


Abstract
Objectives: To demonstrate the importance of visual evoked potential (VEP) in determining the severity and prognosis of the disease and in monitoring the clinical course in patients with idiopathic intracranial hypertension (IIH).
Methods: This is a prospective cross-sectional study conducted covering the period between March 2014 and January 2015. The study included 32 patients recently diagnosed with IIH and 30 healthy volunteers. The initial VEP values of the IIH patients were compared to the VEP values of the healthy control group. Furthermore, the initial VEP values of the IIH patients were compared with their VEP values after one month of treatment.
Results: The mean age of the IIH patients was 37.8±12.02 years. Of the IIH patients, 27 (84%) were females and 5 (16%) were males. There was a statistically significant association of the initial VEP values with the visual field findings (p=0.011) and visual acuity (p=0.040). Moreover, a statistically significant difference was found between the control group and IIH patients in terms of right (p<0.001) and left P100 values (p<0.001). While 18 (56%) of the initial VEPs of IIH patients were pathological, 14 (44%) of the second VEPs were pathological, and this difference was not statistically significant (p=0.125).
Conclusion: A relationship between the VEP P100 values and the severity of the disease was detected, while the importance of monitoring VEP values in the follow-up of IIH patients was not demonstrated.
Idiopathic intracranial hypertension can be defined as raised intracranial pressure with a normal cerebrospinal fluid (CSF).1,2 The overall incidence of IIH is 2.4/100,000; however, the incidence is 22/100,000 in obese women.3 Indeed, the female gender and a high body mass index (BMI) are important risk factors for the disease and female patients account for 90% of the cases.4,5
The visual field is commonly affected in IIH patients.6 Although the visual field is currently the most sensitive method to monitor visual disturbances during the course of the disease, its specificity and sensitivity is not 100%.6,7 However, an early diagnosis, determination of the disease severity, and follow-up of the patients with IIH are critical as IIH can cause serious and irreversible visual field defects and even vision loss during the course of the disease.7-9
The number of patients with IIH is on the rise globally as the number of patients with obesity increases day by day.10 There is a paucity of precisely sensitive and objective indicators of the disease for monitoring relapses and remission.11,12 Moreover, no sensitive and objective methods have been established yet to determine the disease severity in order to decide whether surgery should be performed in these patients.12-14
Despite the potential of IIH to cause visual morbidity, only a limited number of studies are available in the literature to predict the potential impact of IIH on the vision.13 The findings obtained by VEP reflect the functions of the visual pathways extending from the retina to the occipital cortex. The test is particularly sensitive to demonstrate conduction disturbances in the anterior (pre-chiasmatic) visual pathway.15,16 A few studies have shown abnormal findings in VEP tests in patients with IIH, indicating the importance of VEP in the evaluation of the visual functions.17 In the literature, we found only one study evaluating the value of VEP values in the follow-up of patients with IIH.17
This study aimed to demonstrate the importance of VEP testing in determining the severity and prognosis of the disease and in monitoring the clinical course of the patients with IIH as the number of studies evaluating this subject is limited in the literature.
Methods
This prospective, cross-sectional study was performed in a tertiary care hospital in Van, Turkey between March 2014 and January 2015. The Ethics Committee of Yuzuncu Yil University School of Medicine in Van, Turkey, approved the study. This study was performed in compliance with the Declaration of Helsinki and written informed consent was obtained from all participants.
Lumbar puncture (LP) was performed in 63 consented patients admitted to the neurology outpatient clinic for diagnosis, examination, and treatment to confirm a pre-diagnosis of IIH according to the revised modified Dandy criteria. Of these patients, 50 (79%) received a final diagnosis of IIH. Of the 50 patients, 18 were excluded from the study because they could not completely meet the exclusion criteria or they could not comply with the treatment or follow-up procedures of the study. Consequently, 32 patients with IIH were included in the study.
