


Abstract
The prevalence of type 2 diabetes is rising worldwide, including Saudi Arabia. Among patients with diabetes, 30% suffer from mental disorders, such as depression, schizophrenia, delirium, and substance misuse (for example, tobacco smoking). Moreover, these disorders appear to share a bidirectional relationship with diabetes. For example, the incidence of diabetes has been shown to be 2-4 times greater in patients with schizophrenia than in normal individuals; also, there is a known association between depression and diabetes. In this review, we focus specifically on the bidirectional relationship between diabetes and psychiatric disorders, including the effects of antipsychotic drugs.
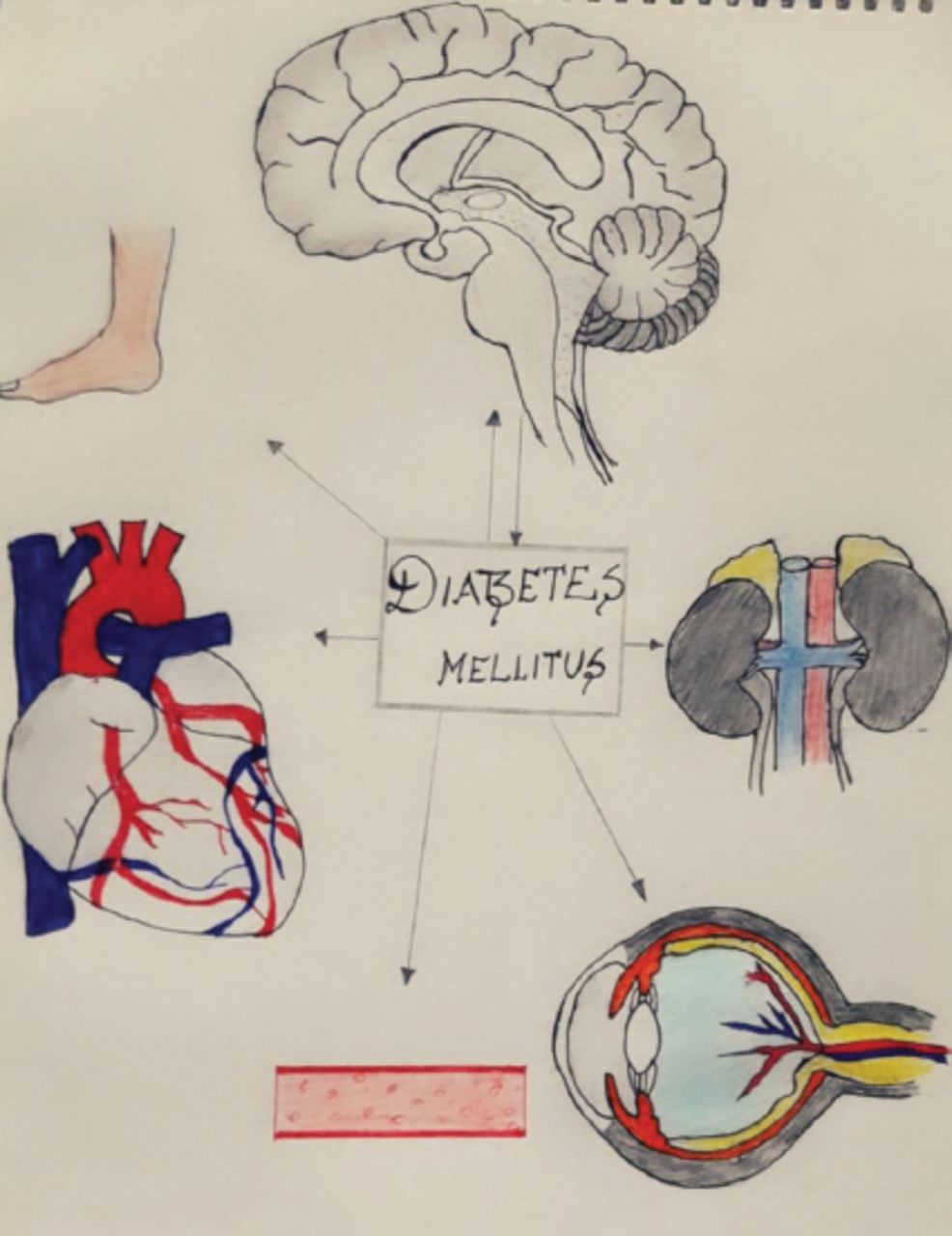
