnosis of PD is clinical, along with EEG rule-out of the epileptic nature of these attacks. There are several other stereotyped paroxysmal phenomenon are reported in association with MS, such as trigeminal neuralgia, paroxysmal dysarthria, itching, paroxysmal dysarthria, hemiataxia, akinesia and paresthesia.2 Although difficult to correlate anatomically, PTS are described as resulting from acute demyelinating plaques in various regions of the brain and spinal cord, posterior limb of internal capsule, contralateral cerebral peduncle, centrum semiovale, thalamus and subthalamus.5 Most of the literature showed association of PD with spinal cord lesions.4 The presumed lesion responsible for this acute presentation of PD in our patient is the only enhancing lesion in right hemisphere located at corona radiata. An ephaptic axonal activation at a non-synaptic contact site within a partial demyelinated plaque at any level in motor pathway is considered the most likely pathophysiological explanation for PD.1 Antiepileptic drugs are found to be effective in treating the PD associated with MS. The most common and effective drug is carbamazepine.6 Our patient showed dramatic response to Carbamazepine as described in the literature as well. The mechanism behind the selective response to Carbamazepine is not well understood. Inhibition of voltage-activated sodium channel along with inhibition of voltage-gated calcium channels may be a likely mechanism for cessation of neuronal excitation by ephaptic activation.6
In conclusion, dystonia is an under-recognized Paroxysmal event during evaluation of MS. The PD can be an initial presentation in patients with multiple sclerosis and may pose a diagnostic challenge to physicians. This paroxysmal disorder is a rare and still under-recognized manifestation of MS with a wide range of differential diagnoses. The disorder responds well to Carbamazepine.
Footnotes
Disclosure. The authors declare no conflicting interests, support or funding from any drug company.
- Received March 19, 2019.
- Accepted April 22, 2019.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.