


Abstract
Objectives: To establish the normal Creatine phosphokinase (CPK) range in newborns of all 3 modes of delivery and prove that high CPK level in neonates is not specific a indicator for muscular pathology.
Methods: This is a prospective cohort study that is conducted in King Abdulaziz Medical City and King Abdullah Specialized Children Hospital in Riyadh and included 504 term neonates who were born between March 2021 and August 2021. Two hundred and fifty three were males and 251 were females. Data and consents were managed and collected using 2 coordinators.
Results: Duration of the second stage of labor, age on the first CPK test and fetal gestational age were significantly correlated with CPK values (r=0.197, r=-0.234, r=0.274, respectively). The normal ranges for each delivery type were 334 U/L-2667U/L in normal spontaneous vaginal delivery, 265U/L-1182U/L in elective cesarean section, and 223U/L-3082 U/L in emergency cesarean section.
Conclusion: The CPK was elevated in all neonates in all 3 modes of deliveries. An elevated levels of CPK in neonates is not a specific indicator for any congenital muscular pathology.
Creatine kinase is formed of polymers with 2 subunits—each is under separate genetic control.1 Creatine kinase is an intracellular enzyme that exists in high concentrations in skeletal muscle, myocardium, and brain; it is found in lower concentrations in other visceral tissues;2 many types depend on the source. Creatine phosphokinase(CPK)-BB is only found in the brain and lungs while CPK-MB is related to the heart; CPK-MM is related to skeletal muscles.3 The CPK helps maintain muscle mass and facilitates its function and performance.4 Hypoxia or any other type of injury can disrupt the cell membrane and releases CPK from the cytosol into the systemic circulation. Thus, CPK is an important and sensitive test for muscle injury.2 High levels of CPK can be used as an important biomarker for many diseases and conditions such as myocarditis, myocardial infarction, pulmonary infarction, strokes, etc.5 It can also detect genetic muscular disorders such as Duchenne muscular dystrophy—a progressive muscle disease that occurs as a result of altered dystrophin proteins.6
An increase in CPK levels is sometimes due to physiological causes other than pathological reasons, e.g., exercising or any minor trauma to the muscles can increase CPK levels. Serum creatine kinase has been shown to be higher in infants than adults with a peak 24 – 48 hours after delivery due to the perinatal trauma during delivery.3 The normal CPK values in a newborn born without any complications might be different than the adult normal range. This would help neurologists know when to suspect a disease. It could also change practice by avoiding unnecessary and unwanted investigations. However, extracting multiple blood samples to measure CPK followed by biopsy to rule out muscular disease is challenging, costly, and potentially harmful. This can be avoided when we know the normal level of CPK in newborns.
Here, we report a prospective study conducted in the Clinic of Pediatrics at the University of Perugia that assessed the serum levels of CPK in newborns. Serum samples were collected from 10 full-term newborns delivered via uncomplicated vertex delivery. The results showed that the peak of serum CPK level in newborns was 24 hours after delivery. It then gradually declined until it reached the adult normal range at day ten.7 Twenty-six newborns with uneventful prenatal histories, no perinatal stress, and typical vaginal deliveries showed elevation in cord blood CPK and significant elevation in serum CPK at twenty-four hours of age in both skeletal and cardiac muscles isoenzymes, but especially in the skeletal isoenzyme. These results were compared with values obtained in a group of 10 neonates with serious cardiac problems and revealed that there was no significant difference in CPK levels between the ill neonates and the normal neonates. These data indicate that caution is needed in the diagnosis of some neonatal cardiac syndromes based only on serum CPK levels and isoenzymes.8 The main aim of our study was to determine the normal range of CPK levels in newborns and to identify the time when high CPK levels return to baseline.
Methods
This was a prospective cohort study conducted in King Abdulaziz Medical City in Riyadh and King Abdullah Specialized Children’s Hospital. It included normal term neonates born between March 2021 and August 2021. A normal neonate is defined as a neonate born with a gestational age of 36 weeks or more and with no neonatal intensive care unit (NICU) admission. The study population was normal full-term neonates less than 24 hours old and born in King Abdulaziz Medical City-Riyadh. Exclusion criteria included NICU admission, fetal hypoxia, and obstetric complications. The data of this study were collected after obtaining Institutional Review Board approval from KAIMRC (RC20/666/R).
