


Abstract
Infarction of the symmetrical middle cerebellar peduncles is often induced by ischemic cerebrovascular disease. Adams described the anterior inferior cerebellar artery (AICA) syndrome as early as 1943, but clinical and imaging studies following this failed to shed more light regarding the condition until the advent of magnetic resonance imaging that comprehension regarding AICA improved significantly. Infarction of the middle cerebellar peduncles (MCP) is uncommon and the endovascular treatment of this condition is even more rare. We studied 4 patients with simultaneous bilateral cerebellar infarction of whom 2 received intracranial vascular therapy and demonstrated improvement in symptoms. Our findings suggest that patients with vertebral basilar artery stenosis with potential bilateral cerebellar infarction may benefit from endovascular treatment.
The middle cerebellar peduncle (MCP) is supplied mainly by the anterior inferior cerebellar artery (AICA) and partly by the superior cerebellar artery. Bilateral infarction of the MCP is rare, and the therapy report of the stent is even more rare. There was only one case report of endovascular stent treatment for bilateral infarction of the MCP. We described 4 patients with bilateral infarction of the MCP, and 2 patients were treated with endovascular stenting and received impressive results.
Case Report
Case 1
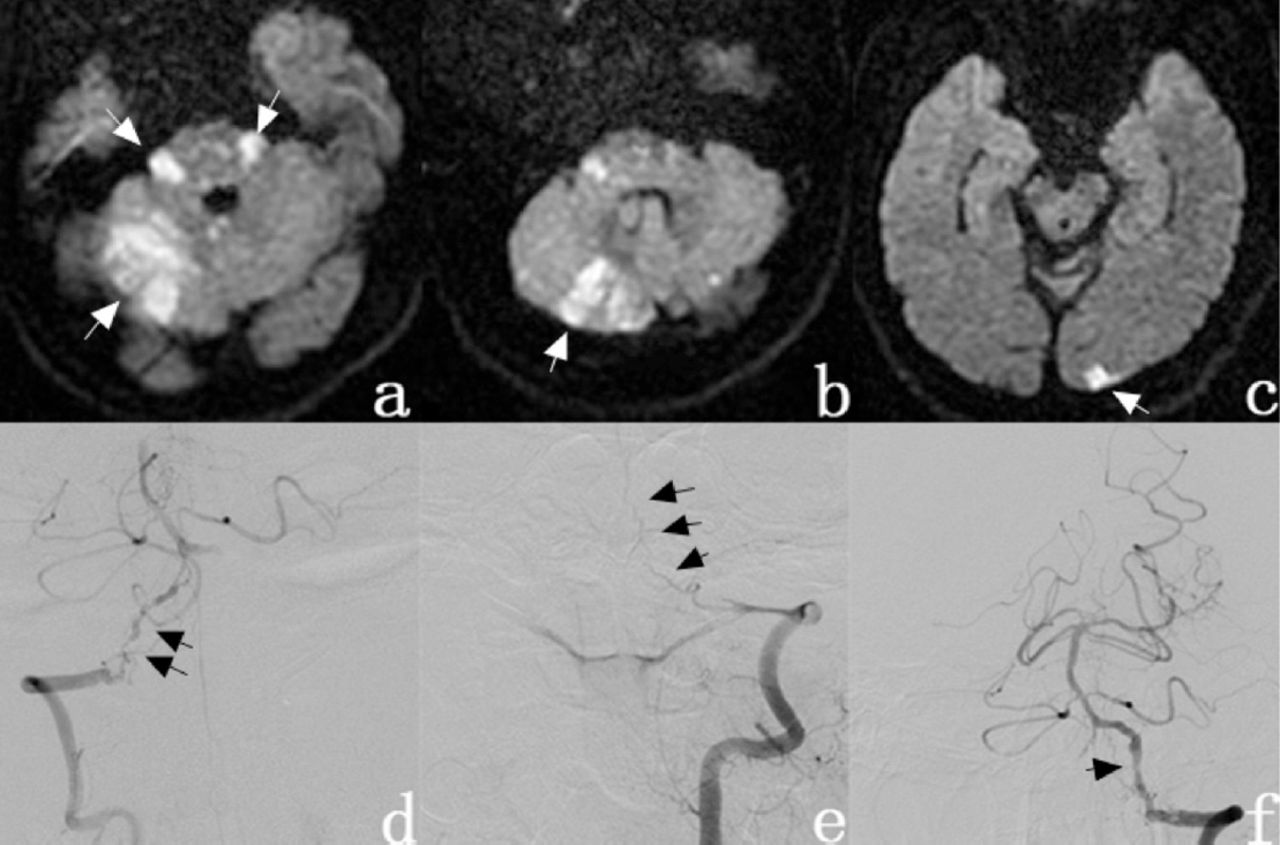
A 50-year-old male patient with long-standing hypertension and episodes of dizziness for 2 years, presented with slurred speech, right side numbness and instability while standing. Neurologic examination revealed right side hearing loss, weakness of right side limbs, right side ataxia, and hyperalgesia. He had recurring transient left eye abduction dysfunction and diplopia following admission. He underwent left vertebral artery angioplasty on January 13, 2013 (Figure 1) and the symptoms improved significantly after stenting. There was significant relief in right side weakness and dysarthria while nystagmus and dyskinesia recovered significantly.

