


Abstract
Brain abscess is a potentially life-threatening condition requiring rapid diagnosis and prompt medical and surgical intervention. Various etiological agents associated with different epidemiological backgrounds are implicated, including Gram-positive and Gram- negative bacterial agents as well as anaerobes. Salmonella is rarely reported to be the cause of this medical condition despite being known to cause invasive infections at extremes of age and the fact that this organism is a common cause of other clinical infectious diseases encountered in immunocompromised and immunocompetent individuals. A case of Salmonella brain abscess involving the right posterior parietal region of the brain is described in a 6-month-old infant. The clinical, microbiological, and radiological features, as well as the clinical management and outcome, are presented. This case highlights the slow-progression nature of brain abscess caused by Salmonella species and the challenge in achieving optimal resolution despite initial surgical intervention.
Despite the fact that bacteremia, sepsis, and meningitis are relatively common in infants, episodes of focal intracranial infection produced by Salmonella are rare. Torrey et al1 reported an incidence of up to 6% bacteremia in infants under 12 months old with salmonellosis, and Rocha described a 1.3% rate of meningitis in children under 18 months with this disease. Cerebral abscesses and other focal intracranial infections due to Salmonella such as subdural and epidural empyema are rarely reported in the literature with only 80 cases reported. In these infections, Salmonella typhi is the most frequently isolated causative agent.1
Case Report
Patient information
A 6-month-old male infant was admitted in the pediatric surgical ward in Khawla Hospital, Muscat, Sultanate of Oman in November 2014 with a history of 2 weeks of fever associated with 2 episodes of focal tonic-clonic convulsions. The child had a history of 2 weeks of fever with temperature of 38.3°C, which was mild and intermittent initially, progressing to high-grade continuous fever not responding to antipyretics. The child later developed 2 episodes of left-sided focal tonic-clonic convulsions of 2 minutes’ duration. This febrile illness was preceded by a history of diarrhea of one days’ duration with passage of non-bloody, loose, watery motion more than 4 times per day and associated with vomiting; no other household member had diarrheal illness during that period. The child was on bottle feeding. There was no history of urinary incontinence, respiratory symptoms, or otorrhea. There was no past history of convulsions, prolonged fever, or traumatic injury.
Further history inquiry revealed that the child had been admitted 3 months earlier in a local hospital with clinical impression of meningitis as he presented with 2 days’ history of fever and bulging fontanel. Computed tomography (CT) scan showed findings suggestive of meningitis: lax brain/subdural effusion at both convexities (maximum-10). Lumbar puncture was refused by the family at that time, and blood culture taken on the day of admission grew Salmonella. The child was treated with Ceftriaxone for 14 days and then discharged home. The child had been asymptomatic until he presented 3 months later (November) with fever and convulsions as described above.
The infant is a baby of a primi mother, with no family history of seizure disorders. The infant was immunized as per the national immunization schedule and had attained milestones as per the age.
The baby has been on bottle feed since age of one month. He was also started on yogurt and preserved canned grain and fruits since age of 4 months. The mother and the child are not known to have HIV or any risk factors for blood-borne diseases.
Clinical findings
Clinical examination revealed a febrile baby with a temperature of 38.3°C. He was stable hemodynamically. His anterior fontanel was about 1.5×2 cm and non-bulging, and his posterior fontanel was closed. No abnormality was found on general and systemic examination, including examination of the central nervous system and ENT.
Diagnostic assessment
Investigations were carried out on admission revealed hemoglobin (Hb) 8.3 g/dl (11.5-14.5), mean corpuscular volume=64.42 fl (78-92), mean corpuscular hemoglobin=21.41 pg (27-32), platelet count=896.40 103/ul (150-400), white blood cells of 18.73 103/ul (4.5-18), differential leucocyte count was neutrophils 9.47 103/ul (1.5-6.5), Lymphocytes 7.16 103/ul (3-10), Monocytes 1.71 103/ul (0.3-1.2), and erythrocyte sedimentation rate (ESR) was 133 mm in the first hour, C-reactive protein was 104.91 mg/l (0-5), blood culture was bacteriologically sterile. Sickling test was negative.
