


Article Figures & Data
Figures
- Figure 1
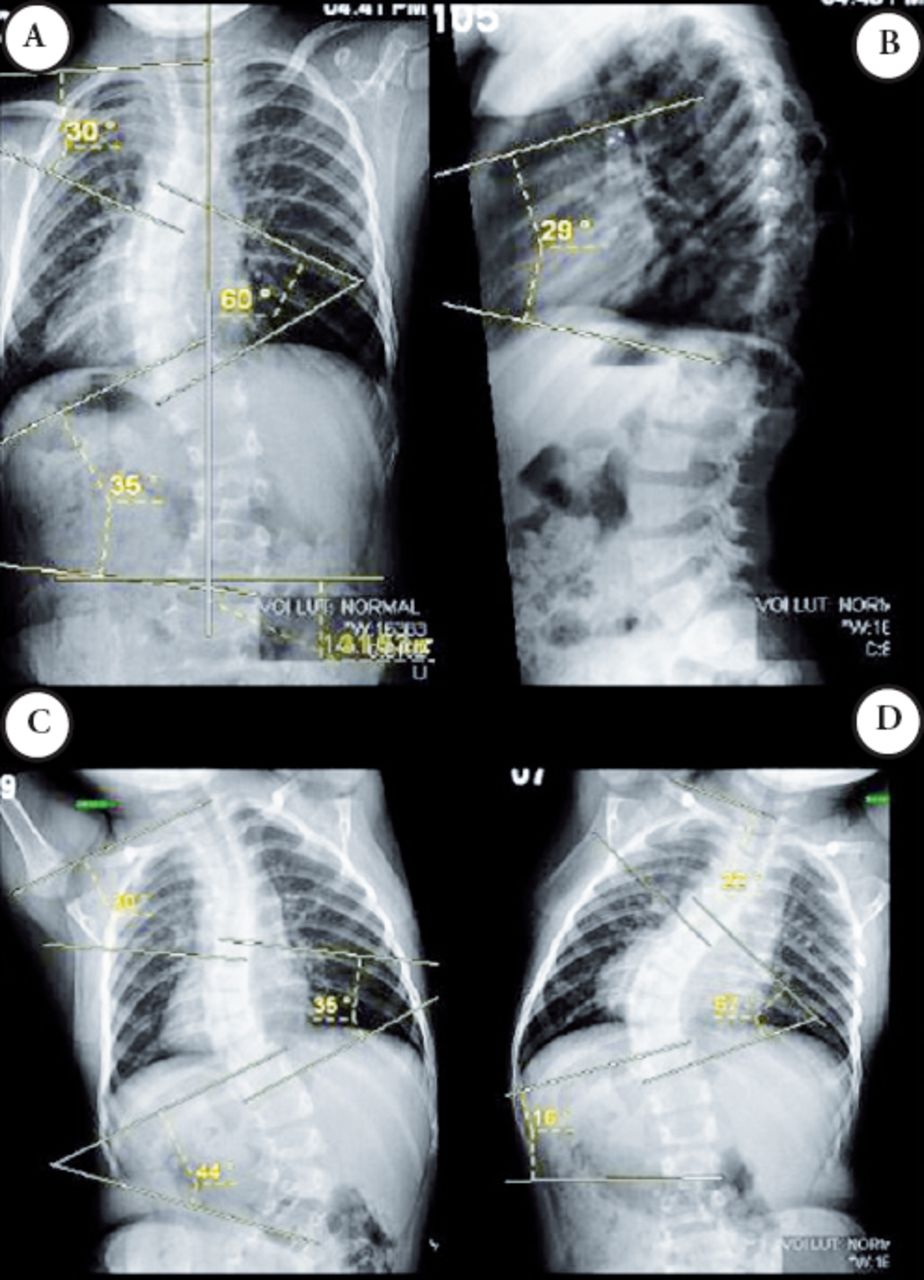
Scoliogram of a 3-years and 3 months-old girl with severe idiopathic early-onset scoliosis, progressive and non-responsive to conservative treatment: A) Preoperative standing PA scoliogram; B) standing lateral scoliogram; C) Preoperative left side bending film (PA); and D) right side bending film (PA). PA - posteroanterior
- Figure 2
Surgical view of a posterior thoracolumbar spine approach for the implantation of the pedicle screws and magnetic rods (1 incision at high thoracic and another at lumbar region) in the same patient, which x-ray was presented before with severe scoliosis.
