


Article Figures & Data
Figures
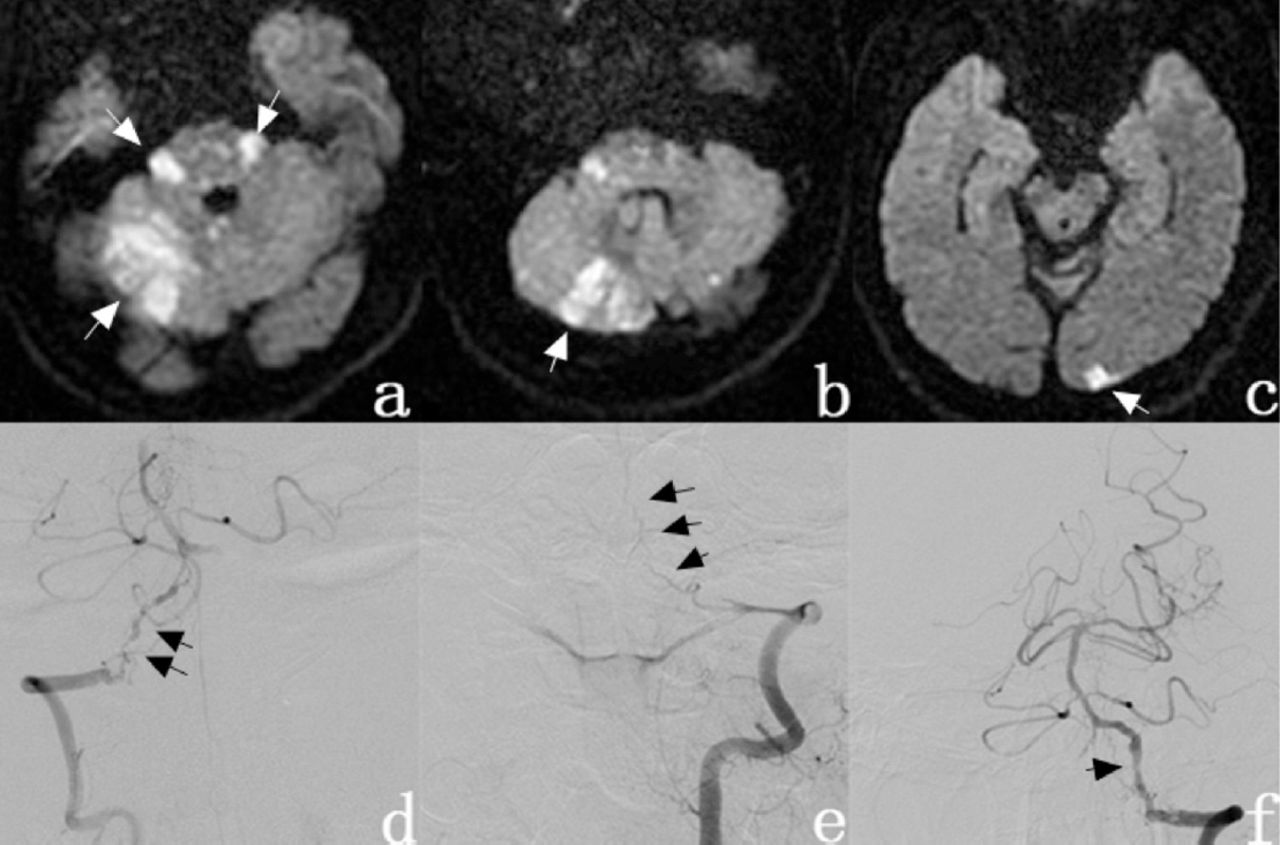
- Figure 1
- Diffusion Weighted Image showing A & B) spotty high signal in bilateral cerebellar hemispheres and vermis of the cerebellum, pons, right thalamus (arrow); C) with left occipital high-intensity (arrow). D) Digital subtraction angiography showed right vertebral artery and basilar artery stenosis (arrow) and E) left vertebral artery distal was totally occluded. F) Left vertebral artery, basilar artery, bilateral inferior cerebellar artery, and bilateral superior cerebellar artery were visible after left vertebral artery recanalization.