We collected parameters and data on patients including demographics, blood types, gravidity, parity, gestational age, delivery type, stages of labor durations, 1-, and 5-minutes APGAR scores, anthropometric variables of the neonates, mothers’ demographics, and blood type. We also measured CPK on the first 24 hours of age of the neonate and again on the seventh day from delivery; high CPK levels were repeated for 4-6 weeks post-delivery. All samples were obtained from a venous blood sample. For the measurements we used the Alinity Creatine Kinase Kit to measure CPK in all neonates. We collected venous blood and prepared serum. All specimens were free of red blood cell, fibrin, and any other particulate matter. We stored the specimen in a 2 to 8°C environment. We used the Statistical Package for the Social Sciences (version 22) for our statistical analysis. Categorical variables are presented as frequencies and percentages; numerical variables are presented as the mean ± standard deviation (SD). Spearman’s rho correlation analysis was used to test the correlations between different variables. Statistical significance was set to p<0.05.
Ethical considerations
The data were collected after obtaining Institutional Review Board approval from KAIMRC (RC20/666/R). Access for the data was only available to the research members. The confidentiality of all patients was preserved, and neither names nor medical record numbers were used or collected. A written informed consent form was signed by the participants‘ guardians prior to the blood test.
Results
The mothers’ who participated on our study were mothers (n=504) with no family history of muscular diseases were eligible and were enrolled. Most mothers had a normal spontaneous vaginal delivery 335 (66.50%); 102 (20.20%) had an elective caesarean section, and 67 (13.30%) had an emergency caesarean section. The mean age was 30.36±6.21 years old with a mean BMI of 32.06±5.88. The prevalence of underweight, normal weight, overweight, and obese mothers were 0.0%, 10.70%, 28.60%, and 60.70% respectively. The weight of the mothers was taken before the delivery, which could add from 13.4 kg to 15.1 kg to the pre-pregnancy weight and could explain the noticeably higher prevalence of weight and BMI. The prevalence of the neonates blood group types O, B, A and AB were were 50%, 20.6%, 24.8%, and 4.6% respectively. The other characteristics are in Table 1.
- Maternal and neonatal demographics.
As for the neonates, there were 504 neonates included after applying the inclusion/exclusion criteria. All included children were ≥36 weeks of gestation. Of these neonates, 253 (50.2%) were males and 251 (49.8%) were females. The mean weight and height of the neonates were 3.08±0.42 kg and 50.1±2.3 cm, respectively. The mean head, chest, and abdominal circumferences were 34.4±1.5 cm, 32.6±1.7 cm, and 30.7±2.2 cm, respectively. Twenty (4.2%) neonates had an APGAR score of 7 or less at the first minute of age, 40 (8.3%) had an APGAR score of 8 at the first minute of life, 421 (87.5%) neonates had an APGAR score of 9 at the first minute of age, and 23 neonates had a missing APGAR data at the first minute of age. At 5 minutes of age, the prevalence of 8, 9, and 10 APGAR scores were 5 (1.0%), 473 (98.3%), and 3 (0.6%); (Table 1 & 2).
- Neonatal anthropometric parameters.
