


Abstract
Strokes are a major cause of disability in systemic lupus erythematosus (SLE). Classical neurological manifestations are rare at onset. The use of thrombolytic therapy improves clinical outcome in eligible stroke patients who present early. Modern imaging modalities augment decision making. This 37-year-old woman presented with an acute stroke with National Institute of Health stroke scale 10. The CT showed a hyperdense middle cerebral artery (MCA) dot sign. The magnetic resonance angiography revealed focal thromboembolic occlusion at the insular MCA segment (M2). Intravenous recombinant tissue plasminogen activator (rtPA) was administered with successful recanalization. The present case was a rare event for rtPA use in acute MCA occlusion with underlying latent lupus. Acute vascular event thrombolysis as the presenting manifestation of autoimmune disease has not previously been encountered on literature review. Stroke pathophysiology in conditions of hypercoagulability is a significant clinical entity where the implication for thrombolytic use requires further studies. An ischemic stroke with underlying connective tissue disease benefits from timely multimodal brain imaging and should be considered for reperfusion.
Strokes have been reported in up to 19% of systemic lupus erythematus (SLE) patients,1 with an age and gender adjusted odds ratio of 1.5. The stroke severity in SLE observed by Mikdahsi1 et al in this prospective cohort study showed a high proportion (77%) associated with a National Institute of Health stroke scale (NIHSS) of more than 6. There is high association between antiphospholipid antibodies (APL) and stroke in SLE. The presence of persistently elevated APL antibodies of different specificities increases the risk of stroke more than a single APL antibody.2 The risk of cardiovascular disease (CVD), which includes myocardial infarction, cerebrovascular disease, and peripheral vascular disease among SLE patients is at least doubled when compared with the general population. Younger patients with SLE have the greatest relative risk of CVD compared with their healthy counterparts, but the absolute risk is higher in older SLE patients.3 After accounting for the increased CVD risk associated with traditional risk factors like diabetes, hypertension, dyslipidemia, family history of coronary heart disease, obesity, sedentary lifestyle, and cigarette smoking, SLE itself or its treatment confers the greatest risk for accelerated atherosclerosis. Stroke subtypes in SLE can vary from large vessel disease with resulting hemiparesis, hemisensory loss, ocular field defects or aphasia caused by cardiogenic embolism, vasculitis, and premature atherosclerosis to transient ischemic attack (TIA) or recurrent small infarcts usually due to associated presence of antiphospholipid antibodies. The key factor for successful thrombolysis in acute ischemic stroke is early intervention, which improves functional outcome and the benefits outweigh the risks for patients who receive intravenous (IV) recombinant tissue plasminogen activator (rtPA) within 4.5 hours of symptom onset. This narrow therapeutic window warrants quick screening for thrombolysis since the benefit decreases with time. Modern imaging techniques have potential to identify both salvageable ischemic brain tissue and the responsible vascular lesion. Various risk factors have been associated with the development of ischemic stroke in SLE, but there is no literature on the use of rtPA in acute ischemic stroke with SLE. We present this case of acute middle cerebral artery (MCA) stroke in a healthy young female where IV rtPA was successfully given with previously undiagnosed SLE and discuss the implications of thrombolysis in stroke patients.
Case Report
A 37-year-old right handed female healthy mother of 4 children presented to our hospital 30 minutes after symptoms onset of speech difficulty and weakness in the right side of the body associated with deviation of the mouth to the left side. She had no current history of seizure, incontinence, fever, vomiting, recent head trauma, illicit drug abuse, or oral contraceptive use. There was no history of transient ischemic attack or syncope. She gave a history of one miscarriage in the first trimester 3 years earlier. She also gave a history of small joints pain and swelling around 11-12 years earlier, which lasted for 4 years and was investigated with no cause found. There was no family history of stroke or clotting disorders. On clinical examination, she was fully alert, and oriented. Pulse 82 per minute and regular, blood pressure 146/72 mm of Hg, saturation 99% on room air. There was no jaundice, edema, lymphadenopathy, joint swelling. Neurological examination revealed Glasgow coma scale 15/15, no dysphasia, there was right upper facial motor weakness, no ocular or bulbar signs. There was hypotonia with grade 1 power in the right upper limb, grade 2 in the right leg with normal power in the left upper and lower limbs. Reflexes were brisk in the right half of body with positive babinski sign. National Institute of Health stroke scale (NIHSS) score at presentation was 10. All peripheral pulses well felt with no carotid bruit. She had her first CT of the brain carried out at 35 minutes from hospital arrival (Figure 1), which showed a small hyperdense dot sign in the M2 segment of the left MCA with no direct sign of ischemic infarct or hemorrhage. She showed signs of improvement to Medical Research Council (MRC) grade 3 power in the right upper and lower limbs. The MRI of brain with diffusion weighted imaging (DWI) and magnetic resonance angiography of the cerebral circulation were carried out to document cerebral infarction (Figure 2). This showed acute infarction of the left lentiform nucleus and corona radiata region with signal attenuation from the M2 segment of the left MCA graded as partial thrombo-embolic occlusion (Figures 3 & 4). After full neuroimaging, a decision for thrombolysis with IV rtPA was taken in view of the MRI evidence of an occluded brain vessel with ischemic stroke. All risks and complications associated with the procedure were explained to the patient and her family, and contraindication screening was carried out. She received 10 mg of IV rtPA as bolus followed by 80 mg as IV infusion at 4 hours from onset of symptoms, and was monitored in the intensive care unit for neurostatus to look for any complications associated with thrombolysis. A repeat CT of brain (Figure 5) the next day showed acute linear infarction at the left lentiform and head of caudate nuclei.