- Figure 3
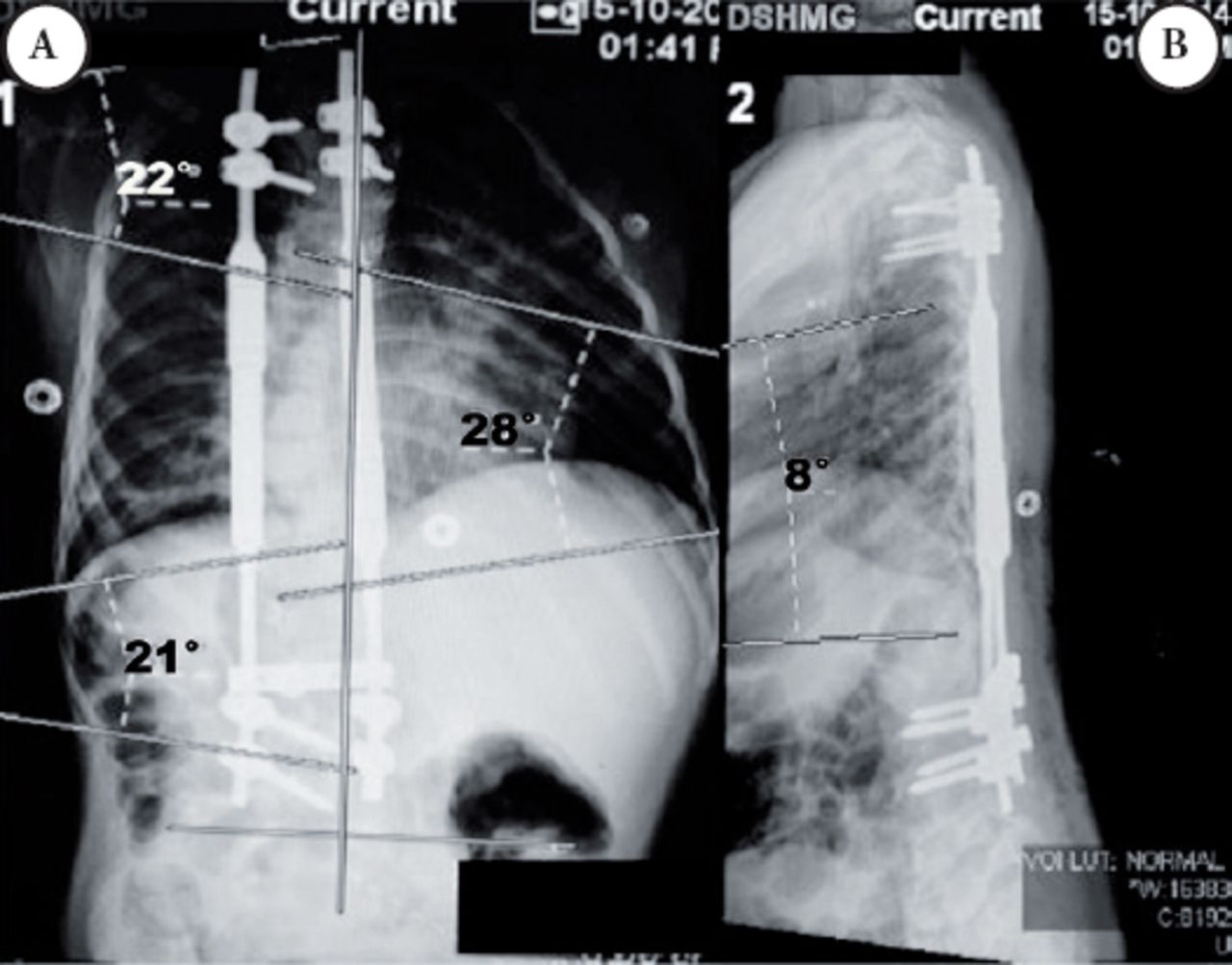
Scoliogram of the same 3 year-old girl at first postoperative day: A) standing posteroanterior spinal x-ray; and B) standing lateral.