- Diffusion Weighted Image showing A & B) spotty high signal in bilateral cerebellar hemispheres and vermis of the cerebellum, pons, right thalamus (arrow); C) with left occipital high-intensity (arrow). D) Digital subtraction angiography showed right vertebral artery and basilar artery stenosis (arrow) and E) left vertebral artery distal was totally occluded. F) Left vertebral artery, basilar artery, bilateral inferior cerebellar artery, and bilateral superior cerebellar artery were visible after left vertebral artery recanalization.
Case 2
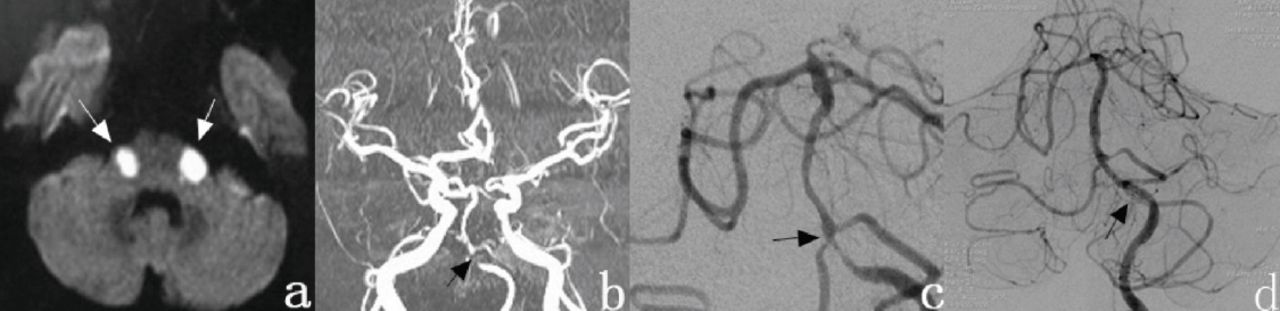
A 61-year-old male patient presented with slurred speech, unsteady gait, dizziness and standing instability for 20 days. Following 3 days of work, he presented with limited abilities in left limb, dysarthria, dysphagia, aspiration, bilateral hearing loss and somnolence. Physical examination revealed that the pupil size of both eyes was not equal. Left pupil diameter was approximately 3 mm and the right was 4mm. Both eyes showed horizontal nystagmus, hearing significantly decreased, muscle strength of all four limbs was reduced and Babinski’s sign was elicited on the left side. On presentation at the hospital, he was started on dual antiplatelet medication (acetylsalicylic acid and clopidogrel). The patient’s physical activity significantly improved when following stent implantation after admission and hearing was restored. However, serious limbs and trunk ataxia persisted when he was discharged (Figure 2).

- Diffusion Weighted Image shows A) high-intensity bilateral symmetric round infarctions (arrow). B) MRA shows that the right vertebral artery is invisible, severe stenosis of the segment from the left vertebral artery distal to the basilar artery or occlusion (lower arrow). C) Cerebral angiography shows diffuse severe stenosis from the V4 segment of the left vertebral artery to the proximal end of the basilar artery and moderate stenosis at the origin of the right AICA (arrow). D) The stenosis was relieved following stent implantation (arrow) in the inferior segment of the basilar artery and the stenosis of the right vertebral artery. artery stenosis (arrow).