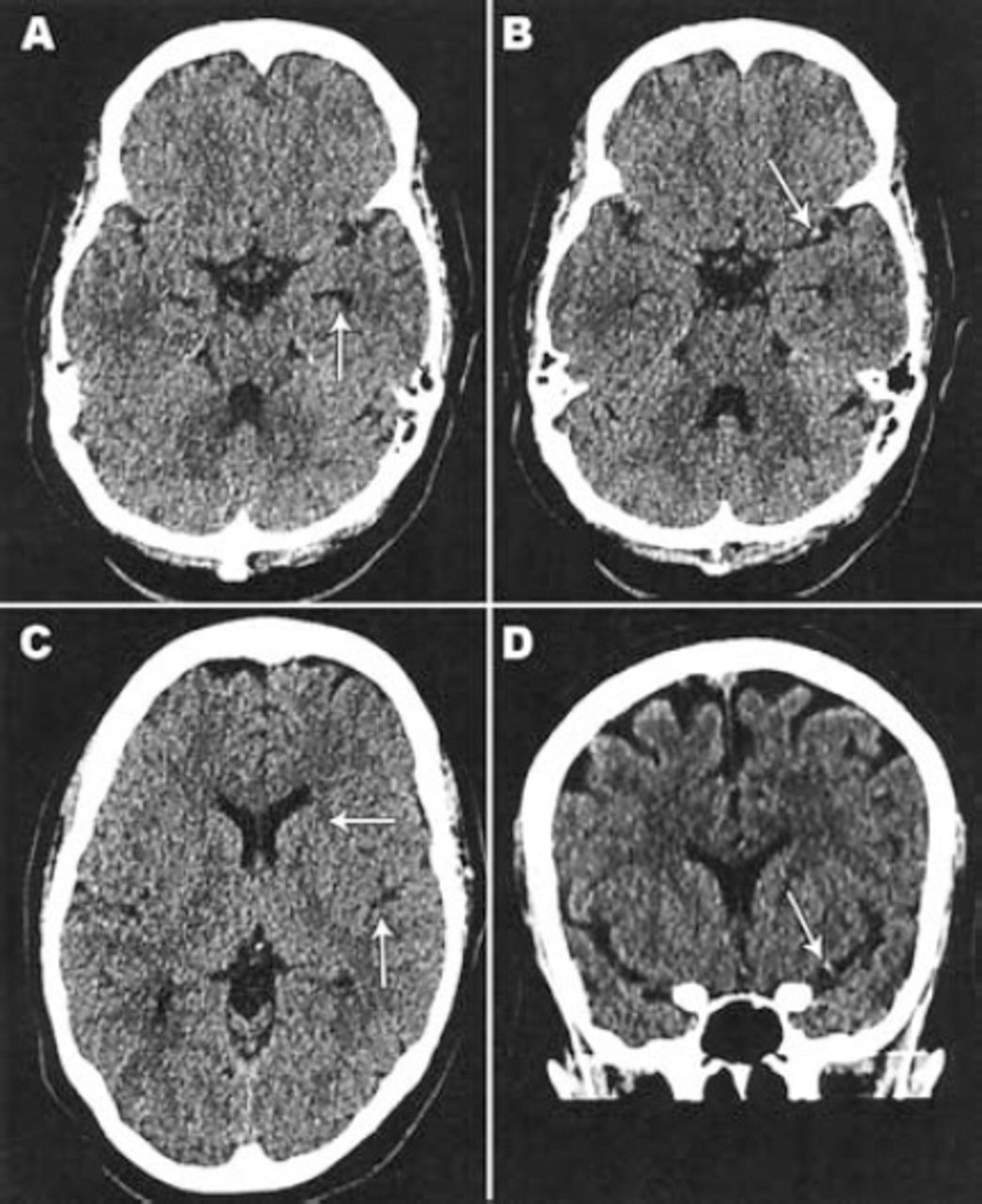
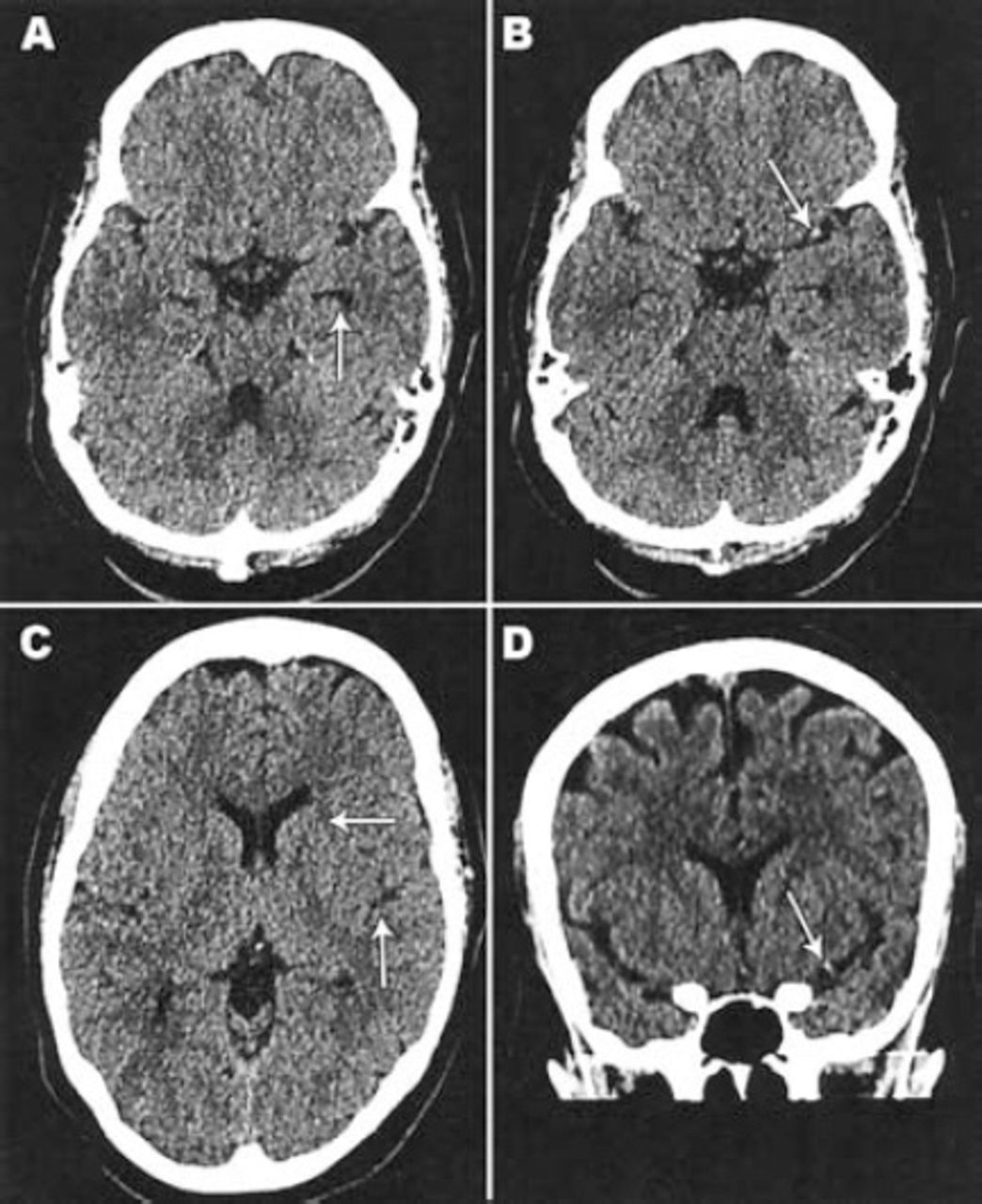
Non-contrast CT scan brain showing A) and C) no CT signs of acute infarction or hemorrhage. B) Axial image and D) Coronal image showing focal hyper-density at the M2 segment of the left middle cerebral artery (MCA dot sign).