- Figure 4
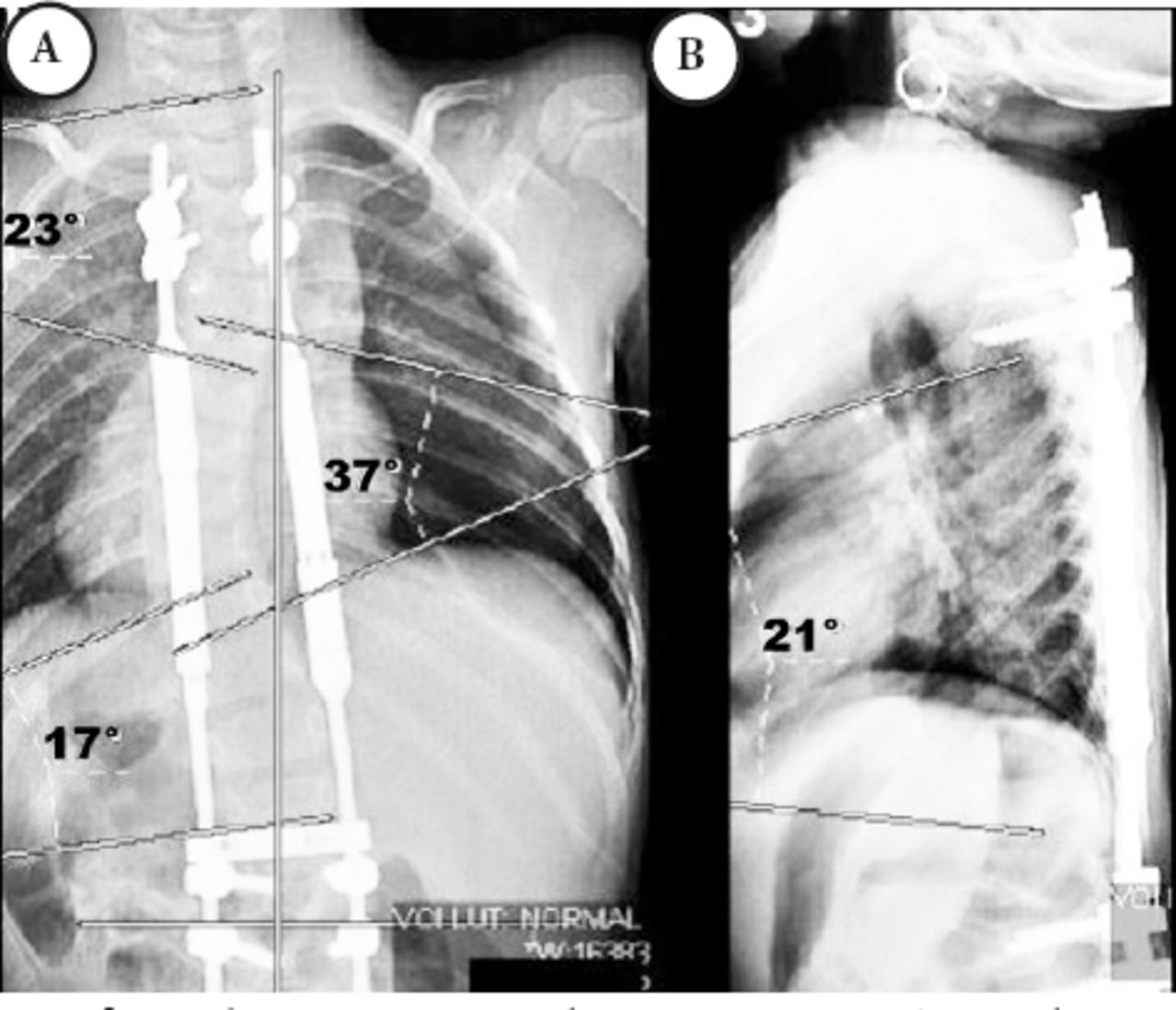
Scoliogram at 2 months postoperative: A) Spinal x-ray after the first distraction standing posteroanterior; and B) standing lateral.




