


Abstract
Neuro-behçet’s disease (NBD) is an uncommon, serious presentation of behçet’s disease (BD) causing long-term morbidity and mortality. Cerebral aneurysms are rare in BD, with only a handful of cases reported worldwide. A 39-year-old female experienced slurring of speech, numbness, and reduced sensation in the left face, arm, and leg 90 minutes prior to presentation. She provided a history of recurrent oral and genital ulcers associated with intermittent joints pain and blurring of vision. erythrocyte sedimentation rate was elevated, but all other autoimmune workup was negative. Neuro-behçet’s disease was diagnosed. Brain magnetic resonance imaging demonstrated acute right periventricular infarction. Magnetic resonance angiogram revealed M1 segment stenosis and right internal carotid artery saccular aneurysm. Catheter angiography confirmed its presence measuring 4.8 mm×6.1 mm. She was stabilized after coiling of the aneurysm and was started on medical therapy. Brain imaging should be carried out in young patients with BD presenting with an ischemic event, and intervention may be lifesaving.
Behçet’s disease is a recurrent multisystem vascular inflammatory disease of unknown etiology.1 The diagnosis is based mainly on clinical symptoms and signs of the International study group criteria.2 Neuro-behçet’s disease is a relatively uncommon neurological manifestation of this disease. It may be the first symptom in approximately 3% of cases.1,3 Cerebrovascular accidents (CVA) and aneurysms due to NBD are very rare and are potentially life threatening.3 We report a rare case of NBD in a 39-year-old female presenting with a stroke and cerebral aneurysm.