Therapeutic intervention
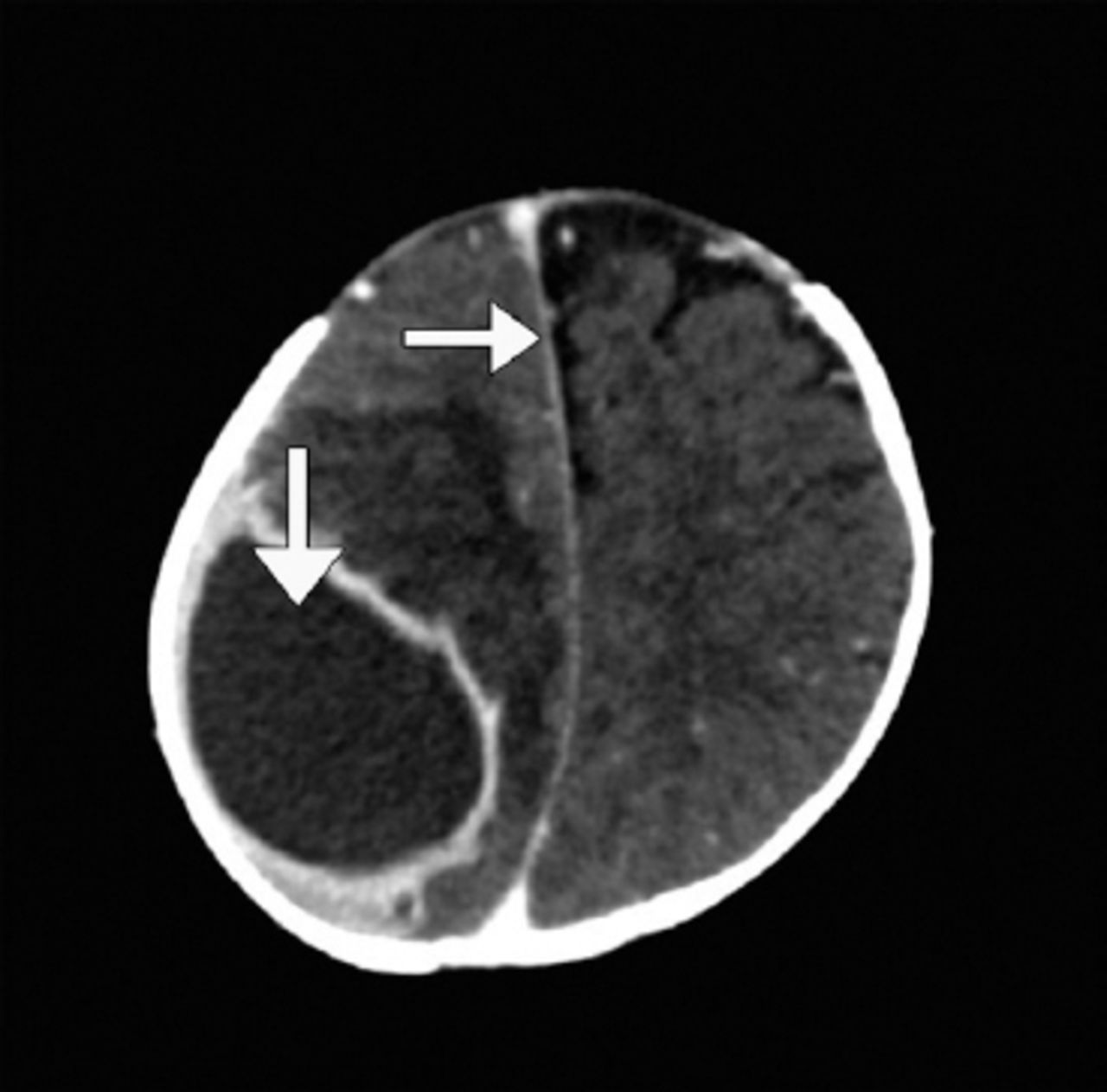
The child underwent an urgent neurosurgical procedure under general anesthesia, during which a right parietal burr hole was created (Figure 1). After opening the dura with a cruciate incision, the brain surface was coagulated with bipolar diathermy. Tapping of the abscess revealed foul-smelling pus, which was sent to the microbiology laboratory for culture and sensitivity. Bacterial cultures grew non-lactose fermenting colonies identified by conventional biochemical reactions and API20E (bioMérieux) by Pheonyx (Becton Dekinson) as Salmonella species. It was further confirmed by slide salmonella antigen agglutination test as Salmonella L. Stool culture was performed on day 8 of Ceftriaxone and was negative for Salmonella spp. Anerobic and mycobacterial cultures of the pus yielded no growth.