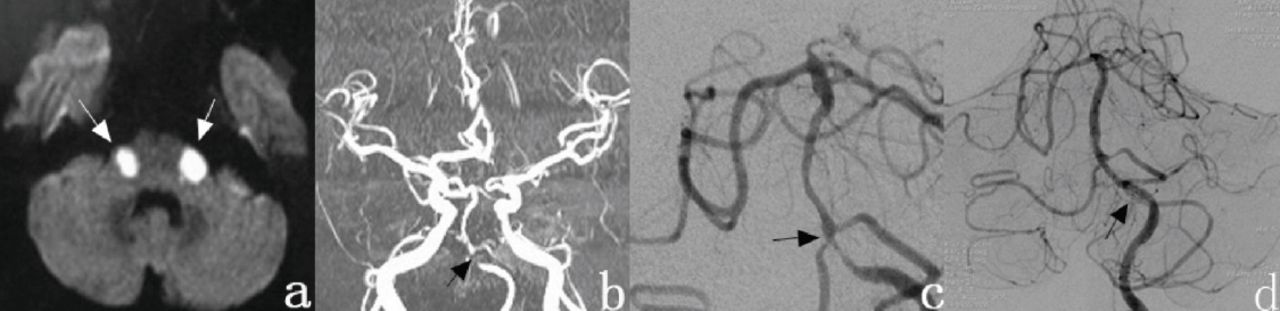
- Figure 2
- Diffusion Weighted Image shows A) high-intensity bilateral symmetric round infarctions (arrow). B) MRA shows that the right vertebral artery is invisible, severe stenosis of the segment from the left vertebral artery distal to the basilar artery or occlusion (lower arrow). C) Cerebral angiography shows diffuse severe stenosis from the V4 segment of the left vertebral artery to the proximal end of the basilar artery and moderate stenosis at the origin of the right AICA (arrow). D) The stenosis was relieved following stent implantation (arrow) in the inferior segment of the basilar artery and the stenosis of the right vertebral artery. artery stenosis (arrow).
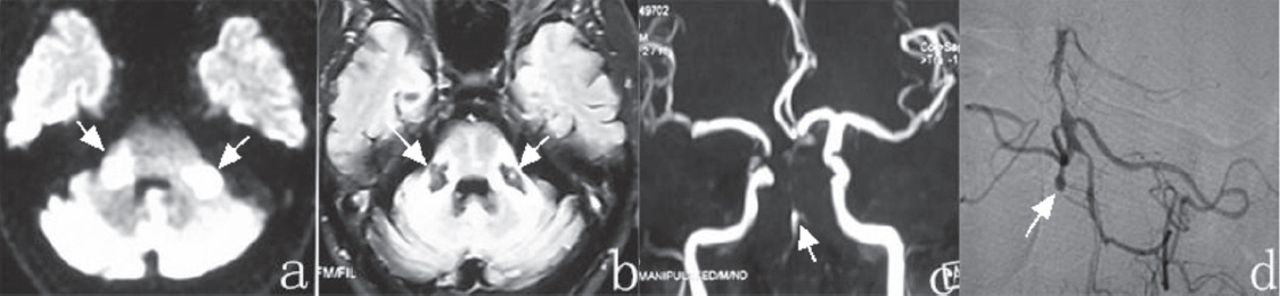
- Figure 3
- Diffusion Weighted Image shows A) high-intensity areas in the bilateral middle cerebellar peduncles (arrow). B) Bilateral middle cerebellar peduncle shows symmetrical hypodensity areas on T1-weighted images (arrow). C) MRA shows that bilateral vertebral artery is invisible and the basilar artery at the end of the vertebral artery can be visualized (arrow). Bilateral anterior inferior cerebellar artery, superior cerebellar artery and posterior cerebral artery are not invisible. D) Cerebral angiography showed occlusion of the V5 segment (arrow)of the right vertebral artery, moderate to severe stenosis of the left vertebral artery, basal segment of the basilar artery shows swelling, bilateral superior cerebellar artery visible but obviously thin, the right posterior cerebral artery is invisible and moderate to severe stenosis of the left posterior cerebral artery.