Case Report
Patient’s information
We present a 39-year-old Saudi female who is known to have uncontrolled hypertension and bronchial asthma.
Clinical findings
She presented with the chief complaint of slurring of speech and numbness on the left side of the face, left upper limb, and leg upon waking that lasted for 90 minutes. No other neurological symptoms were reported. She had a history of recurrent oral (4 times) and genital ulcers (2 times) associated with intermittent joints pain and blurring of vision. There was no history suggestive of ophthalmic symptoms. Her family history was unremarkable. She was not a smoker. She was not taking any medications prior to presentation. She denied allergies to drugs or food.
On examination, her blood pressure was 188/100 mmHg with pulse rate of 76 bpm. She was alert and oriented to time, place, and person (language comprehensive and coherent). Her cranial nerves were intact. Her motor system was normal. She had decreased sensation to pain and temperature on the left side of body involving face, arm, and leg. Her cerebellar function and gait were normal. Her systemic examination did not reveal significant findings.
Diagnostic assessment
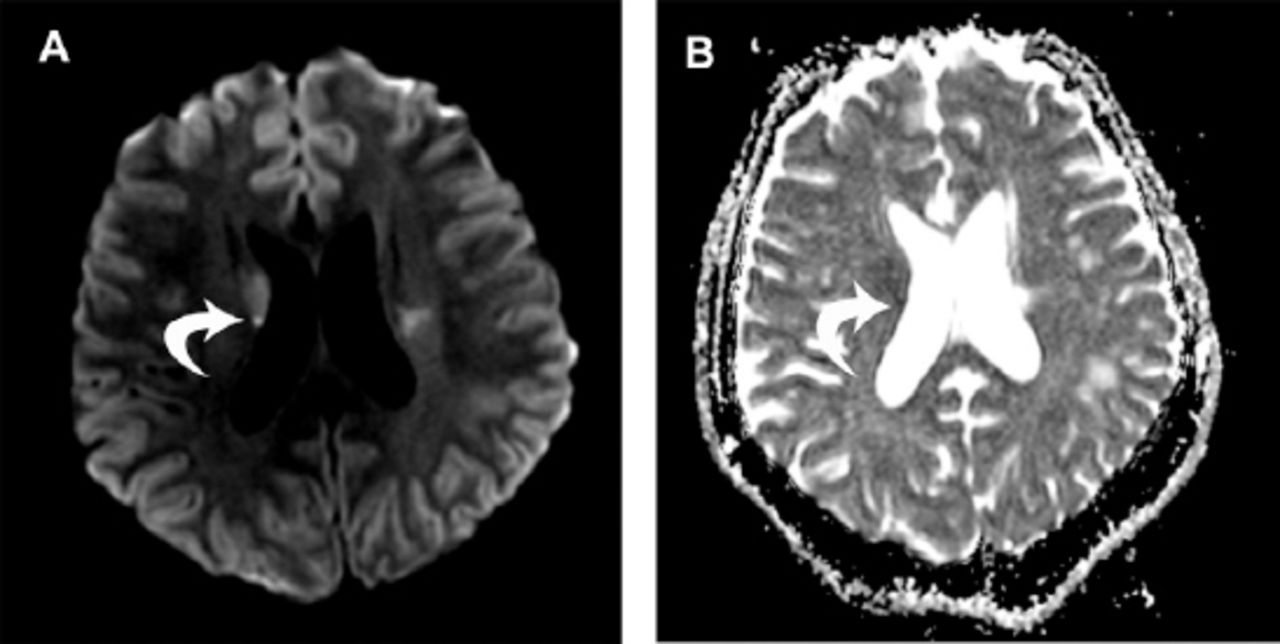
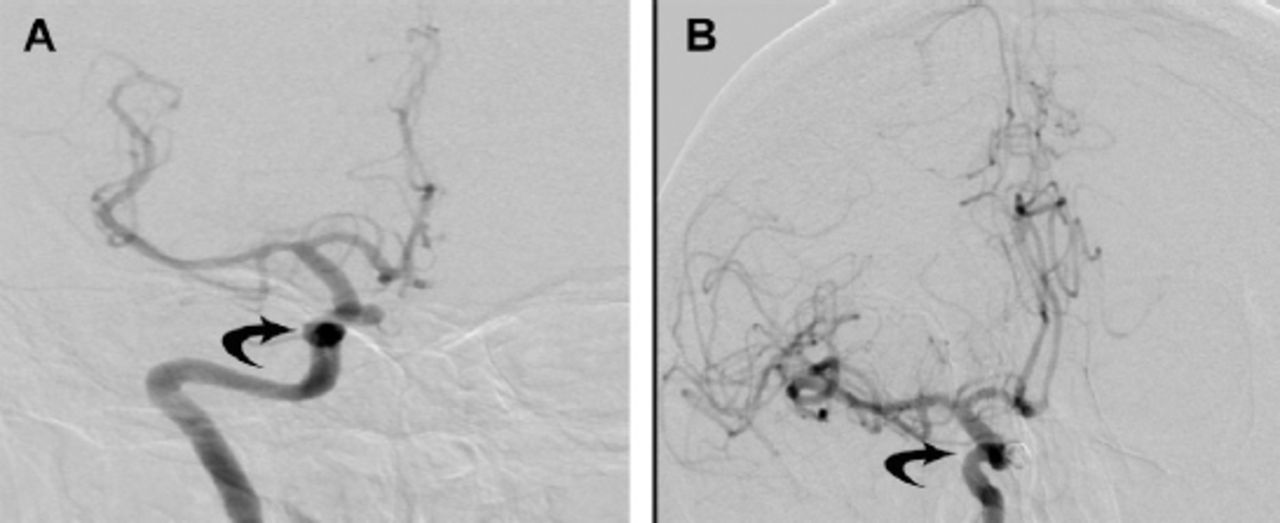