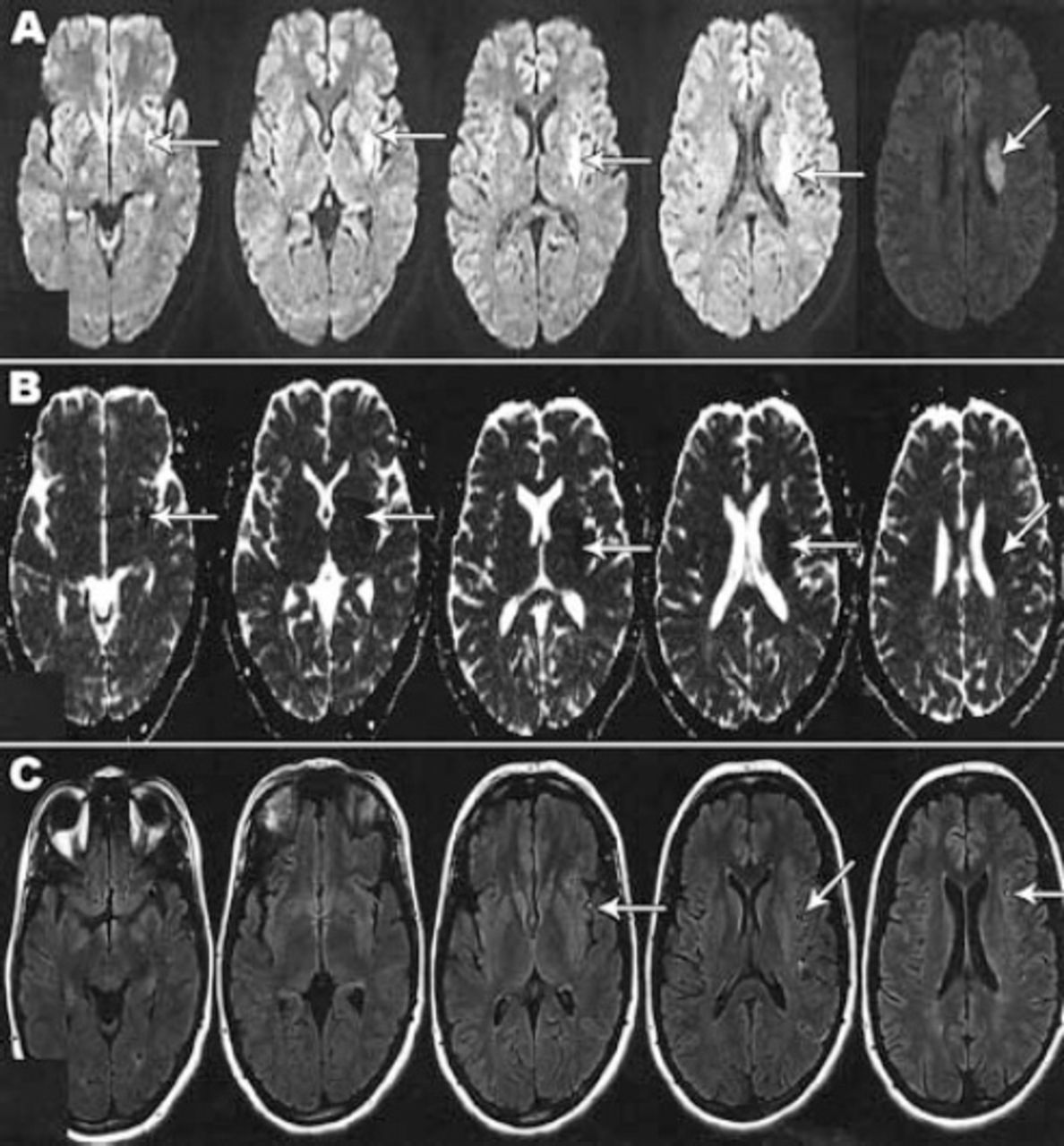
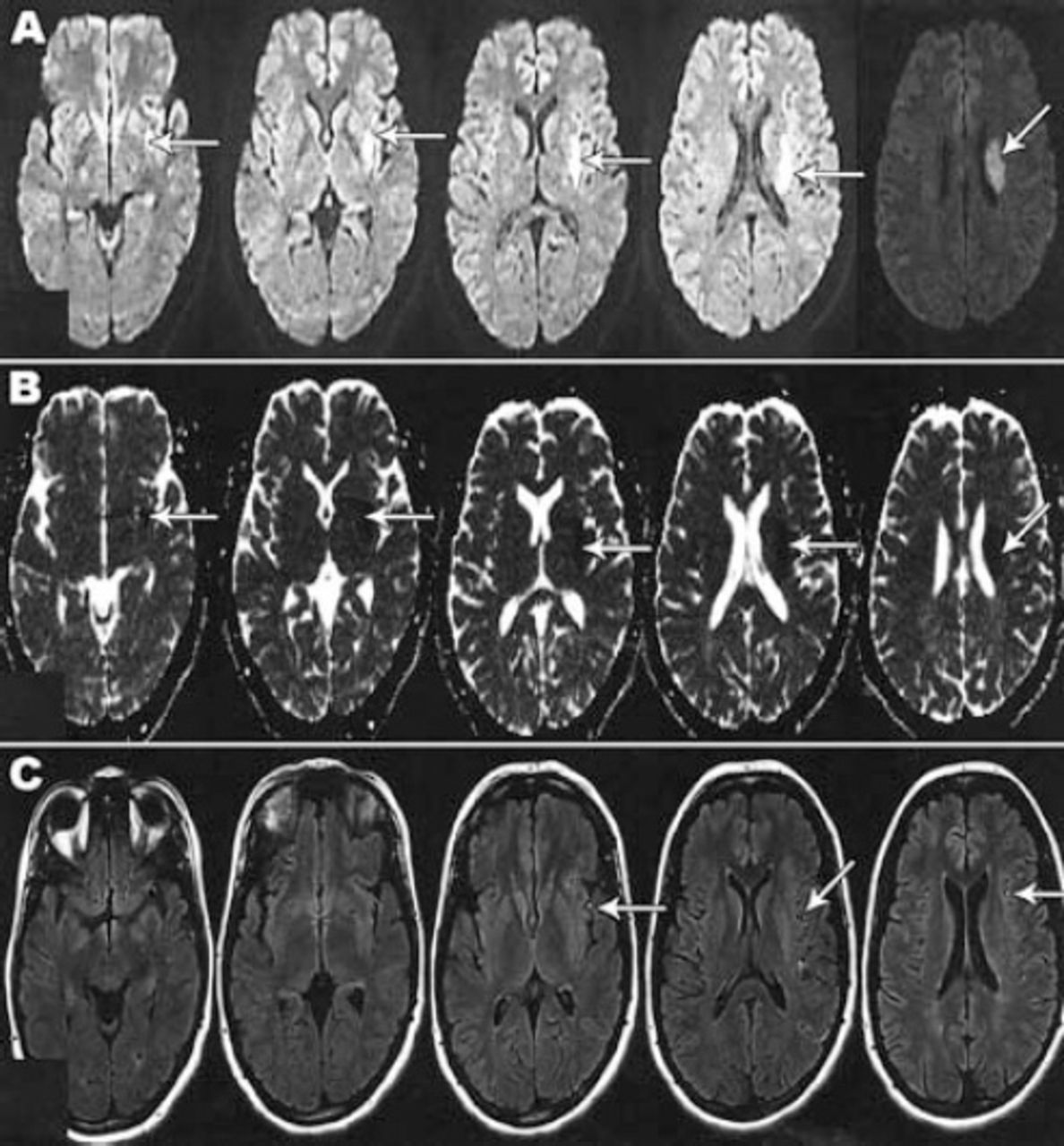
Magnetic resonance imaging with diffusion-weighted image (DWI), apparent diffusion coefficient (ADC) and axial fluid attenuated inversion recovery (FLAIR) WI showing: A) Acute infarction of the left lentiform nucleus and corona radiata region with high signal on DWI (arrow in A); B) Low signal on ADC (arrow in B); C) FLAIR WI with loss of the normal signal void along the M2 and M3 branches of the left middle cerebral artery (arrow in C) implying slow blood flow.