The patients younger than 18 years old, the patients with a suspicion of any type of eye disease other than papilledema; pregnant or breastfeeding patients; patients with a history of diabetes, hypertension, or any other chronic diseases; patients with hormonal disorders, B12 deficiency, anaemia, folate deficiency; and patients with elevated levels of urea, alanine aminotransferases (ALT), Aspartate aminotransferases (AST), or patients with elevated levels of other metabolic values were excluded from the study. A total of 30 healthy volunteers with no neurological or ophthalmological pathologies, and who complied with the exclusion criteria, were included in the study.
Brain magnetic resonance (MR) imaging, brain MR venography, and brain MR angiography were performed in all patients. Lumbar puncture was performed in the lateral decubitus position to measure the intracranial pressure. A detailed neuro-ophthalmologic examination was performed in all patients including Snellen test for visual acuity, ophthalmoscopic examination, and fundus photography. Humphrey visual field test was performed by automated perimetry. Any deterioration in the visual field was evaluated as abnormal.
For performing the pattern VEP recording (Medelec, Synergy multimedia EMG/EP; Oxford Inst. Medical Systems Division, England), the active electrode was placed on the occipital bone 2 cm above the external occipital protuberance, the reference electrode was placed in front of the frontal hairline, and the earth electrode was placed on the ear lobe. In patients with pattern VEP (pVEP); the evaluated parameters were the P100 latency (ms) and P100 amplitude (µV). Pattern-VEP was recorded at a rate of 2 Hz. At least 100 stimulations were given to each eye twice at 5 minutes intervals. The pattern size was 0.3° and the contrast was 99% of the Michelson constant. The recordings were repeated when the rate of blink artefact or peripheral artefacts reached a level above 5%. A well-experienced electrophysiology technician (with 10 years of experience) ensured that the patients maintained accurate fixation during all recordings. The following were recorded and reported by the neurophysiologist; including the patient compliance to the test; the movements that might affect the results; and the pupil diameter, age, and refractive error of the patient. The test was repeated if considered necessary. The interpretation of VEP results was performed by the neurophysiologist.
The pathological VEP results included a P100 latency of 116 ms or higher, distorted VEP waveforms, interpeak latency differences (a difference between the P100 values of the 2 eyes) of greater than 6 msec, amplitude values less than 4 µV, and amplitude differences higher than 50% between the 2 eyes.
Body mass index was calculated for all patients included in the study. The study patients were divided into 2 groups based on their BMI. Those with a BMI lower than 30 were assigned into one group and those with BMI values 30 or higher (obese patients) were assigned to another group.18,19 The patients’ pain levels at the time of hospital admission were scored according to the visual analogue scale (VAS). These scores were compared with the VAS scores found in the control visit after the treatment. Based on the VAS scores, the patients were divided into 3 groups as the patients with diminished VAS scores, stable VAS scores, and increased VAS scores.
In our study, we compared the VEP values of the healthy control group with those of the patient group diagnosed with IIH for the first time. Furthermore, the VEP values of the IIH patients after one month of treatment were compared to the initial VEP values. (all study patients received treatment by reducing the CSF pressure after LP and in addition, they received medical treatment consisting of acetazolamide (manufactured in Turkey) solely, administered at doses in the range from 500-1000 mg). Idiopathic intracranial hypertension patients were divided into groups according to age, gender, BMI, fundoscopic examination findings, visual field findings, visual acuity, CSF pressure, and VAS scores. The categorical variables were expressed in number and percentages and the data in each group were analysed to demonstrate their effects on VEP results.
During the follow-up visits, it was decided to apply shunt treatment to 2 patients and those patients underwent shunt surgery. One month after the surgical procedure, the third VEP tests were performed on the patients and the VEP results obtained were included in the data analysis.
Pubmed and Google Scholar were used for the literature review.
Study design
The statistical analyses were performed using the Statistical Package for the Social Science (SPSS), Version 21.0 (IBM Corp., Armonk, NY, USA). In our study, the descriptive statistics for continuous variables were expressed as mean, standard deviation, minimum and maximum values; while the categorical variables were expressed in number and percentage. The distribution of the data was tested with the Shapiro Wilk test. A one-way analysis of variance was performed to compare the mean values of continuous variables in the groups. The independent sample t-test was used for testing the normally distributed data. The chi-square test and McNemar test were used in order to determine the relationship between groups and categorical variables. The statistical significance level was accepted as 5%.