She was admitted for further workup and management. Her routine blood workup was within normal limits. Brain imaging with MRI was performed which demonstrated an acute infarction involving the right periventricular area. (Figure 1) Magnetic resonance angiogram revealed a stenosis of M1 segment of the right middle cerebral artery (MCA) and a saccular aneurysm of the cavernous portion of the right internal carotid artery (ICA). Due to aforementioned findings, catheter angiography was carried out for her, and it confirmed the presence of saccular aneurysm measuring 4.8 mm×6.1 mm projecting medially from the cavernous portion of right ICA. (Figure 2)
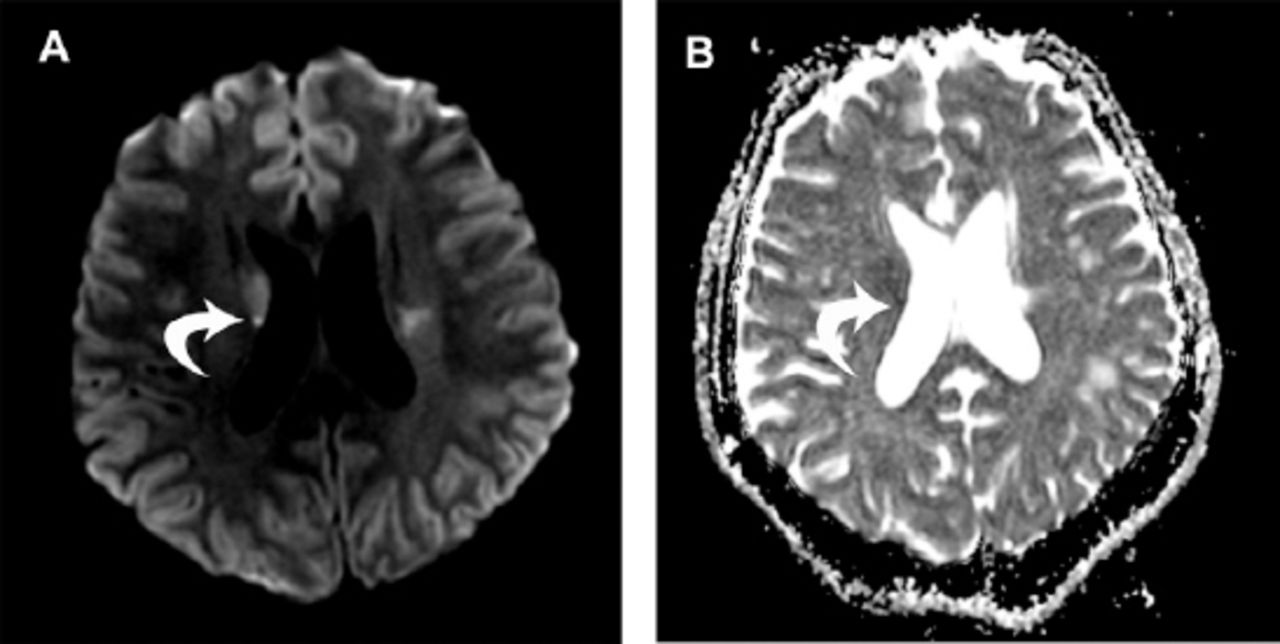
Diffusion weighted imaging. A) showing hyperintense lesion involving right periventricular area with corresponding hypointense lesion on adjusted diffusion co-efficient sequence. B) suggestive of acute infarction of this area.
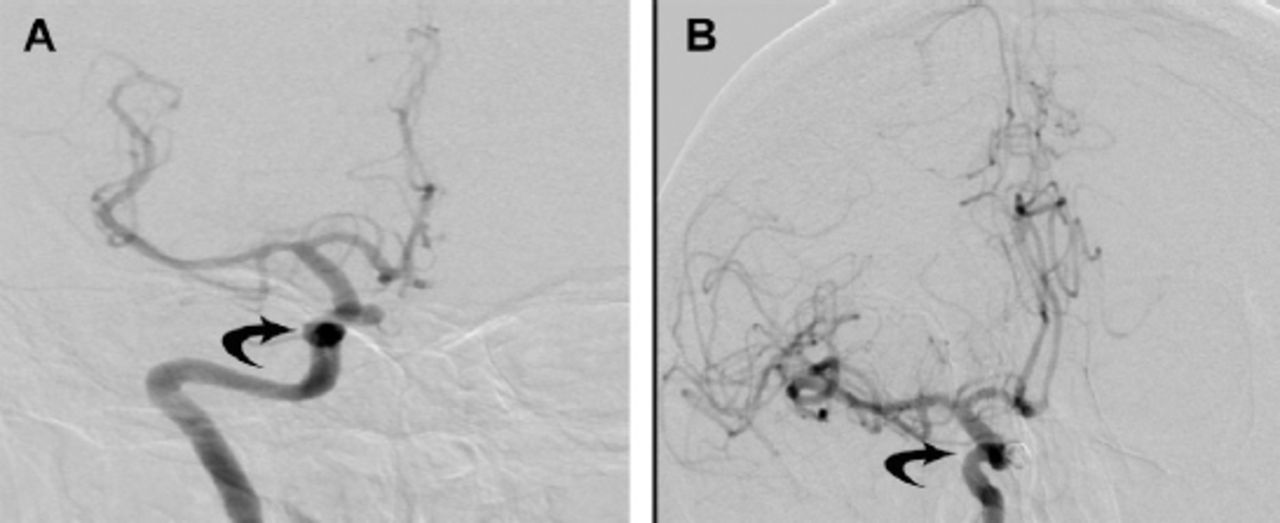
Catheter angiogram of right ICA. A) pre-coiling showing aneurysm involving the cavernous portion of right ICA. B) post-coiling angiogram showing complete obliteration of right ICA aneurysm with coils visible inside aneurysm.
Her stroke workup showed cholesterol of 253 mg/dl, triglyceride 165mg/dl, High-density lipoproteins (HDL) 42mg/dl, and Low-density lipoprotein (LDL) 173mg/dl. Her hemoglobin A1c was 6.2%. Her transthoracic as well as transesophageal echocardiogram were unremarkable. Her erythrocyte sedimentation rate (ESR) was 69mm/hr, but all her autoimmune workup was negative. The computed tomography (CT) scan of her chest was unremarkable as well.