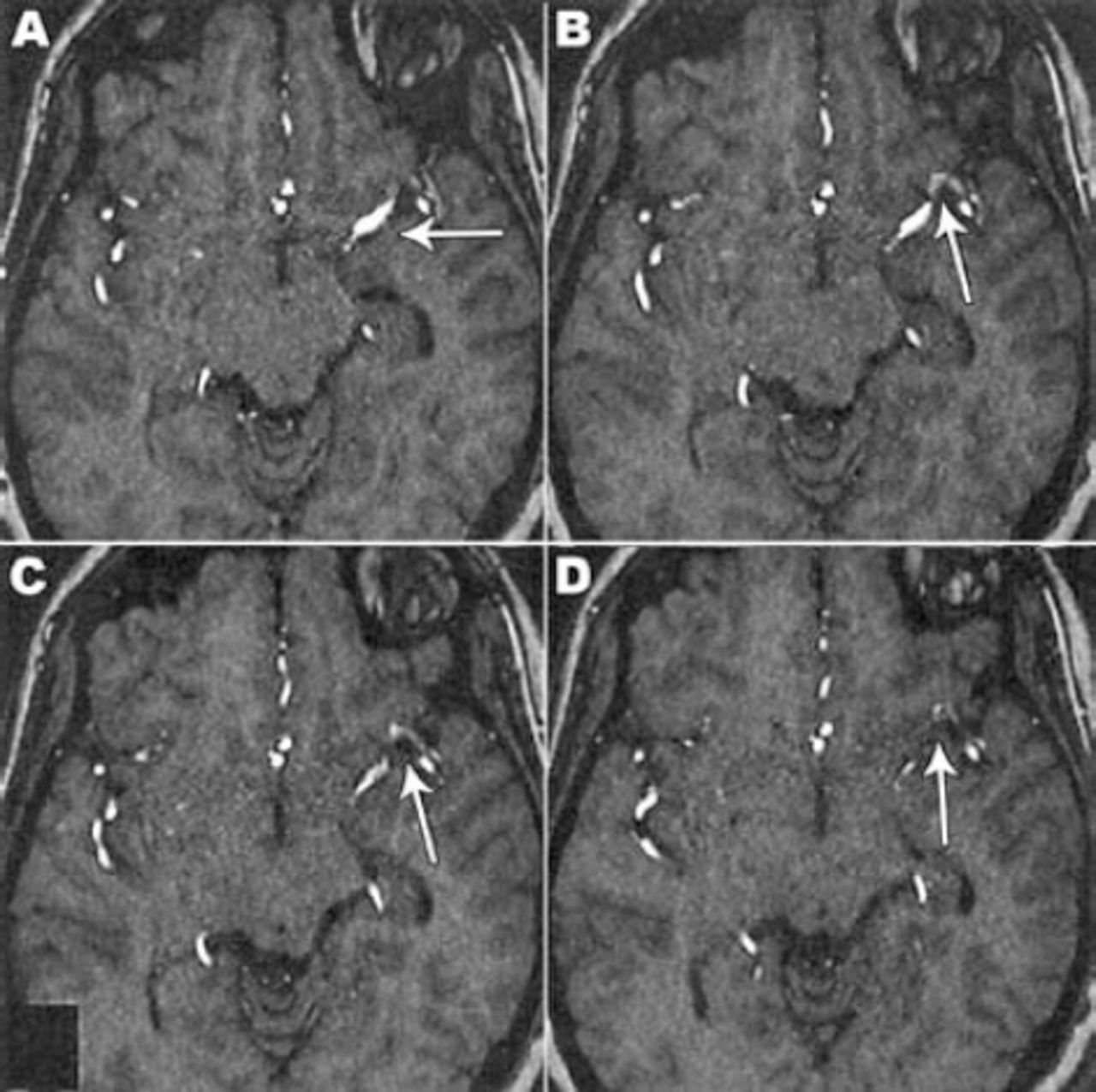
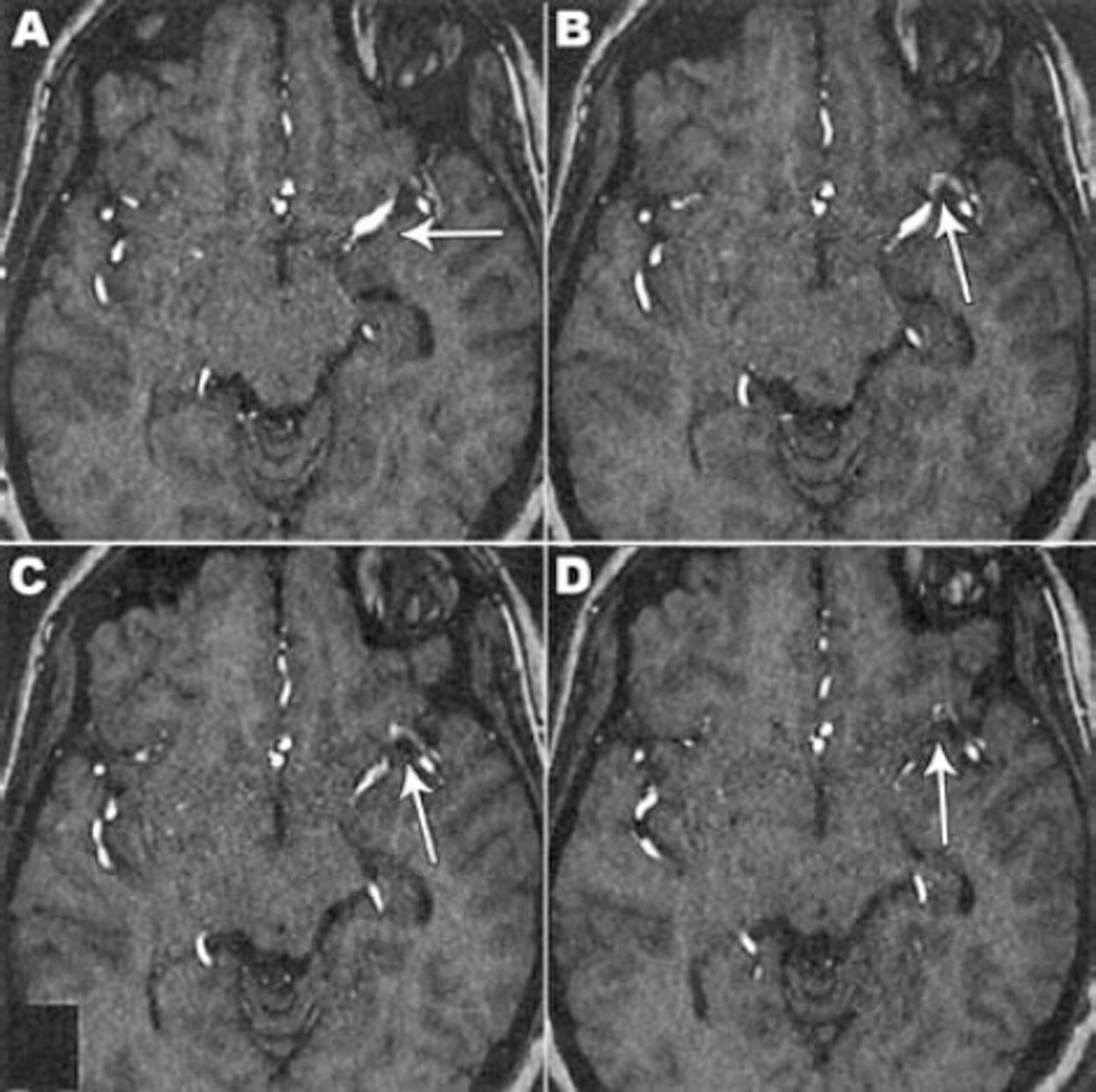
3-D time-of-flight magnetic resonance angiogram (3 hours after stroke onset) showed A) left middle cerebral (MCA) segment with contrast enhancement, B), C), & D) signal attenuation from the M2 segment of the left MCA depicted with arrows graded as partial thrombo-embolic occlusion.

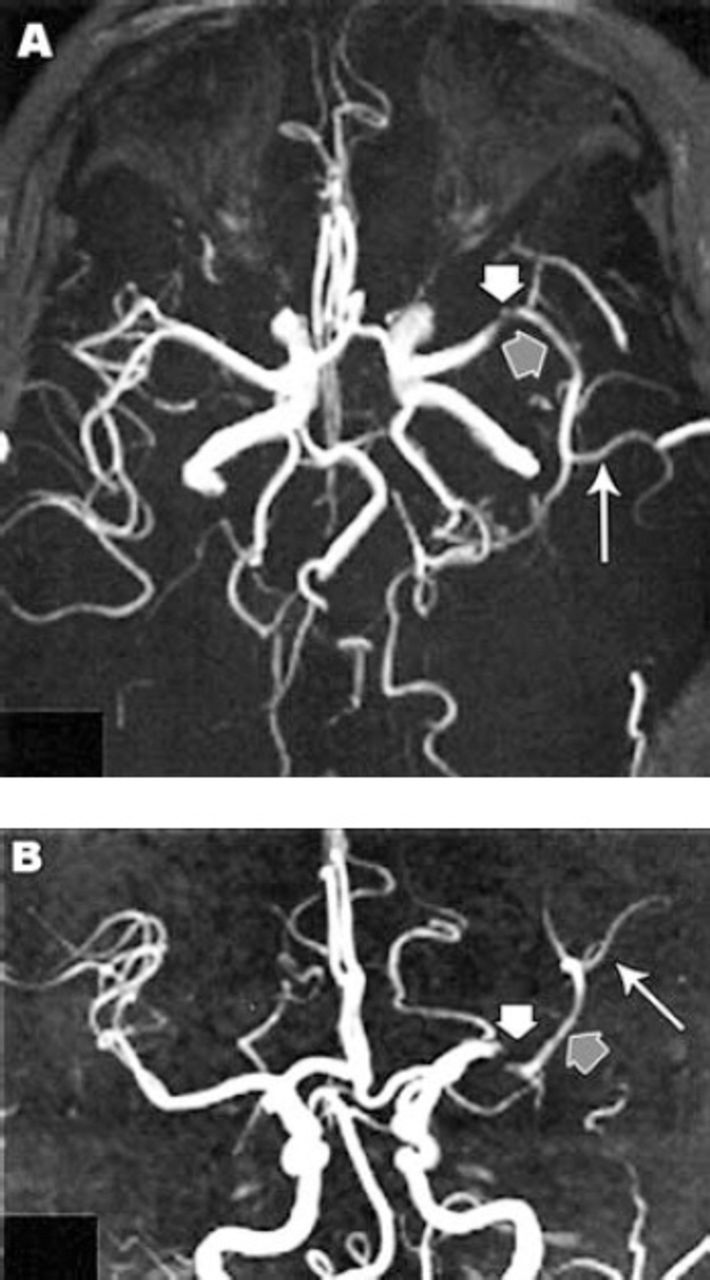
Maximum intensity projection 3-D time-of-flight magnetic resonance angiogram of the circle of Willis (3 hours and 30 minutes after stroke onset) showing: A and B) thrombo-embolic filling defect at the M2 segment (short white arrows in A and B), narrowing distal M2 segment (short grey arrows in A and B) and pruning of M3 segment branches (long white arrow in A and B) of the left middle cerebral artery.