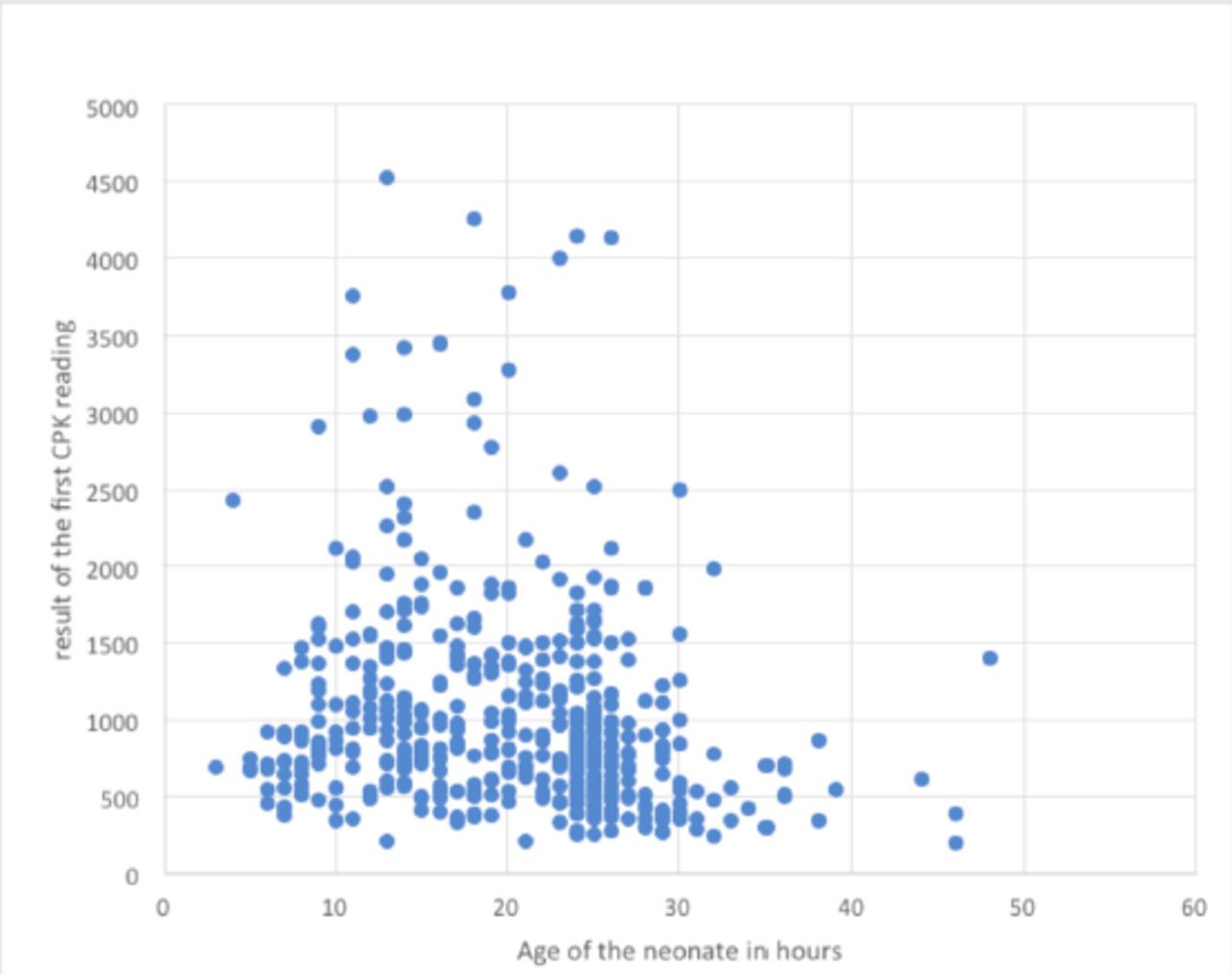
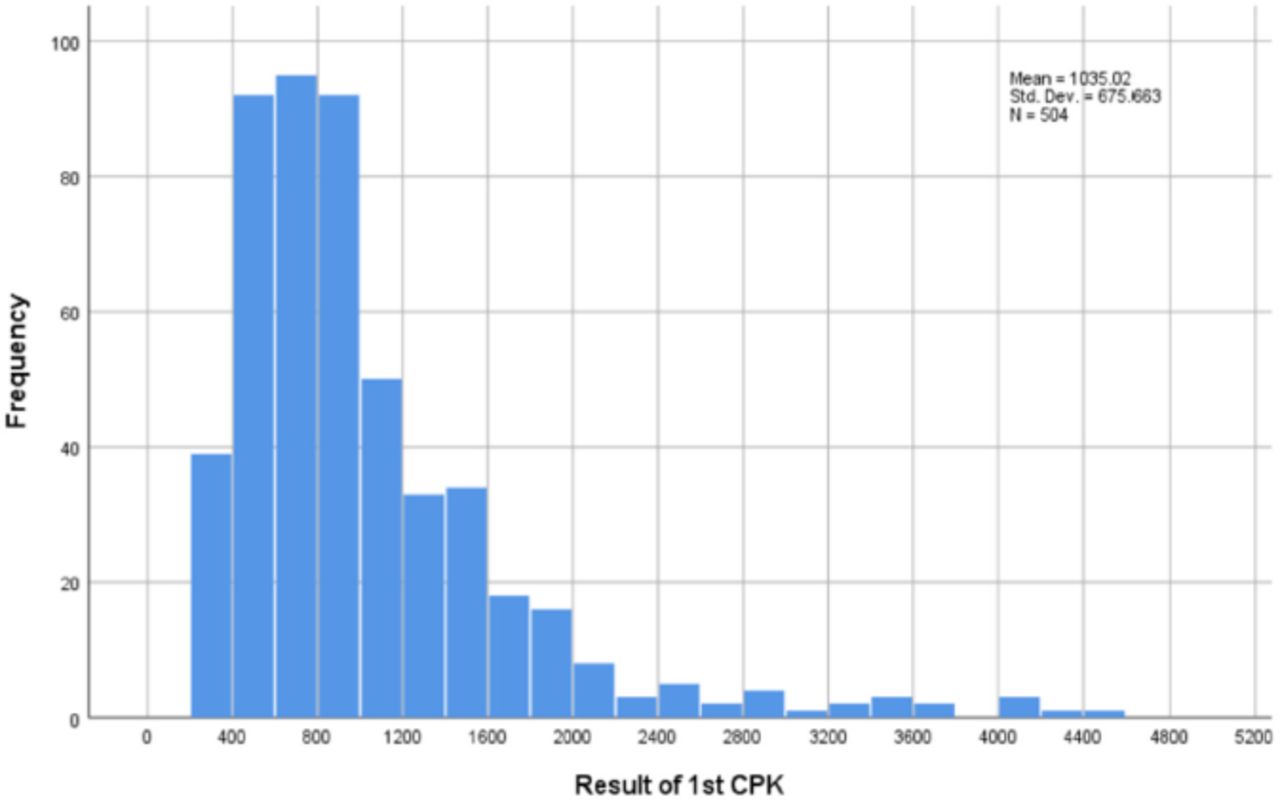
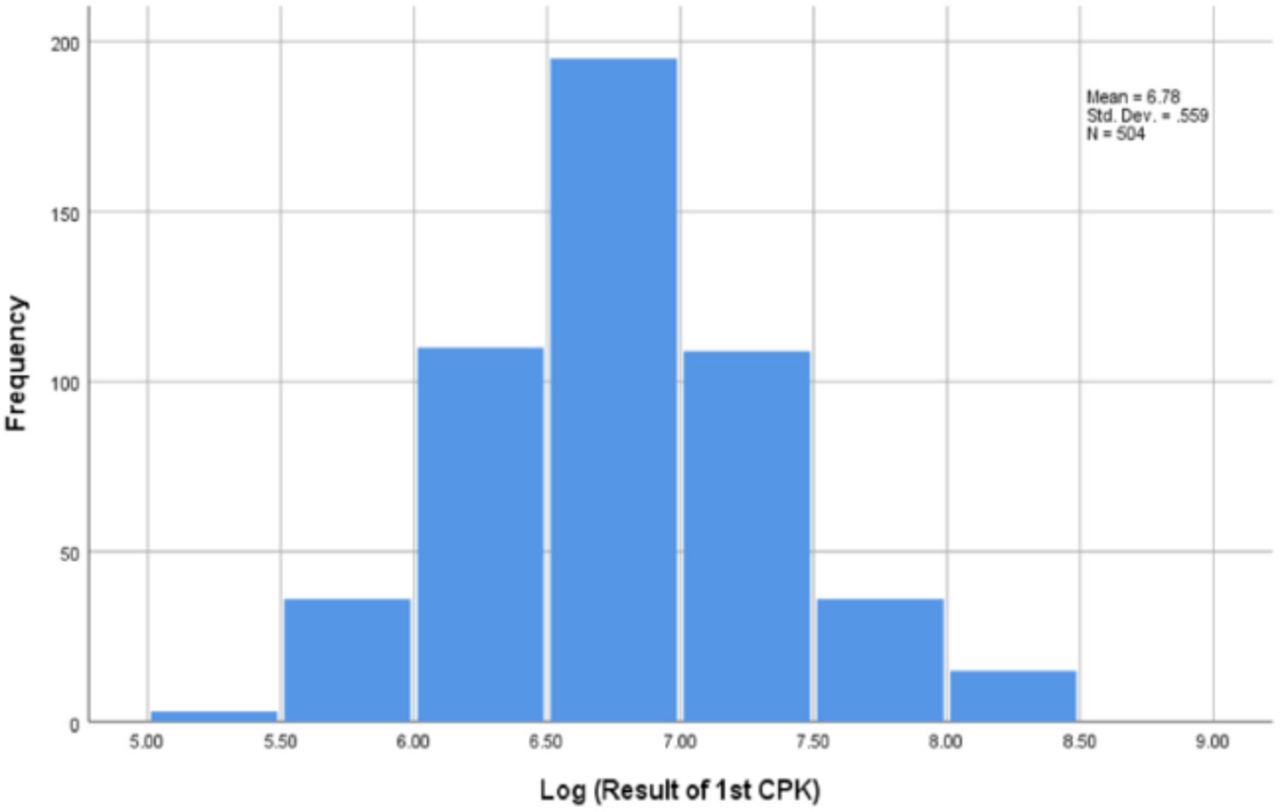
The mean of each CPK value of each delivery mode, normal spontaneous vaginal delivery, elective cesarean section, and emergency cesarean section are 1098.3±673.0, 805.8±465.2, and 1067.4±867.2, respectively. The correlation between the CPK value and age in hours can be seen in Figure 1. In Spearman’s rho correlation analysis, the duration of the second stage of labor, age on the first CPK test, fetal gestational age, gravidity, and parity were significantly correlated with CPK values (r=0.197, r=-0.234, r=0.274, r=-0.101, r= -0.135, respectively). Other variables like maternal BMI; duration of the first and third stages of labor; head, chest, and abdominal circumferences; birth weight and height; and APGAR scores on