Results
Demographic and clinical characteristics of the patients are presented in Table 1. One of the IIH patients reported a decrease in visual acuity 3 days after the onset of their complaints. The reduction was confirmed by the Snellen eye screening test. As severe vision loss occurred within 4 weeks, this patient received the diagnosis of Fulminant IIH. The mean age of the healthy control group was 38.11±10.542 years. Of these healthy individuals, 27 (84%) were males and 5 (16%) were females. There were no statistically significant differences in age (p=0.744) and gender (p=0.911) between the IIH group and the healthy control group. A comparison of the initial VEP values between the IIH group and the healthy control group is presented in Table 2. The initial VEP values were evaluated as normal in 14 (44%) patients and abnormal in 18 (56%) patients.
Demographic and clinical features of patients with idiopathic intracranial hypertension.
Comparison of the initial VEP values of IIH patients to the VEP values of the healthy control group.
The mean CSF pressure of the IIH patients with obesity was 409.50±86.175 mm-water, while the average CSF pressure of the non-obese IIH patients was 362.86±70.757 mm-water. The CSF pressure of IIH patients was significantly higher in obese subjects (p=0.044). While the mean CSF pressure of the patients with visual field abnormalities was 390.40±81.470 mm-water, the mean CSF pressure of the patients with normal visual field findings was 374.29±92.711 mm-water, and the difference between these figures was not statistically significant (p=0.656). The mean CSF pressure of the IIH patients with reduced visual acuity was 412.50±108.989 mm-water and the mean CSF pressure of the IIH patients with normal visual acuity was 378.33±72.871 mm-water. The difference between these figures was not statistically significant (p=0.320). The mean CSF pressure of the IIH patients with pathological VEP test results at baseline was 405.56±88.399 mm-water, while the mean CSF pressure of the IIH patients with normal VEP results was 362.86±70.757 mm-water. The difference between these values was not statistically significant (p=0.151).
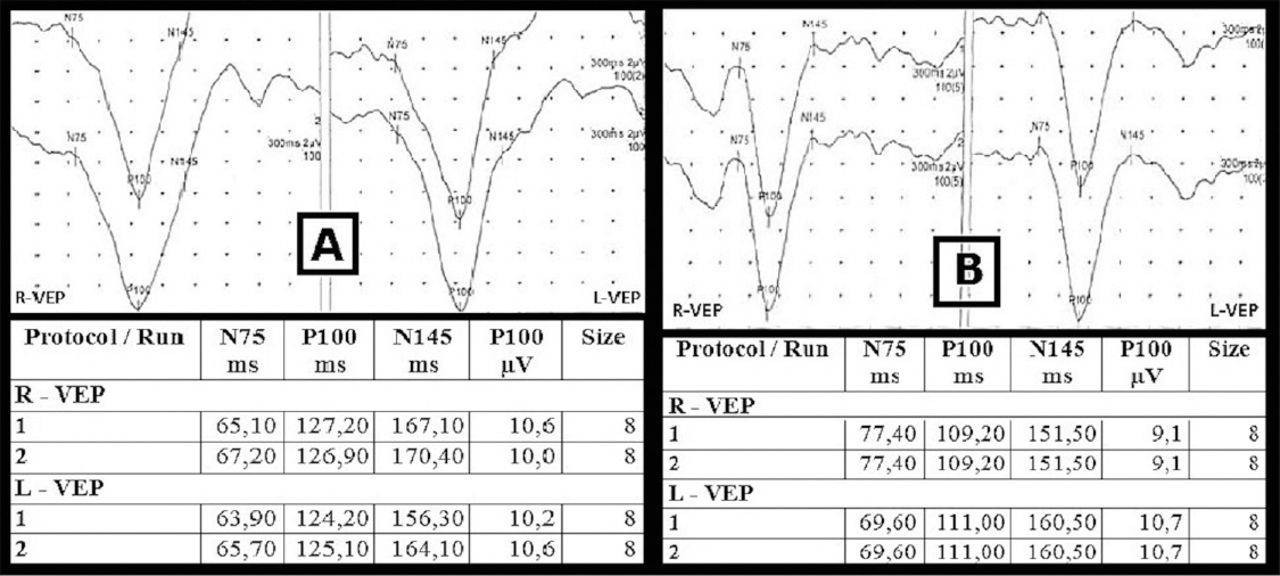
Table 3 shows the relationship of pathological VEP results with gender, obesity, and visual acuity and visual field findings at admission. Table 4 shows the comparison of the initial VEP results and the second VEP results of the IIH group. While 14 (44%) of the initial VEP were normal and 18 (56%) were pathological, 18 (56%) of the second VEP taken after one-month treatment were normal and 14 (44%) were pathological. The difference was not statistically significant (p=0.125). Visual evoked potential images of a patient who showed improvement in VEP values after one month of treatment were shown in Figure 1.