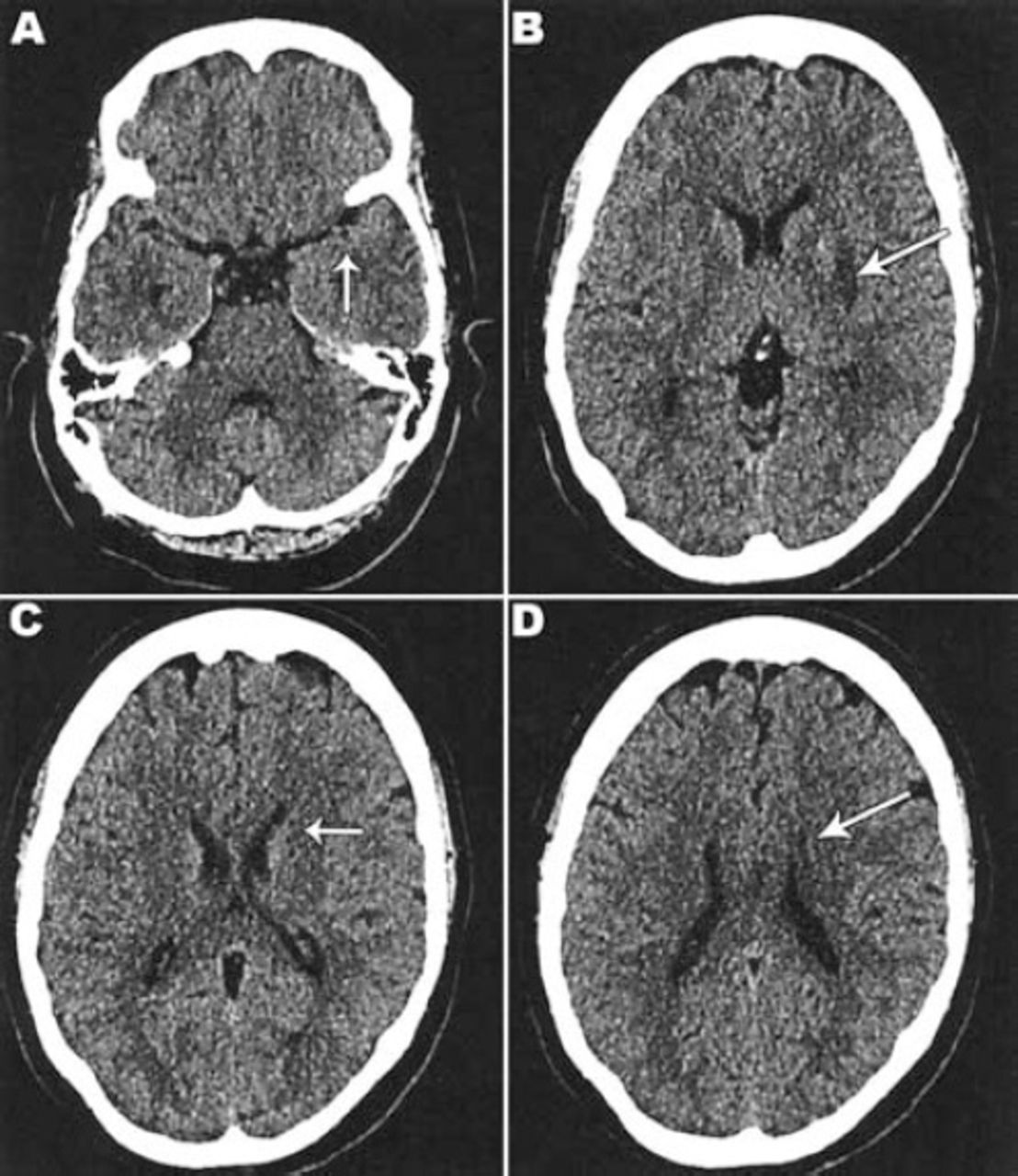
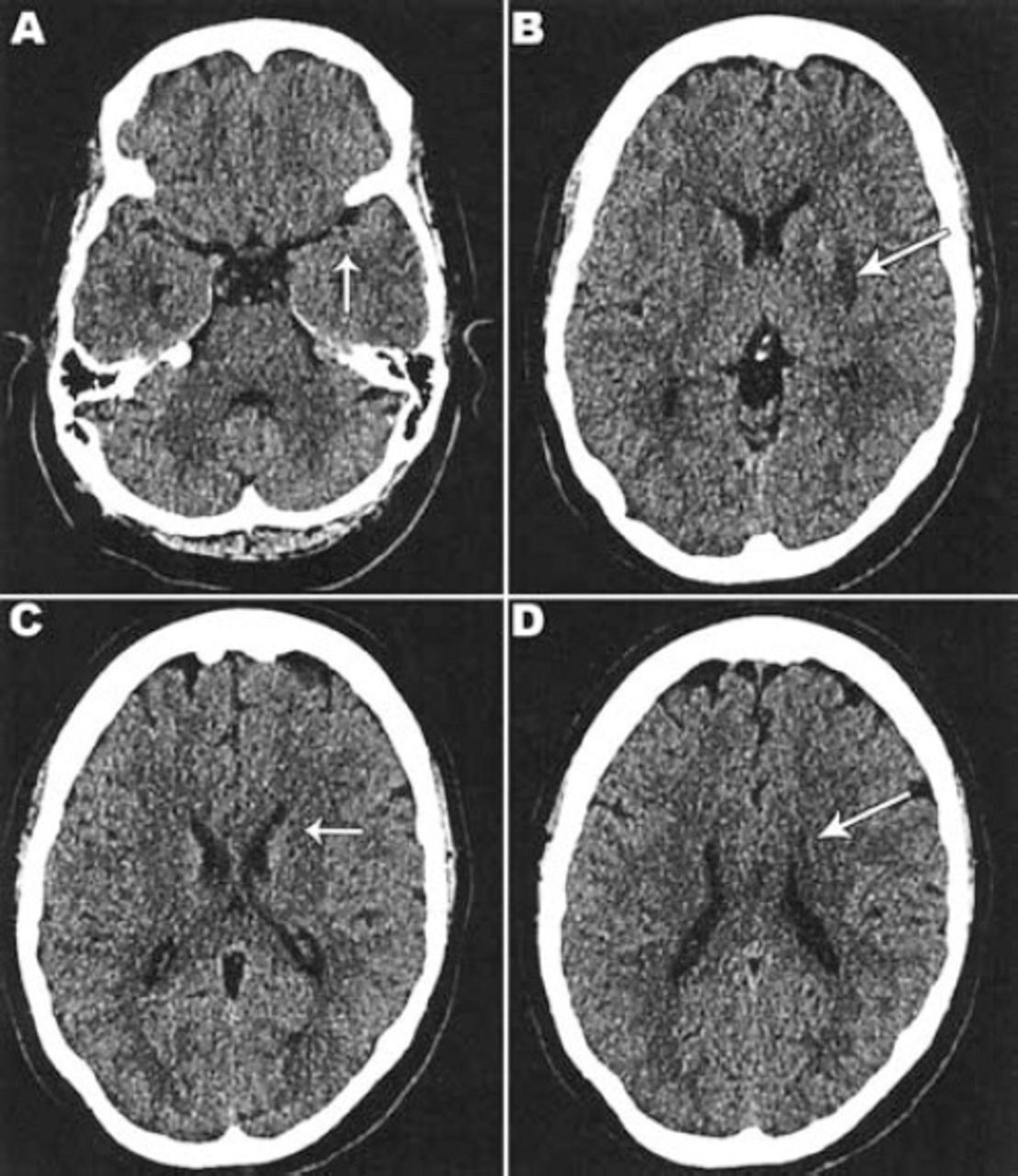
Non-contrast CT scan brain (26 hours after stroke [22 hours after IV thrombolysis]) showed: A) previously seen hyperdense left middle cerebral artery dot sign in the M2 segment is less prominent. B), C) and D) showed acute linear infarction at the left lentiform and head of caudate nuclei.