Advances in basic science and in investigative techniques result in constant changes in the knowledge about several disorders and their complex interactions. For example, currently psychiatrists recognize that many psychiatric disorders result from medical conditions, and vice versa. Indeed, the urgency of mental health issues may require that the psychiatrist becomes the primary physician treating the individual. This review highlights the common psychiatric morbidities that coexist with diabetes, and the role of psychiatrists in the diagnosis and management of patients suffering from concurrent mental and somatic disorders. (Figure 1)
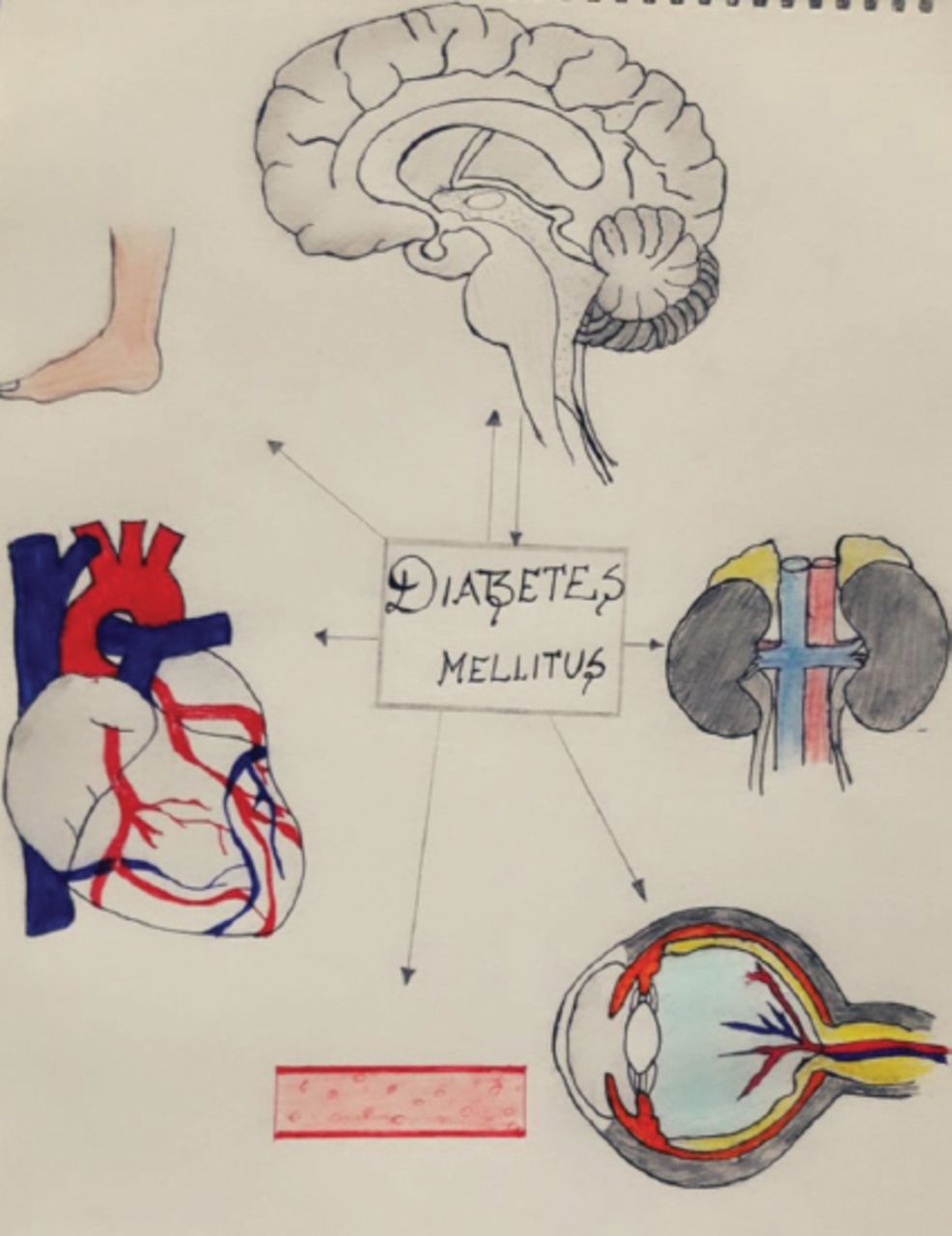
The effect of diabetes on kidney, eye, blood vessels, heart and foot is unidirectional, while its effect on Psychiatric illness could be bidirectional.