The relationship of pathological VEP results with gender, obesity, and visual acuity and visual field findings at admission.
Comparison of the initial VEP results of IIH patients with second VEP results

Visual evoked potential (VEP) images of a patient who showed improvement in VEP values. Visual evoked potential images and values of a patient 3 hours before lumbar puncture (A). Visual evoked potential images and values of the same patients after one month of treatment (B). [X-axis: latency (ms), Y-axis: amplitude (µV)].
At the time of admission, 7 (28%) visual field revealed normal results and 25 (78%) revealed pathological results. The visual field performed after one month of treatment revealed 16 (50%) normal results and 16 (50%) pathological results, and the difference was statistically significant (p=0.012).
The relationship between the improvement in VEP results and the changes in VAS scores was investigated. Of the patients with reduced VAS scores, VEP results were improved in 4 but remained pathological in 12. None of the patients with stable VAS scores experienced improvements. Of the patients with increased VAS scores, VEP results improved in one but did not improve in 8. The highest VEP improvement was detected in the patients with reduced VAS scores but this difference was not statistically significant (p=0.286).
Two patients with clinical deterioration underwent shunt treatment and the third VEP test was performed in these patients one month after the surgery. The VEP results of these 2 patients at baseline were pathological. Their second VEP results obtained after one month of medical treatment and the third VEP results taken one month after the shunt treatment were also pathological.
Discussion
In the literature, the age of IIH onset is reported to be variable; however, the mean age of onset is reported in the range from 25-37 years.8,20 In the literature, the ratio of female/male patients in IIH varies between 2/1 and 10/1 but in general it was reported in the range from 76.5-90%.4,20 In our study, the female/male ratio of the IIH patients was 27/5 and the mean age was 37.8 years (the oldest patient was 64 and the youngest patient was 18 years old). Our findings are consistent with the data reported in the literature.8,20
Headache is the most common symptom seen in 98% of the patients with IIH.17 Temporary vision loss occurs in 55-70% of the patients.20,21 Other symptoms may include photopsy, diplopia, pulsatile tinnitus, and vertigo.22,23 In our patient group, patients had headache, blurred vision, photopsy, eye pain, diplopia, tinnitus, and vertigo complaints, being consistent with the literature. The frequency of IIH patients without papilledema was reported as 11.9%.24 Unilateral papillary oedema was reported in 3-10% of the patients with IIH.21,25 In this present study, papillary oedema was not detected in 9% of the patients, while unilateral papillary oedema was found in 3% of the patients, and these findings were consistent with the literature.
The disease results in blindness in approximately 10% of patients and this figure may increase up to 32% in untreated cases.22,26 In 29-35% of patients with IIH, abnormal findings in visual acuity (Snellen chart test) was reported.22,27 Visual field defect was reported in 80% of patients.17 In our study on the patients, who were diagnosed with IIH for the first time, diminished visual acuity was observed in 8 (25%) patients and pathological findings in the visual field were found in 25 (78%) patients. These figures were consistent with the literature.