Case 3
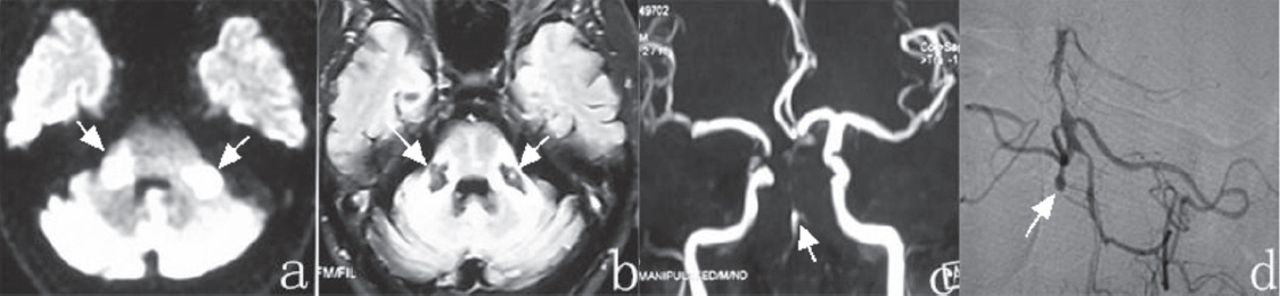
A 68-year-old male patient presented with recurrent attacks of nausea, vomiting, vertigo and severe ataxia for 3 years, sudden slurring of speech and unsteady gait. He was admitted to a local hospital. He had transient dysarthria, somnolence, hearing loss, unsteady gait after vertigo, vomiting and nausea. Physical examination revealed bilateral horizontal nystagmus and ataxia of limbs and trunk. He was unable to complete both heel-knee-tibia test and finger-nose test. Diffusion weighted image (DWI) examination is shown in Figure 3. After 14 days of hospitalization conservative treatment there was a slight improvement in dysarthria, but there were significant ataxia and bilateral deafness.

- Diffusion Weighted Image shows A) high-intensity areas in the bilateral middle cerebellar peduncles (arrow). B) Bilateral middle cerebellar peduncle shows symmetrical hypodensity areas on T1-weighted images (arrow). C) MRA shows that bilateral vertebral artery is invisible and the basilar artery at the end of the vertebral artery can be visualized (arrow). Bilateral anterior inferior cerebellar artery, superior cerebellar artery and posterior cerebral artery are not invisible. D) Cerebral angiography showed occlusion of the V5 segment (arrow)of the right vertebral artery, moderate to severe stenosis of the left vertebral artery, basal segment of the basilar artery shows swelling, bilateral superior cerebellar artery visible but obviously thin, the right posterior cerebral artery is invisible and moderate to severe stenosis of the left posterior cerebral artery.
Case 4
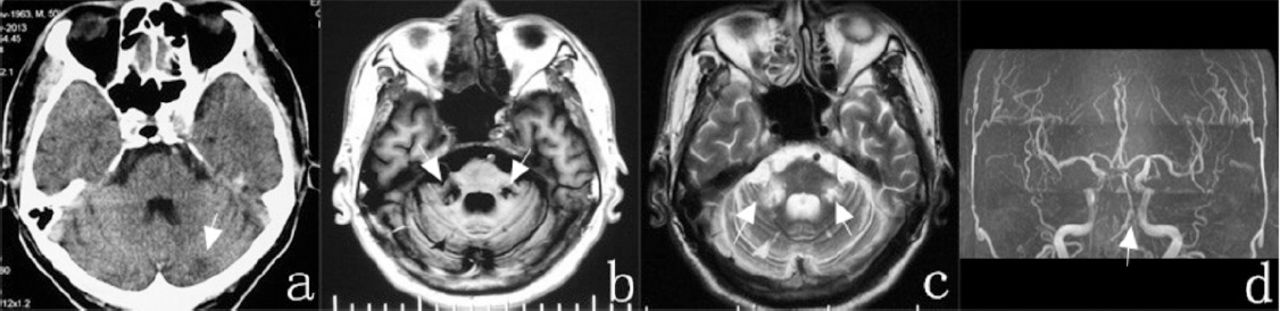
A 51-year-old male patient presented with dizziness that had persisted for more than 5 hours, accompanied by nausea, vomiting, slurred speech, diplopia dysphagia, tinnitus, weakness and unsteady gait. He was admitted. Physical examination revealed that alternating hand movement test and heel-knee-tibia test were mildly abnormal. Following conservative therapy, the patient still had slurred speech and gait instability. Diffusion Weighted Image examination is shown in Figure 4.