Tables
- Table 1
Descriptive summary of all included studies regarding MCGR for severe pediatric scoliosis.
Authors Level of medical evidence Description Comment Akbarnia et al24, 2013 IV Prospective case series of 14 patients who underwent surgery for scoliosis using MCGR, mean age of 8.8 years. Five had SR and 9 had DR surgery. Mean follow-up was 10 months. The main Cobb angle of the main scoliosis changed from 60° to 34° after initial surgery, and 31° at latest follow-up. The mean spinal length T1-S1 changed from 292 mm to 338 mm at the latest follow-up. Complications occurred in 5 (35.7%) of the patients. This paper supports the use of MCGR for severe pediatric scoliosis, as a safe and effective technique. DR achieved better curve correction and greater spinal height compared with SR. Cheung et al,13 2012 IV Prospective case series of 5 patients who underwent surgery for scoliosis using MCGR, mean age of 11 years. Mean follow-up was 19 months. Regarding the case of 2 patients with 24 months’ follow-up, 1 had SR and 1 DR; the mean Cobb angle of the main scoliosis changed from 67° to 29° at latest follow-up; regarding the kyphosis, changed from 43° to 34° at latest follow-up. The mean spinal length T1-S1 changed from 199 mm to 229 mm at the latest follow-up. Complications occurred in 2 (40%) of the patients. This paper supports the use of MCGR for severe pediatric scoliosis, as it minimizes surgical scarring and psychological distress, improves quality of life, and is more cost-effective than the traditional GR. Cheung et al,22 2014 IV Case report of a 12-year-old girl with severe kyphoscoliosis, syringomyelia and Chiari I malformation who underwent implantation of the MCGR. She had daily distractions of the implant over the course of 2.5 months, obtaining 47 mm of total distraction length. The Cobb angle of the main scoliosis changed from 109° to 94° after initial surgery, and 66° at 2.5 months follow-up; regarding the kyphosis, the curve of 72° did not change after the initial surgery, and reduced to 62.2°. After the final fusion, the main scoliosis reduced to 28.2°, and the thoracic kyphosis to 54.7°. There was no complication or implant failure. This paper supports the use of MCGR for severe pediatric kyphoscoliosis, allowing gradual correction of the deformity while the patient is awake, where the device has been shown to be safe and effective. Dannawi et al,15 2013 IV Prospective case series of 34 patients who underwent surgery for scoliosis using MCGR, mean age of 8 years. The mean follow-up was 15 months. Twenty two had DR and 12 had SR surgery. The mean Cobb angle changed from 69° to 41° at latest follow-up; regarding the thoracic kyphosis, changed from 33° to 32° at latest follow-up. The mean spinal length T1-S1 changed from 304 mm to 348 mm at the latest follow-up. Complications occurred in 8 (23.5%) of the patients. This paper supports the use of MCGR for severe pediatric scoliosis, as a safe and effective method, with the avoidance of repeated surgical lengthening. Hickey et al,17 2014 IV Retrospective case series of 8 patients who underwent surgery for scoliosis using MCGR, mean age of 4.5 years. In 4 patients in the primary group and of 10.9 years. In the 4 patients of revisions from other surgeries, the mean follow-up was 28 months. Six had DR and 2 had SR surgery. In patients who had MAGEC as a primary procedure, mean Cobb angle changed from 74° to 42° at latest follow-up; mean spinal length T1-S1 changed from 215 mm to 286 mm at the latest follow-up. In patients who had MAGEC as a revision procedure, mean Cobb angle changed from 45° to 44° at latest follow-up. The mean spinal length T1-S1 changed from 306 mm to 373 mm at the latest follow-up. Complications occurred in 4 (50%) of the patients. This paper supports the use of MCGR for severe pediatric scoliosis, when used as either a primary or revision procedure. Although implant-related complications are not uncommon, the avoidance of multiple surgeries following implantation is beneficial compared with traditional GR systems. Yoon et al,23 2014 IV Prospective case series of 6 patients who underwent surgery for neuromuscular scoliosis using MCGR, mean age of 7.5 years. The mean follow-up was 30 months. Five had DR and 1 had SR surgery. The mean Cobb angle changed from 87° to 34° at latest follow-up; regarding the thoracic kyphosis, changed from 66° to 36° at latest follow-up. Mean improvement in postoperative FVC was 14.1% and FEV1 was 17.2%. Complications occurred in 2 (33.3%) of the patients. This paper supports the use of MCGR for severe pediatric scoliosis, which is associated with significant improvement in deformity correction and postoperative pulmonary function. N - number, MCGR - magnetically controlled growing rod, SR - single-rod, DR - dual-rod, FVC - forced vital capacity,
FEV1 - forced expired volume in 1 second, GR - growing rod
- Table 2
Quantitative summary of the papers related to magnetically controlled growing rod for severe pediatric scoliosis.