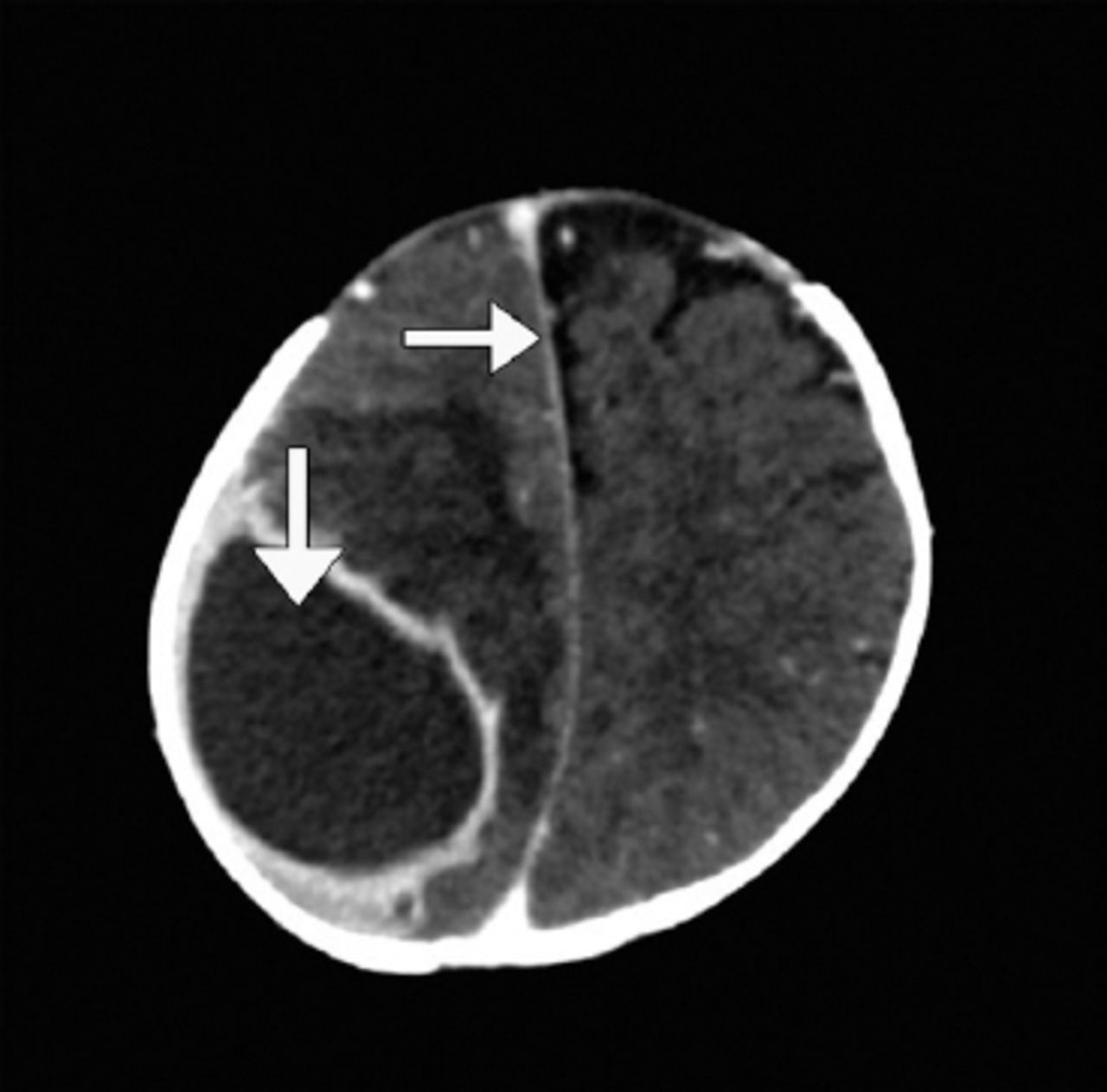
Computed tomography (CT) scan of the brain showed a large, 6x4x3.7 cm hypodense area likely extra axial location in the right high posterior parietal region with enhancing wall suggestive of empyema/abscess with mass effect and displacement and compression of ipsilateral right frontal horn and mild dilatation of left frontal and right temporal horn of lateral ventricle and midline shift to the left by 8-9mm. There is reduced density of a large area of the underlying right posterior frontal and parietal brain regions, likely edema.