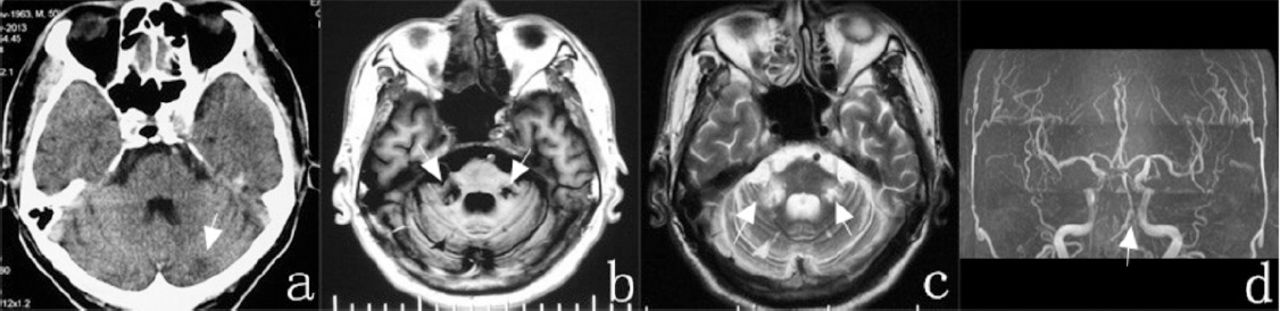
- Figure 4
- CT scan showed A) patchy low-density foci in the left cerebellar hemisphere (arrow). B & C) MR shows low signal intensity from bilateral middle cerebellar (arrow). D) MRA shows bilateral vertebral artery stenosis (arrow).




Tables
- Table 1
Clinical manifestation from the clinical features of our 4 patients, they have several obvious common features, such as vertigo, ataxia, slurring speech, unsteady gait, and hearing loss.
Cases Age (years)/gender Vascular risk factors Symptoms/signs Diagnose Treatment Outcome 1 50/M Hypertension, hypercholesterolemia, smoking and drinking history Vertigo, slurred speech, right side numbness and weakness, unsteady gait, right hearing loss, right ataxia, right hemihypoestesia. left eye abduction dysfunction, and diplopia Infarction of MCP Angioplasty-stent placed, oral dual antiplatelet (acetylsalicylic acid and clopidogrel) Relief in right side weakness and dysarthria, nystagmus and dyskinesia recovered significantly 2 61/M Hypertension, hypercholesterolemia, smoking and drinking history, atrial fibrillation Vertigo, slurred speech, unsteady, standing instability, dysarthria, dysphagia, aspiration, bilateral hearing loss, and somnolence Infarction of MCP Angioplasty-stent placed, oral dual antiplatelet (acetylsalicylic acid and clopidogrel) Physical activity significantly improved, hearing was restored. Ataxia persisted 3 68/M Hypertension, hypercholesterolemia, diabetes Vertigo and severe ataxia, slurring of speech and unsteady gait, dysarthria, somnolence, hearing loss, unsteady gait, vomiting and nausea. bilateral horizontal nystagmus Infarction of MCP Oral dual antiplatelet (acetylsalicylic acid and clopidogrel) Slight improvement in dysarthria, but there were significant ataxia and bilateral deafness 4 51/M Hypertension, hypercholesterolemia, diabetes Vertigo, severe ataxia, slurring speech, unsteady gait, dysarthria, somnolence, hearing loss, bilateral horizontal nystagmus, ataxia of limbs and trunk Infarction of MCP Oral dual antiplatelet (acetylsalicylic acid and clopidogrel) Still had ataxia, slurred speech, and gait instability MCP - Middle Cerebellar Peduncles, M - Male
Year Number of cases Therapy Author + Reference 1991 1 — Tsukamoto T et al11 1994 1 — Ichikawa H et al12 1998 1 — Sato K et al13 1998 1 — Roquer J et al14 2000 1 — Akiyama K et al15 2001 1 Anticoagulation Lee H, et al16 2005 1 Oral antiplatelet Sunami E, et al17 2007 1 Anticoagulation Iwanami H, et al18 2009 3 — Lee H, et al2 2010 1 — Renard D et al19 2011 1 Intravenous ozagrel and oral ticlopidine Kataoka H et al6 2013 1 Dual antiplatelets (acetylsalicylic acid and clopidogrel) John S et al7 2013 1 Stent Kattah JC et al10 2016 1 Anti-platelet and symptomatic treatment Özkan A et al20 “—” means the treatment was not explicitly mentioned in the literature
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.