Clinically, in the first 24 hours post thrombolysis, her motor power improved to normal in the right side with the only weakness remaining in the face, which also recovered within the next few days. She did not have any complications post thrombolysis. While in hospital she underwent workup to determine the stroke etiology. Carotid ultrasound was normal with no atheromatous plaques or stenosis. Transesophageal ECHO showed free left atrial appendage, no patent foramen ovale (PFO), and no vegetations. Venous doppler did not show any signs of deep vein thrombosis in the lower limbs. Hypercoagulability panel showed normal values for protein C, protein S, factor V, antithrombin III and homocysteine (Table 1).
Complete laboratory test data (some test results were rechecked on follow-up as shown by values with / sign).
The diagnostic criteria for SLE by the American College of Rheumatology (ACR) have some inherent weaknesses, which led a consensus group of experts Systemic Lupus International Collaborating Clinics (SLICC) to propose a revised criteria,4 which requires either the patient satisfies at least 4 of 17 criteria including at least one of 11 clinical criteria, and one of 6 immunological criteria, or the patient has biopsy-proven nephritis compatible with SLE in the presence of antinuclear or anti-double stranded DNA antibodies. A clinical diagnosis of SLE with secondary antiphospholipid syndrome presenting with acute MCA ischemic stroke as the first manifestation was made, and after recovery she was started on lifelong oral warfarin anticoagulation with regular INR monitoring. She followed up with us over the next 6 months with no residual deficit. A follow-up MRI brain (Figure 6) plus MRA of cerebral circulation showed patent M2 segment of left MCA, chronic infarction at left lentiform nucleus and head of caudate nucleus.
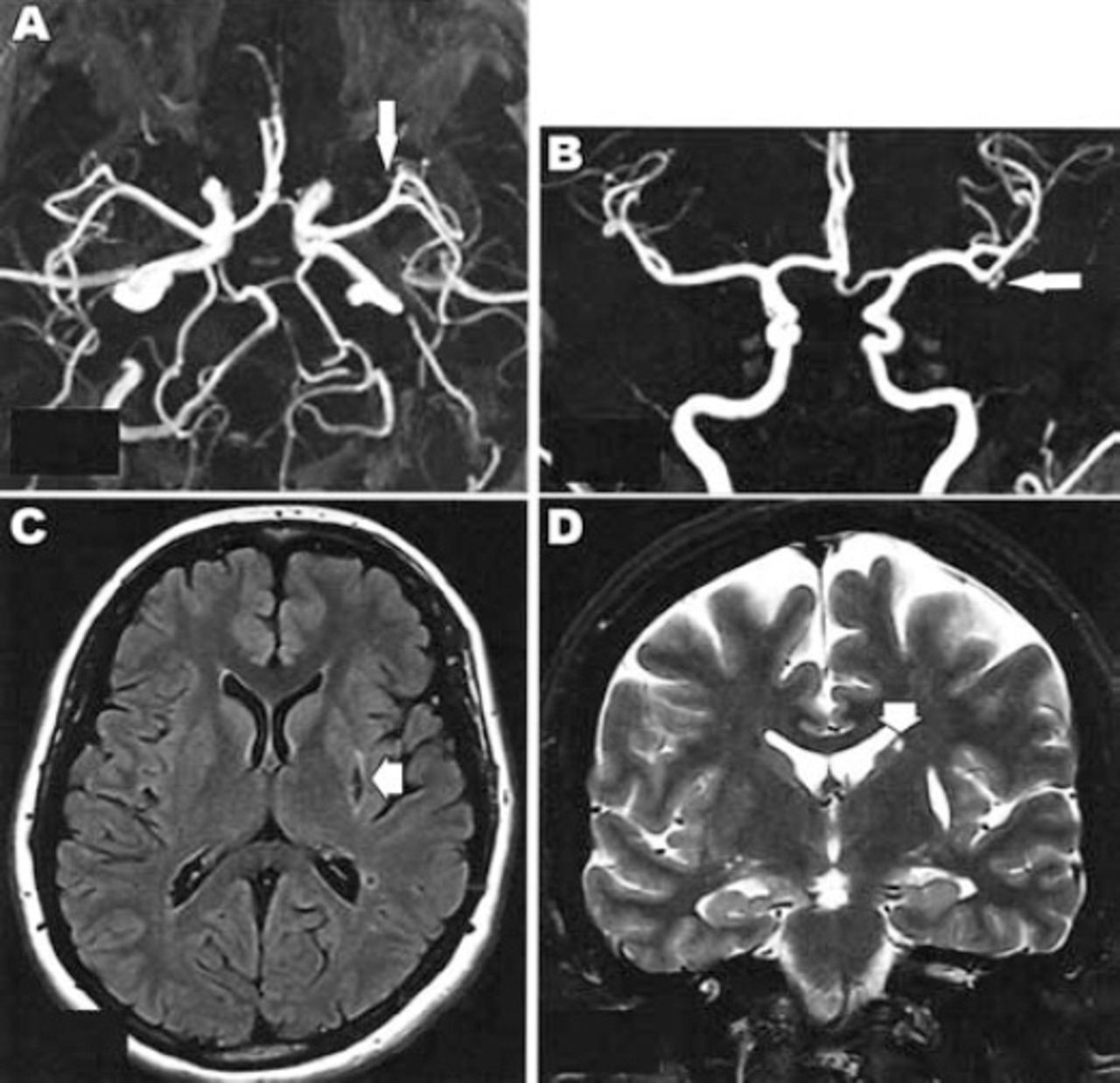
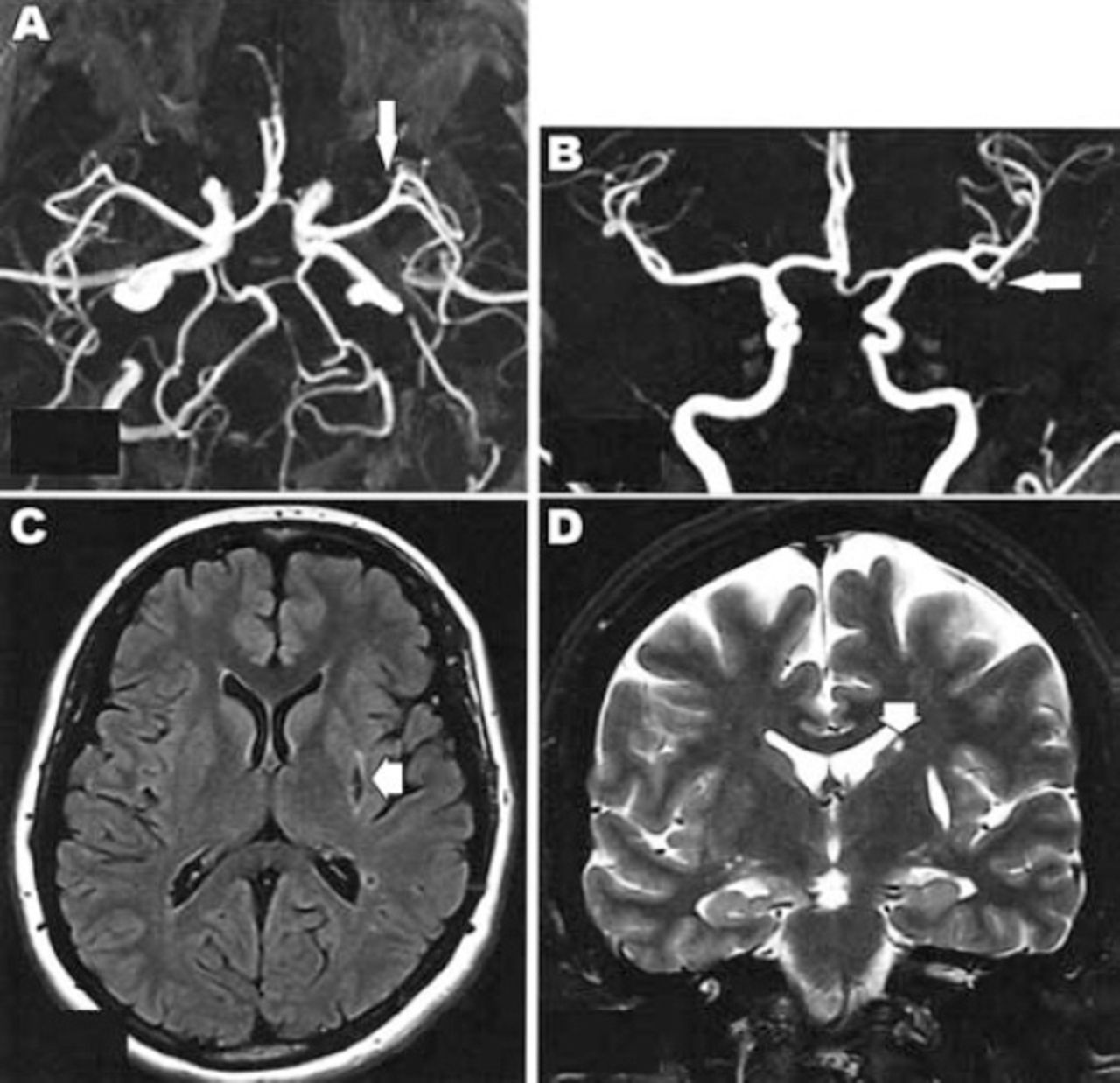
Follow up coronal A) and axial B) maximum intensity projection 3-D time-of-flight magnetic resonance angiogram, axial fluid attenuated inversion recovery [FLAIR] C) and coronal D) T2 WI MRI showing: A) Patent M2 segment of left middle cerebral artery. B) Good filling of M3 segment branches. C) Chronic infarction at left lentiform nucleus. D) Chronic infarction at head of caudate nucleus.
Discussion
In the management of acute ischemic stroke, timely recanalization and restoration of cerebral blood flow using thrombolytic therapy is the desired immediate result; rescue of ischemic penumbra and improvement in clinical outcome is the desired end result. With time delay, the risk of hemorrhagic transformation is increased with thrombolytic use. In the United States,5 around 22% of all ischemic stroke patients present at less than 3 hours, but only around 8% meet eligibility criteria for thrombolysis treatment.
Complement deposition on platelets as a marker showed positive correlation between platelet deposition of complement activation product (C4d) and stroke severity by the NIHSS and infarct volume by MRI.6 Patients who were platelet C4d positive had significantly more severe stroke (NIHSS median 17.5 versus 5, p=0.003) and greater infarct volume (median: 17.4 ml versus 2.9 ml, p=0.06) than those who were platelet C4d negative. Also, platelet C4d positive patients were more likely to have stroke in the total anterior circulation compared with those platelet C4d negative (50% versus 7%, p=0.004). Mortality risk due to stroke or other cerebrovascular disease is doubled as compared with non-SLE controls.7 There is high association between APL and stroke in SLE. The presence of persistently elevated APL antibodies of different specificities increases the risk of stroke more than a single APL does. A report from the Framingham Cohort and Offspring Study8 noted an increased risk of ischemic stroke associated with anticardiolipin antibodies limited to women (hazard ratio for women 2.6; 95% confidence interval 1.3-5.4).