Antimicrobial susceptibility testing was carried out as per the clinical and laboratory standards institute (CLSI) 2014 by disk diffusion as well as microdilution for MIC determination (Pheonyx, Becton Dekinson). The organism was found to be sensitive to ampicillin, ceftriaxone, co-trimoxazole, chloramphenicol, and ciprofloxacin.
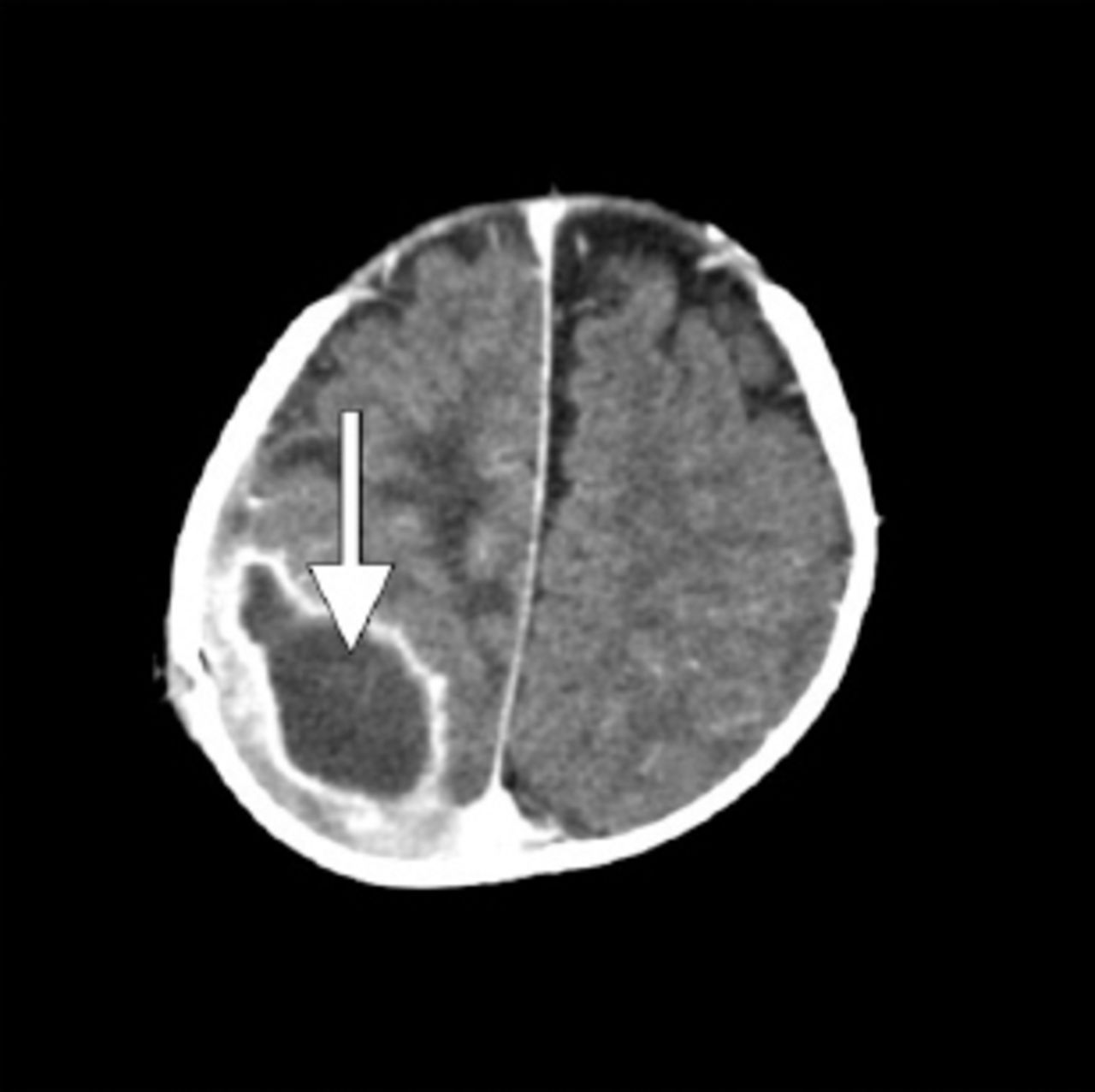
The patient was treated with aspiration of the abscess after a burr-hole placement (Figure 2), along with antibiotic therapy consisting of ceftriaxone (50 mg/kg - 12 hourly).