- CT scan showed A) patchy low-density foci in the left cerebellar hemisphere (arrow). B & C) MR shows low signal intensity from bilateral middle cerebellar (arrow). D) MRA shows bilateral vertebral artery stenosis (arrow).
Discussion
Image analysis of 4 cases demonstrated that the infarction lesion was located in the middle cerebellar peduncles and other AICA supply area with or without PICA or involvement of SCA supply area. We observed an infarct in the SCA area in case 1. Separate AICA infarction can be considered in cases 2, 3 and 4. The treatment consisted mainly of anticoagulation, antiplatelet therapy. Application of stent at the site of stenosis can significantly improve the symptoms in 2 patients.
Infarction of the MCP is a rare type of AICA syndrome. The incidence of anterior inferior cerebellar artery infarction in acute stroke is only 0.9% and represents 5.2% of patients affected the vertebrobasilar territory. Patients with infarction localized in the bilateral middle cerebellar peduncles were rare.1 Adams1 noted rotational dizziness, vomiting, tinnitus and dysarthria on the side of the infarction as well as dysmetria, facial palsy, trigeminal sensory impairment, Horner syndrome and loss of pain and temperature on the opposite side.2 The clinical picture described by Adams1 was called the classic AICA syndrome. The presence of vertigo, ataxia, peripheral facial palsy and ipsilateral hypoacusia means a “complete AICA infarct”.1
Infarction of the MCP is a rare type of AICA syndrome. The incidence of anterior inferior cerebellar artery infarction in acute stroke is only 0.9% and represents 5.2% of patients affected the vertebrobasilar territory. Patients with infarction localized in the bilateral middle cerebellar peduncles were rare.1 Adams1 noted rotational dizziness, vomiting, tinnitus and dysarthria on the side of the infarction as well as dysmetria, facial palsy, trigeminal sensory impairment, Horner syndrome and loss of pain and temperature on the opposite side.2 The clinical picture described by Adams1 was called the classic AICA syndrome. The presence of vertigo, ataxia, peripheral facial palsy and ipsilateral hypoacusia means a “complete AICA infarct”.1 nuclei and roots of the fifth, seventh and eighth nerves which are characteristics of the clinical syndrome.1
Deafness and tinnitus caused by the eighth nerve damage are common symptoms of AICA syndrome since AICA is the source of the internal auditory artery (IAA), which exclusively supply the inner ear. Since deafness and tinnitus are characteristic symptoms of AICA, these symptoms can be used to differentiate between AICA and PICA infarct. Internal auditory artery occlusion is often accompanied by labyrinthine dysfunction. Labyrinthine dysfunction might have been masked by severe ataxia, but it can explain the horizontal nystagmus in cases 2 and 3. Some of the branches of the AICA may constitute the upper and posterior branches of the lateral medulla, supplying the fibers of the ninth and tenth nerves and the superior part of the nucleus ambiguus.3 The involvement of these sites can lead to dysarthria and dysphagia. Our 3 patients presented with obvious dysarthria suggest the possibility of upper medulla involvement. The AICA also supplies the lateral part of the abducens nucleus. Case 3 had recurrent left eye abduction restriction, which may be due to transient ischemia of the left side of the abducens nucleus or abducent nerve. Motor weakness is the common concomitant symptom of AICA, associated with corticospinal tract involvement. From the clinical features of our 4 patients, they have several obvious common features, such as vertigo, ataxia, slurring speech, unsteady gait, and hearing loss (Table 1). Middle cerebellar peduncle is largely supplied by the AICA, but it also receives blood supply from the SCA which anastomoses with the terminal branches of the AICA. As such, the MCP is a watershed area for these 2 arteries.3,6
Clinical manifestation from the clinical features of our 4 patients, they have several obvious common features, such as vertigo, ataxia, slurring speech, unsteady gait, and hearing loss.
Large artery occlusive disease was more frequently observed in cerebellar watershed infarction.6 The common etiology of the AICA infarct is thrombosis superimposed on atheromatous stenosis which is located in the AICA or the basilar artery lower part.2 Symmetrical cerebellar infarction is mostly caused by lesions on one side of the vertebral artery and basilar artery, or bilateral vertebral artery lesions, but the occlusion rarely occurs in AICA. Less frequently the occlusion occurs on the distal part of both vertebral arteries or in the distal part of the ipsilateral vertebral artery.