Characteristics Description (after systematic review) Papers included 6 papers13,15,17,22-24 Level of medical evidence All Level IV of medical evidence for therapeutic studies44 Patients N=68 patients, mean=11.33 patients/study (1-34) Follow-up Mean=16.9 months (2.5-36 months) Age Mean age=8.38 years (3-14 years old) Gender Male = 32/68 (47.1%) patients, Female = 36/68 (52.9%) patients Pathological classification of scoliosis5 Main type: n=68
Idiopathic = 26 (38.23%)
Neuromuscular = 36 (52.94%)
Congenital = 6(8.82%)Surgical technique regarding rod construct Dual-rod (DR) n=65
43 (66.15%)
Single-rod (SR)
22 (33.84%), Information available = 65/68 (95.58%) of the casesDistractions Mean interval = 55.33 days (1-135), Mean distraction per episode = 3 mm (1.5-4.5) Preoperative curve, scoliogram Coronal plane Cobb angle=67.4°
Sagittal plane Cobb angle=50.6°
Data available for comparison = 83.33% (5/6) of the articles
Regarding the rod construct=DR
Coronal plane Cobb angle=65.9°
SR
Coronal plane Cobb angle=69.6°, (p=0.1209)Latest follow-up postoperative curve, scoliogram Coronal plane Cobb angle=39.1°=47.75% of final correction,
Sagittal plane Cobb angle=42.4°=16.21% of final correction
Regarding the rod construct*
DR
Coronal plane Cobb angle=36.8°=44.16% of final correction
SR
Coronal plane Cobb angle=43.0°=38.22% of final correction (p=0.0007)Preoperative T1-S1 spinal length, scoliogram 300.4 mm
Data available for comparison=66.66% (4) of the articles Regarding the rod construct*=DR=298.7 mm, SR=303.5 mm (p=0.0052)Latest follow-up postoperative T1-S1 spinal length, scoliogram 345.3 mm
35.8 mm=13.57% of T1-S1 total lengthening
2.05 mm/month
Regarding the rod construct
DR=347.0 mm
48.3 mm=13.92% of T1-S1 total lengthening
2.8 mm/mo
SR=342.3 mm
38.8 mm=10.48% of T1-S1 total lengthening
2.29 mm/month (p=0.0042)Postoperative complications Complication rate= 21/68 (30.88%) of the patients
Regarding the rod construct, n=36= DR = 36 (25%)
Wound infection or healing problem= 36 (2.77%)
Prominent implant= 3 (8.33%)
Loss of distraction= 3 (8.33%)
Rod breakage= 1 (2.77%)
Implant pull-out= 1 (2.77%)
Specified cases for comparison= (36/43) 83.72% of the patients
SR, n=19= 6 (31.57%) (p=0.7516)
Wound infection or healing problem= 2 (10.52%) (p=0.2716)
Prominent implant=0 (p=0.5437)
Loss of distraction, n=19= 2 (10.52%) (p=1.0000)
Rod breakage= 2 (10.52%) (p=0.2716)
Implant pull-out = 0
Specified cases for comparison= (19/22) 86.36% of the patients (p=1.0000)N - number, DR - dual-rod, SR - single-rod
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.