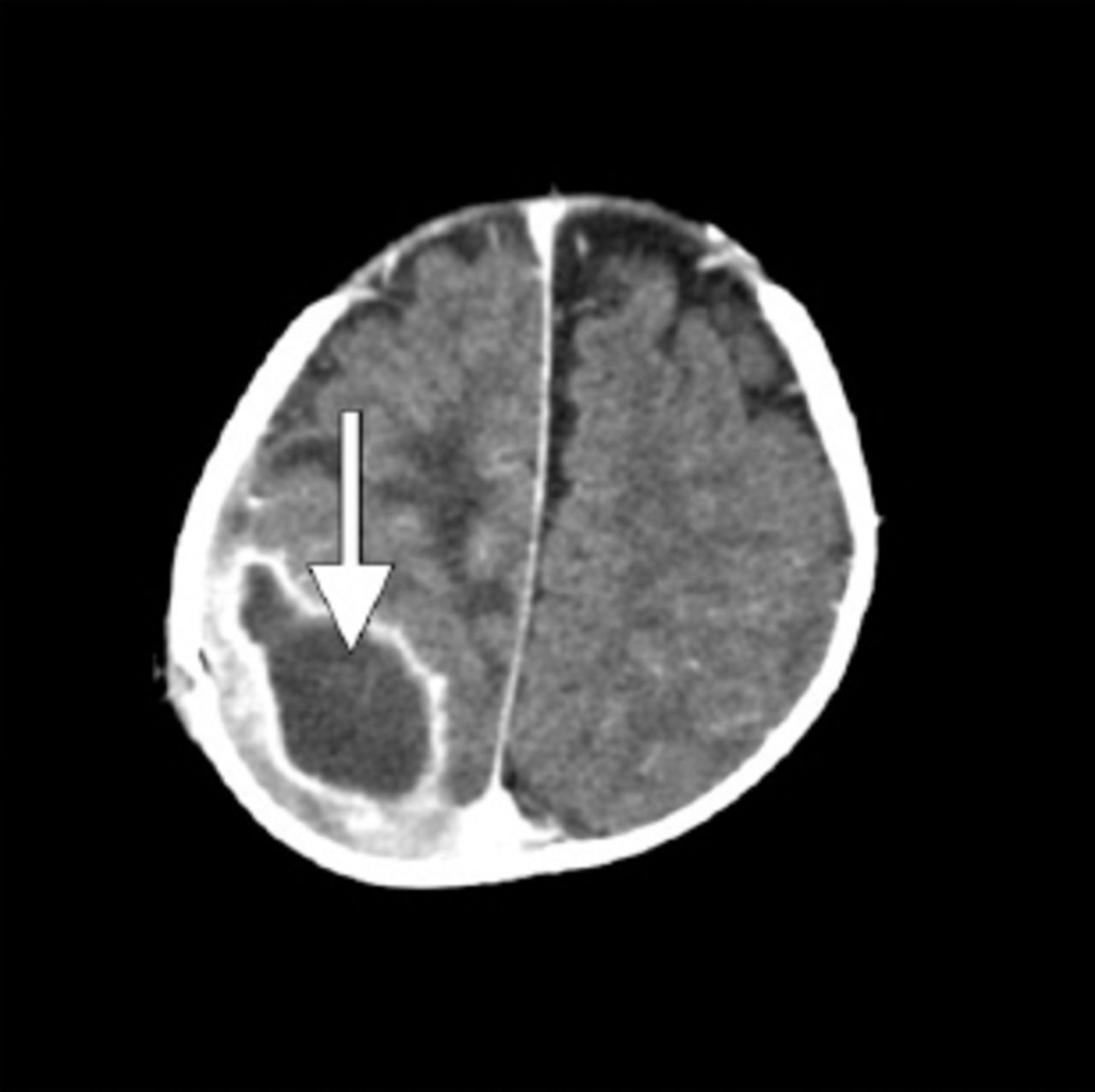
Computed tomography (CT) was repeated 2 weeks post operation.