An overview has shown that there are no accurate data on the prevalence of mental illness in the Saudi Arabian population.1,2 Becker et al2 evaluated somatic symptom disorder and other mental disorders in a Saudi population and found that the prevalence of the bodily symptoms of mental depression in primary health care centers was similar to that reported in other parts of the developed world, making Saudi Arabia one of the 10 countries with the highest prevalence of diabetes.3 A study that screened school children in Saudi Arabia for mental illness revealed a prevalence rate as high as 48%. Furthermore, mental illness was more frequent in girls (51%) than in boys (41%); however, caution must be taken before making this generalization owing to the small study sample.4 In another study, the prevalence of depression, anxiety, and stress was evaluated in Saudi students and the results indicated that most students (59.4%) had at least one of these disorders, and many (40.7%) had 2 and almost one quarter of them (22.6%) had all the 3. It was also determined that 38.2% suffered from depression, 48.9% suffered from anxiety, and 35.5% suffered from stress, and all 3 conditions were significantly and positively correlated.5
Diabetes mellitus and depression
Diabetes is reaching epidemic levels, affecting not only the lives of entire families, but also causing severe healthcare-related economic burdens. The disease has been projected to reach 380 million cases worldwide by 2025, and 552 million by 2030.6 These figures exclude those suffering from undiagnosed diabetes, which accounts for an estimated 183 million people. In a cross-sectional study from a military hospital in Saudi Arabia, 30% of the hospital population had diabetes mellitus.7 A study from the Netherlands showed that patients with type 2 diabetes with complications such as diabetic neuropathy and diabetic nephropathy are at a higher risk of having depression, and emphasized the necessity of early detection and treatment.8 By contrast, there is little data on the incidence of coexisting psychiatric disorders in patients with diabetes in Saudi Arabia. Depression is a major cause of concern worldwide due to the associated morbidity. The incidence of depression is about 2 times higher among patients with type 1 and about 3 times higher among patients with type 2 diabetes than among normal individuals worldwide, adding to the concern is a majority of patients go undiagnosed.9
Diabetes mellitus is the most common endocrinal disorder with metabolic effects, and is associated with predisposing factors, including genetics, a sedentary life style, age, and increased body mass. Similarly, mood and psychotic disorders also have genetic predispositions and are associated with obesity and sedentary lifestyles. The prevalence of co-morbid type 2 diabetes and mood disorders is on the rise, and both diseases are considered multi-factorial. Anderson et al10 and Grigsby et al11 have shown that depression and anxiety are commonly associated with diabetes in the general population, and that depression is more prevalent in women than in men. It is the author’s contention that 3 possibilities exist: 1) diabetes and psychiatric disorders can manifest as independent diseases with no interaction; 2) diabetes and psychiatric disorders are comorbidities that coexist and can negatively affect each other; and 3) psychiatric disorders are risk factors for diabetes mellitus. (Table 1)
Interrelationship between diabetes mellitus and depression.