Therapeutic intervention
Thus, the diagnosis of NBD was presumed on the basis of her history. She was started on aspirin and clopidogrel, and her risk factors were controlled for secondary prevention of stroke. She underwent coiling of the right ICA aneurysm. She remained stable after the procedure, and she was discharged with advice to follow-up in clinic.
Follow-up and outcomes
She was started on azathioprine, and she did not report any symptoms recurrence or new neurologic symptoms on follow-up visits up to 8 months (Table 1).
The patient’s progress summarized in a timely manner from day of admission until discharge.
Discussion
Our patient demonstrated stroke and cerebral aneurysm that might be the initial presentation of patients with BD, and imaging of brain vasculature should be considered as an essential workup for stroke in young people. The diagnosis of NBD is difficult in the absence of other criteria for BD. Thus, the diagnosis of NBD in our case was established based on the history of oral and genital ulcers (which were not present at the time of presentation), the presence of stroke-like episodes, the presence of a cerebral aneurysm, and the absence of other possible underlying causes.
Neuro-behçet’s disease is one of the most serious presentations of BD and one of the most important causes of long-term morbidity and mortality.2,3 Shahien R et al,2 reported that the incidence of NBD is very variable, as it is to be 18% (range 4%-49%), but Tursen U et al,4 reported that it can also be as low as 1.3%. Cerebral aneurysms are very rare in BD, and its incidence and prevalence have not been well documented in the literature. Although the vasculitis is theorized as the typical pathogenesis in arterial involvement, its underlying mechanism in developing cerebral aneurysms is uncertain to this day.3 One study reported by Benamour et al,5 demonstrated only one case from 316 cases of BD that was identified as having a cerebral aneurysm. MRA is the most sensitive non-invasive method to screen for cerebral aneurysms, and cerebral angiogram and it remains as the gold standard.6
Table 2 summarizes 25 cases of NBD with cerebral aneurysms previously reported in the literature. Eighteen (75%) of the cases with NBD and cerebral aneurysm were related to those of the male gender, and the mean age of diagnosis of the aneurysm was 41.7 years of age, with ages ranging from 12-65. The majority of patients in these cases were reported to be of a Turkish descent with 8 patients, followed by Japan with 7 cases, then Tunisia and Morocco with 2 cases each. Patients of Saudi Arabian, Indian, Korean, Caucasian, and Armenian descent were reported with one case each. When it came to the clinical manifestation, the majority of the patients 11 (44%) presented with subarachnoid hemorrhage (SAH), and cerebrovascular disease was present in 4 (16%) of patients. Our case presented with with paresthesia alone. The aneurysm was unruptured in 3 (12%) of patients and were most commonly located on the MCA. In our patient, the aneurysm was in the cavernous portion of right ICA. The aneurysm treatment in these 25 patients was mainly by coiling and clipping, which was composed of 8 (32%) patients each. No management was seen in 5 (20%) of the patients. There was a single case of Craniectomy, a single case of excision and grafting of the aneurysm, and a single case of embolization.
Summary of 25 cases of neuro-behçet’s disease with cerebral aneurysms.
With the aneurysm in our case being a superior hypophyseal aneurysm and being saccular with a small projection, its size increased the risk of subarachnoid hemorrhage (SAH) and mandated coiling of aneurysm. There are currently no guidelines on approaching such patients as well as the benefits of early intervention. The treatment of the reported cases ranged from conservative observation, medical, and surgical treatment in the form of open microsurgery and endovascular treatment. This is a topic that needs to be studied further. However, when approaching cerebral aneurysms in NBD, the state of the aneurysm (ruptured or not), the size, and location should be kept in mind.7 The use of adjuvant immunosuppressive therapy and steroids has also been reported, but there is a lack of consistency.8 The prognosis of ruptured intracranial aneurysms in patients with NBD remains unclear and is likely influenced by the severity of the hemorrhage and the course of the disease.
In conclusion, NBD presenting with a cerebral aneurysm is very rare and potentially life threatening. we believe such cases are often underdiagnosed and not reported. A high index of suspicion should be raised, and imaging of brain vasculature should be carried out in young patients with BD presenting with an ischemic event, and intervention may be potentially lifesaving in such patients.
Footnotes
Disclosure. The authors declare no conflicting interests, support or funding from any drug company.
- Received July 12, 2018.
- Accepted August 29, 2018.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.