We speculate that occlusion of both vertebral arteries may lead to hypoperfusion in the watershed area between the AICA and the superior cerebellar arteries, resulting in infarction in the bilateral middle cerebellar peduncles. John described bilateral cerebellar infarction cases, although bilateral AICAs were invisible, but also speculated that the possible mechanism of bilateral cerebellar infarction to be due to arterial stenosis or occlusion, based on blood flow reduction leading to AICA involvement.7
In our study, cerebral angiography showed severe stenosis or occlusion of the vertebral basilar artery system, except in case 2 where there was mild stenosis at the initiation site of the right AICA, while the other cases showed that AICA was not. However, all of our 4 cases demonstrated severe stenosis or occlusion of the vertebral basilar artery. The pathogenic mechanism of MCP infarcts may be the result of hypoperfusion based on arterial stenosis leading to decreased blood flow to the AICA, which could not be completely compensated by the collateral circulation. From the point of risk factors, the 4 patients have long history of hypertension and hyperlipidemia (Table 1). We consider the hyperlipidemia and hypertension lead to atherosclerosis when suddenly decreased blood pressure leads to the hypoperfusion for cerebral infarction. The history of atrial fibrillation cannot be excluded as the cause of cardioembolic infarcts resulting in MCP of case 2. Unfortunately, the patient did not undergo an ultrasound examination. In case 1, the left cerebellum showed high signal intensity and the right superior cerebellum showed patchily or spotted high signal intensity, suggesting that the superior cerebellar artery or anterior inferior cerebellar artery perforating branch occlusion may be associated with hypoperfusion. Case 3 showed basilar artery dilatations distal to the stenosis suggesting arterial dissection. According to the case 4 cerebral angiography, clinical symptoms, the time of onset, and an obvious responsibility lesion in imaging, we excluded the multiple system atrophy.
Anterior inferior cerebellar artery syndrome occurs mostly due to vertebral basilar artery stenosis. The treatment mainly comprises of anticoagulation and antiplatelet therapy. Stent implantation in the stenosed artery has become an important therapeutic avenue. Huo et al8 and Gao et al9 had shown that the combined use of mechanical thrombectomy with angioplasty and stent placement in the basilar artery, with severe underlying intracranial atherosclerotic stenosis, is technically feasible and safe. A previous single case report suggests a possible stent therapy for bilateral cerebellar infarction.10 In this study, we found that cases 1 and 2 had significant improvement following stent placement. We found that the overall prognosis of stenting was better than that without stent implantation. Patients with AICA infarction who have mild symptoms have a good prognosis and fewer sequelae. However, patients with severe stenosis of the vertebral basilar artery system, if not treated in a timely fashion, have an increased risk of large artery infarction that hinders posterior circulation and threatens their lives.
We collected 16 relevant case reports, most of which were treated conservatively in 1991 to 2016, with only one case referred to the stent (Table 2). It can be seen that the endovascular treatment in the bilateral infarction of middle cerebellar peduncles is very rare. We analyzed that the previous treatment for bilateral infarction of middle cerebellar peduncles was a more conservative treatment rather than endovascular treatment for the reason that the development of intravascular treatment technology was relatively backward. But with the development endovascular treatment techniques in recent years, endovascular techniques in the treatment of bilateral infarction of middle cerebellar peduncles will become a new and effective method.
Previous case reports of bilateral cerebellar infarction.
In conclusion, cerebellar infarction is the core area involved in AICA infarction and the main clinical symptoms are vertigo and ataxia. The cause of AICA infarction in almost all cases is atherosclerosis or thrombosis superimposed on the basilar artery stenosis. Patients with severe stenosis of the vertebral basilar artery system, if not treated in a timely fashion, have an increased risk of large artery infarction that hinders posterior circulation and threatens their lives. In addition to the traditional drug therapy, interventional therapy can play a significant role.
At present, the evidence of the conventional basilar artery angioplasty/ stenting of infarction of the middle cerebellar peduncles is lacking. However, there is a growing of literature that shows that angioplasty stenting as a generally acceptable choice in patients with the rapidly deteriorating neurological status from the advanced vertebrobasilar stenosis.
Acknowledgments
The authors would like to thank Dr. XueLiang Qiu from the Department of Radiology, Affiliated Hospital of Weifang Medical College, China for reviewing radiology images.
Footnotes
Disclosure
The authors declare no conflicting interests, support or funding from any drug company.
- Received March 14, 2016.
- Accepted August 11, 2016.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.