In the first of these possibilities, the disorders have an entirely independent etiopathogenesis and occurrence. In the second possibility, however, diabetes mellitus and psychiatric disorders exist as comorbidities that follow independent but parallel pathways. For example, poor glycemic control may increase diabetes-related complications and affect a comorbid psychiatric disorder.12,13 Various biological and psychological factors mediate the process of development of psychiatric problems in a patient known to have diabetes. In the third possibility, psychiatric disorders such as depression and schizophrenia may act as significant independent risk factors for diabetes.
Depression is becoming increasingly common worldwide. It is characterized by persistent low moods and is associated with multiple risk factors. The World Health Organization speculates that by 2020, depression will be the second most common factor for disability. The prevalence in primary care is reportedly 15-22%, with a global prevalence of approximately 13%. In Saudi Arabia, the reported prevalence of depression varies widely from 17-46%; however, it is also reported that primary care physicians can miss the diagnosis in 30-50% of cases.14
The prevalence rates of depression and anxiety among diabetics are known to be higher than those in normal individuals, with a staggering 50-100% increased risk of depression among patients with diabetes.15 The prevalence of diabetes in depressed adult patients is much higher in women than in men.16 A study performed by Golden et al17 also identified a bidirectional adverse relationship between diabetes and depression. Over a 3-year follow-up period, the depressive symptoms in patients correlated with an increased risk for diabetes. In contrast, they found that patients with uncontrolled fasting blood glucose levels and patients with type 2 diabetes not under treatment had less chances of having depressive symptoms. It is known that patients suffering from depression often fail to follow medical advice about medication and diet, and this can ultimately lead to glucose dysregulation and diabetic complications. In contrast, another independent mechanism for glucose dysregulation in patients suffering from depression is via the neurohormonal route. Depression activates neurohormonal and neurotransmitter changes that stimulate the hypothalamic-pituitary-adrenal axis, thereby increasing the release of cortisol and other hormones responsible for insulin resistance. This can decrease glucose uptake and interfere with glucose metabolism. Comorbid diabetes and depression certainly lead to a decreased quality of life, increased treatment costs, more complications, and higher mortality rates.
Gemeay et al18 studied the frequency of depression among Saudi patients, and established a correlation between the level of depression and diabetes. Their study established that 37% of type 1, 37.9% of type 2, and 13.6% of gestational diabetic patients had depression. In addition, Das et al19 correlated the depressive symptoms in patients known to have diabetes with the HbA1C levels and quality of life. They found that 46.15% of the diabetic patients in their study had depression, and among this group 36.7% had a moderate level of depression. The average level of HbA1C was higher among patients with depression than among the non-depressed group. These authors concluded that the presence of depression in patients with type 2 diabetes mellitus was associated with an impaired quality of life.
Mansour et al20 studied the effects of counseling on patients with depression and diabetes. Initially, depression was present in approximately 57.5% of the control group, and among the patients who underwent counseling, 32.5% had severe depression. However, by the second assessment, the rate of depression increased to 67.5% in the control group, while the rate of severe depression decreased to 25% in the counseling group. Thus, counseling was helpful in reducing the level of depression.