It has been suggested that there is a strong relationship between IIH and obesity.8,18 A theory attempting to provide an explanation to this relationship proposes that central obesity causes an increase in the intraabdominal pressure, resulting in increased pelvic and cardiac pressure.8,18 Consequently, the venous return is hampered, resulting in increasing intracranial venous pressure. The ultimate result is suggested to be increased intracranial pressure.8,18 The increased synthesis of adipose tissue products, which are leptin and ghrelin, have been suggested to play an effective role in developing IIH.8,18 Similarly, deteriorations in insulin and glucose metabolism in obese patients and changes in the levels of gender hormones, glucocorticoids, lipids, and free fatty acids can be some of the potential causes of IIH.8,18 The prevalence of obesity in IIH patients ranges from 70.5-94%.28 In our study, the obesity rate was 63% and this figure was slightly below the reported figures in the literature. This difference may be attributed to genetic differences across different populations. A study conducted by Gafoor et al28 showed no associations between CSF pressure and obesity. In our study, a relationship was found between the CSF pressure and obesity, which supported the current hypotheses.
Hamzeii-Moghadam et al17 found pathological VEP results at a rate of 23.3% at the time of diagnosis in IIH patients. El Habashy et al29 reported anomalous findings in VEP results in 63.3% of chronic IIH patients. In our study, VEP pathology was detected in 56.25% (18 patients) during the diagnosis. In the literature, this value was the highest rate of VEP pathology detected at the time of admission in IIH patients. The reason for this relatively high rate in our study may be due to diagnostic delays in rural areas leading to an inability to predict the disease onset precisely.
Hamzeii-Moghadam et al17 conducted the first study in the literature, comparing the baseline and after-treatment results of the visual field and VEP. They reported a significant relationship between the visual field findings and P100 wave latency. However, when the authors categorised the VEP results into 2 groups as pathological and normal, no statistically significant relationship was found between the VEP and visual field findings.17 Takkar et al13 found no statistically significant relationship of VEP results with the visual field and visual acuity findings. In our study, a relationship of VEP results was found with the visual acuity and visual field findings.
The most frequent complaint of IIH patients was pain and this study investigated the association between the pain severity and VEP results. In our study, there was not a statistically significant relationship between the changes in VAS scores and VEP results.
Today, the most commonly recognized and used method is the visual field test in evaluating the prognosis and clinical course in patients with IIH.17,22 Therefore, the association of visual field and VEP findings found in our study points to the importance of VEP in the IIH patients and contributes to the literature. In our study, 5 patients had improved VEP results. Furthermore, no pathological changes emerged in any of the VEP values in patients with normal baseline VEP findings. These findings in our study may lead to the suggestion that the short-term treatment in IIH has a positive effect on VEP results in patients with slightly affected optic nerve. An increase in the mean P100 latency was found in both eyes of the study patients. This might have occurred due to the fact that short-term treatment is insufficient to inhibit the inflammation and demyelination process in the patients with a more significant optic nerve damage.
Limitations
The short duration of the study is the main limitation of this study. Another limitation is the relatively small sample size.
In conclusion, besides the longer P100 values found in VEP compared to the findings in the healthy control group, there was a statistically significant relationship of the VEP results of the patients with the visual field and visual acuity findings. These results of the study may suggest that a relationship between the severity of the disease and VEP results exist at the time of diagnosis. Significant improvements were observed in the visual field after one month of treatment in the follow-up visits. However, the significant increase in P100 latency and the absence of a relationship between the VAS scores and VEP results may indicate the limitations of VEP findings in monitoring these patients during the follow-up period.
Further long-term studies are required using optic coherence tomography, VEP, and visual field findings together in monitoring the IIH patients during the follow-up period in order to determine the most effective method.
Acknowledgements
The authors gratefully acknowledge (www.protranslate.net) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received January 20, 2019.
- Accepted April 15, 2019.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.