The National Institute of Neurological Disorders and Stroke (NINDS) trial9 results showed that rtPA improves functional outcome at 3 months if given within 3 hours of symptom onset, or within 3 hours of when a patient was last seen normal in cases where onset time is unknown. The third trial of the European Cooperative Acute stroke study (ECASS III)10 found this beneficial even up to 4.5 hours. Each 15 minute time reduction to rtPA initiation corresponded to an increase in odds of walking independently at discharge of (4%) and being discharged to home rather than an institution.11 A meta-analysis12 showed favorable outcome far better for 0 to 90 minutes than at a later time frame, and beyond 4.5 hours harm may exceed benefit. The optimal approach to non-hemorrhagic strokes management in SLE is challenging, emphasizing the importance of full risks and potential benefits assessment of a particular approach in an individual patient. The mainstay treatment after stroke is antiplatelet aspirin or warfarin anticoagulation based on individual risk profile as in our case that had an ischemic stroke with criteria confirming diagnosis of antiphospholipid syndrome.
Vessel recanalization studies13 showed rtPA success at 46.2%. Persistent large vessel occlusion is associated with early neurologic deterioration and poor functional outcome. A few case series14 have MCA recanalization at 24 hours after rtPA in 53-68%. Comparing MRI-based thrombolytic treatment15 within 3-6 hours with conventional CT-based treatment within 3 hours has shown similar recanalization rates and functional outcomes; however, MRI helps in excluding patients who will not benefit. The present case is a rare event in terms of rtPA use for acute MCA occlusion heralding an underlying latent systemic lupus with secondary antiphospholipid syndrome that was diagnosed first time presenting with acute ischemic stroke as a primary problem. Due to early diagnosis, use of multimodality imaging, and thrombolytic intervention she improved with no residual sequelae. On literature review, we were unable to source IV rtPA thrombolysis and subsequent neurological course previously described in patients presenting with acute ischemic stroke as the first presentation of SLE. This case provides an important opportunity to consider the pathophysiology of stroke in systemic lupus and its implication for thrombolytic use with further studies in well-characterized patient groups and perhaps other autoimmune conditions where hypercoagulability is a significant clinical manifestation.
In conclusion, our patient showed excellent outcome with rtPA in this acute anterior circulation stroke, which was her first manifestation of undiagnosed systemic lupus disease. Stroke thrombolysis use for an acute vascular event as a presenting manifestation of autoimmune diseases like SLE is a rare experience, which was not previously sourced in the literature concerning tPA and stroke.
- Received May 11, 2014.
- Accepted November 18, 2014.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.