Diabetes mellitus and schizophrenia
In a cross-sectional study, patients with schizophrenia were shown to be at increased risk of developing diabetes, indicating schizophrenia as an independent risk factor for diabetes.21 A Danish study also showed that not only did schizophrenia increase the risk for diabetes, but this risk was further increased by first- and second-generation antipsychotic drug use. They suggested the need for early detection and treatment of diabetes, with multidisciplinary care for schizophrenia, irrespective of antipsychotic drug exposure.12 Although it remains unproved whether schizophrenia could be a predisposing factor for diabetes mellitus, many studies have suggested that impaired fasting glucose and insulin resistance occurs in 10% to 15% of patients with schizophrenia, almost 4 times more frequently than in normal individuals.22-25
Diabetes is frequently associated with cognitive impairment, and in patients with schizophrenia the presence of cognitive deficits has been identified as an important index of functional and treatment outcomes.26,27 Han et al28 reported that schizophrenia concurrent with diabetes was associated with a greater degree of cognitive impairment than schizophrenia alone or diabetes alone. A study in Singapore, among 194 schizophrenic patients, 16% had diabetes and 30.9% had impaired glucose tolerance. The mean age of the participants in this study was 55.5 years, which suggests that the coexistence of the 2 disorders may be associated with age. It was also suggested that this association places patients with schizophrenia at increased risk of coronary artery disease, hypertension, and ultimately, death. It is therefore recommended that clinicians be vigilant for early symptoms of diabetes mellitus, and that regular glucose monitoring be considered mandatory.29
The association between diabetes and schizophrenia has been known for a long time, but the incidence of diabetes mellitus has increased significantly since the introduction of antipsychotics for schizophrenia. This increased risk is thought to result from a combination of genetic and environmental factors, such as a low level of physical activity, poor diet, neglected health care, and use of antipsychotic medication. While these are all undoubtedly important risk factors for diabetes that are inherent to having schizophrenia; the diagnosis of schizophrenia itself may also be an independent risk factor. Furthermore, schizophrenia may be associated with treatment non-adherence, which has a significant impact on disease management.30 (Table 2)
Interrelationship between Schizophrenia and diabetes mellitus.
Interestingly, among the first-degree progeny of patients with schizophrenia, there is a higher prevalence of diabetes, and those with a family history of diabetes mellitus have been shown to be at a higher risk of developing schizophrenia. Thus, clinicians should be aware that patients suffering from both schizophrenia and diabetes have an increased risk of depression and can have an associated cognitive impairment, increasing the chances of hospitalization. The rate of identifying psychiatric problems in patients with diabetes is quite low, with as much as 45% of such disorders going undetected.31
Antipsychotic medications and hyperglycemia
Database analysis has suggested that all antipsychotic drugs (Table 3) can be a factor for higher blood sugar levels, and that if persistent, may lead to type 2 diabetes. Antipsychotics may also lead to metabolic acidosis, ketoacidosis, or rarely, hyperglycemia-related deaths. However, the risk of antipsychotics causing diabetes is variable.30 Many comparative studies have shown that olanzapine and clozapine have a higher incidence of associated diabetes than quetiapine.32 There is evidence that strongly suggests that antipsychotic treatment creates a higher risk for developing diabetes as compared to individuals who do not take antipsychotics. Atypical antipsychotics have been shown to affect glucose sensitivity and to induce insulin resistance after only a single dose. The waist-to-hip ratio appears to be the most strongly associated risk factor for diabetes in these patients.33-35 Antipsychotics affect the control of the hypothalamus on serum glucose via dopamine antagonism. Treatment with clozapine is associated with higher serum insulin levels compared with conventional medicines.
Commonly prescribed antipsychotic drugs.
Schizophrenia is often associated with metabolic abnormalities, and recent second-generation atypical psychotropics have been shown to increase the risk of diabetes mellitus 4-fold.36 These drugs have different potentials for causing metabolic changes, hyperglycemia, and weight gain. Although the exact mechanism underlying the weight gain associated with these drugs is not known, it has been attributed to their strong antihistamine activity, probably through antagonism of the 5-HT2C receptors.37
Risperidone and olanzapine are commonly used antipsychotics in Saudi Arabia, and both have been shown to cause weight gain and diabetes. Notably, diabetes is more common with olanzapine therapy, while glycemic states are more common with risperidone therapy.38 Thus, atypical antipsychotics differ in their metabolic actions and there is a need for a thorough evaluation of each patient before starting therapy. However, patients may not follow the doctor’s advice, and in these cases, diabetic ketoacidosis and other complications are not uncommon. Thus, the resulting poor glycemic control may lead to a reduced quality of life, more hospital admissions, and increased treatment costs.