Follow up and outcome
The child made a dramatic clinical response with immediate improvement of fever, and convulsions were not recorded or observed during the rest of the hospital stay. The child’s total white cell count, as well as inflammatory markers, normalized following surgical drainage of the abscess and commencement of antibiotic therapy. A plan for prolonged intravenous antibiotic treatment as well as re-evacuation and irrigation was made, but the parents decided to take the patient abroad for a second opinion. The full details of management of the case abroad are not available, as the patient did not show up for follow-up after he came back. However, the baby was well at home as per the parents, who were contacted via phone calls 6 and 8 months later. Table 1 summarizes the patient progress on a timely manner from the day of admission until discharged.
Summarizes the patient progress on a timely manner from the day of admission until discharged.
Discussion
The genus Salmonella belongs to the family of Enterobacteraceae. They can be broadly categorized as typhoidal or non-typhoidal (NTS) Salmonella depending on the clinical syndrome with which they are predominantly associated. The NTS are predominantly food-borne pathogens acquired from both animals and humans, and transmission primarily induces acute, self-limiting gastroenteritis.2 While poultry and eggs remain the most common source of NTS, other animal reservoirs include reptiles, rodents, cats, and dogs.2
The NTS pathogens are known to cause invasive infections in patients with HIV, Sickle cell disease, hematological malignancy, or immunosuppression, as well as in individuals at extremes of age. Infants are at high risk of severe infections, which may present as bacteremia, bone and joint infection, and meningitis, according to Siriven et al.4,5 Such extra-intestinal manifestations are occasionally preceded by gastrointestinal illness, as seen with our case.3
The case presented showed slow disease progression over a few months. Although reinfection or relapse (from inadequate treatment) could have other causes for such a prolonged course, long duration of fever with slowly progressive illness is not uncommon with Salmonella subdural empyema. Kai-Mao Chen 3 reviewed the clinical presentation and laboratory findings of cases with Salmonella subdural empyema in 17 children. Fever (17/17; 100%), symptoms and signs of increased intracranial pressure (8/17; 47%), seizures (8/17; 47%), and limb paralysis (8/17; 47%) were the most frequent clinical features. In 11 out of 17 of those cases (65%), the causative organism was not known before surgical intervention, while 5 (29%) of them had prolonged fever for more than 3 weeks; this leads to the conclusion that a slow disease progression may be seen with subdural empyema due to Salmonella species.
Although objective clinical assessment following treatment could not be done, this reported case has had a favorable outcome after 6 and 8 months following clinical presentation. Treatment consisted of prolonged intravenous antibiotic treatment as well as surgical intervention. The requirement for surgical intervention is common in this disease and can be up to 94%.3 Morbidity is reported to be high as well, with a 29% morbidity rate reported by Kai-Mao Chen.3
In summary, we report a case of brain abscess caused by Salmonella species in an infant who was initially presented with gastroenteritis, bacteremia, and meningitis. The disease manifested with slow progression and neurological complications that necessitated neurosurgical interventions and prolonged course of antibiotic treatment with a final favorable outcome.
Footnotes
Disclosure. The authors declare no conflict of interests, support or funding from any drug company.
- Received March 30, 2017.
- Accepted March 7, 2018.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.