To limit the risk of hyperglycemia in patients receiving antipsychotics, the author recommends a protocol that categorizes patients into the following 3 groups:
Group I: Patients recently diagnosed with a psychiatric disorder
For patients who have never received psychotropic or atypical antipsychotics drugs, initial blood tests for glycated hemoglobin, fasting blood sugar, and random blood sugar, as well as recording the initial waist circumference and weight, are recommended. All blood tests and measurements should then be repeated after 4 months.
Group II: Patients already receiving atypical antipsychotics
In these patients, a blood test for glycated hemoglobin, plus measurements of waist circumference and weight are recommended. Medication can be continued in those patients who have results that are within the normal range or that do not change significantly over time.
Group III: Patients with diabetes who are receiving atypical antipsychotics
It is recommended that regular evaluation of glycated hemoglobin levels, and weight and waist circumference measurements are performed every 3 months. Treatment should be continued or changed in consultation with an endocrinologist.
Delirium and diabetes mellitus
Delirium is a syndrome of altered consciousness that is characterized by an acute onset of cognitive change and attention deficit and follows a fluctuating course. In diabetes, delirium could be a late manifestation of acute hypoglycemia due to diabetic ketoacidosis.30 Patients with diabetes and comorbid psychiatric disorders are more prone to hypoglycemic delirium, which may present with hypoactivity or hyperactivity. A hyperactive patient will present in a very excited state and will move around aimlessly. By contrast, a hypoactive patient will present with reduced psychomotor activity and apparent calmness. However, confusion, disorientation, and hallucinations are present in both forms, and early detection is crucial to the outcomes.
Smoking and diabetes mellitus
Tobacco smoking is estimated to be 2-5 times more common in individuals with psychiatric illnesses, including schizophrenia, mood disorders, anxiety, eating disorders, and attention deficit and hyperactivity disorder.39,40 There is sufficient evidence to prove that smoking could be a modifiable factor for the development of diabetes and has a clear dose-response relationship. Early smoking cessation can decrease the chances of developing diabetes, and later cessation has been shown to improve blood sugar levels and limit the harmful effects on vital structures. There is only weak evidence to suggest that smokeless tobacco usage is associated with a higher risk of developing diabetes.41 Every patient attending a psychiatry clinic should be asked about tobacco use, especially adolescents and those with diabetes. It is also worth noting that a significant number of patients start tobacco use after being diagnosed with diabetes, and that efforts should be made to educate patients before this happens.42,43
In conclusion, every patient suffering from a psychiatric disorder should undergo systematic screening for diabetes (and vice versa) because of the inter-relationship of the psychopathological symptoms between the 2 conditions. Current evidence shows that diabetes mellitus, depression, and schizophrenia are significantly associated with one another. In addition, depression and schizophrenia are common comorbidities in patients with diabetes, indicating the need to screen patients with diabetes for these conditions and to provide early referral for psychiatric care and psychosocial support. A simple and effective means of screening for depression is asking the patient about the presence of a persistent depressed mood before evaluation with a formal mood questionnaire, if warranted.
Furthermore, diabetes mellitus and psychiatric disorders are not only more likely to occur in the presence of each other, but also have potential causal relationships. Atypical antipsychotics, chiefly olanzapine and clozapine, and, to a lesser extent, risperidone, can cause a metabolic syndrome that can lead to diabetes. It is therefore advised that patients on such medication be monitored at regular intervals to ensure early diagnosis and optimal glycemic control. Ziprasidone and sertindole do not induce diabetes and may be more suitable alternatives in high-risk populations.
This review article clearly emphasizes to the medical fraternity in general, and psychiatry in particular, the necessity of a holistic treatment approach aiming for the total wellbeing of the patient, including physical, mental, and emotional dimensions.
Acknowledgment
The author would like to thank Editage for the English language review and Ms. Reshma V.K for the drawing of figure 1.
Footnotes
Disclosure. Author has no conflict of interests, and the work was not supported or funded by any drug company.
- Received February 28, 2017.
- Accepted December 13, 2017.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.