the first minute and fifth minute of life were not significantly correlated with the CPK value on the first day of life using Spearman’s rho correlation analysis (-0.047, 0.109, -0.041, 0.006, 0.072, 0.028, 0.04, 0.048, 0.014, -0.005, respectively). Initially, 504 neonates had the CPK test on the first day of life. However, only 172 neonates came back after seven days to measure the CPK level. This was a response rate of only 34.12% and was likely because most participants lived outside Riyadh City and already left to their town; others were simply uncooperative. All 504 neonates had an elevated first reading of CPK (higher than 200 U/L) with a mean value of 1035.02±675.7 (SD). On the second reading of CPK test, all 172 neonates experienced a decrease in the CPK value; 167 (97%) neonates had a normalized CPK value with only 5 (3%) neonates still having an elevated CPK value. However, even these still experienced a decline from the first CPK measurement. We ordered a third test for the remaining 5 (3%) neonates who still did not have a completely normalized CPK level 7days post-delivery, but they were lost to follow-up. Of the 504 neonates, 335 (66.4%) were born via normal spontaneous vaginal delivery (NSVD), 102 (20.2%) were born via elective cesarean section, and 67 (13.3%) were delivered via an emergency cesarean section. We tried to establish the normal range for CPK in the first day of life, but it was skewed to the left due to outliers (Figure 2). The skewness was proven using tests of normality and the Shapiro-Wilk test with a result of <0.001. To overcome the skewness, the log value of each CPK test was taken, and it showed a normal distribution as in Figure 3.
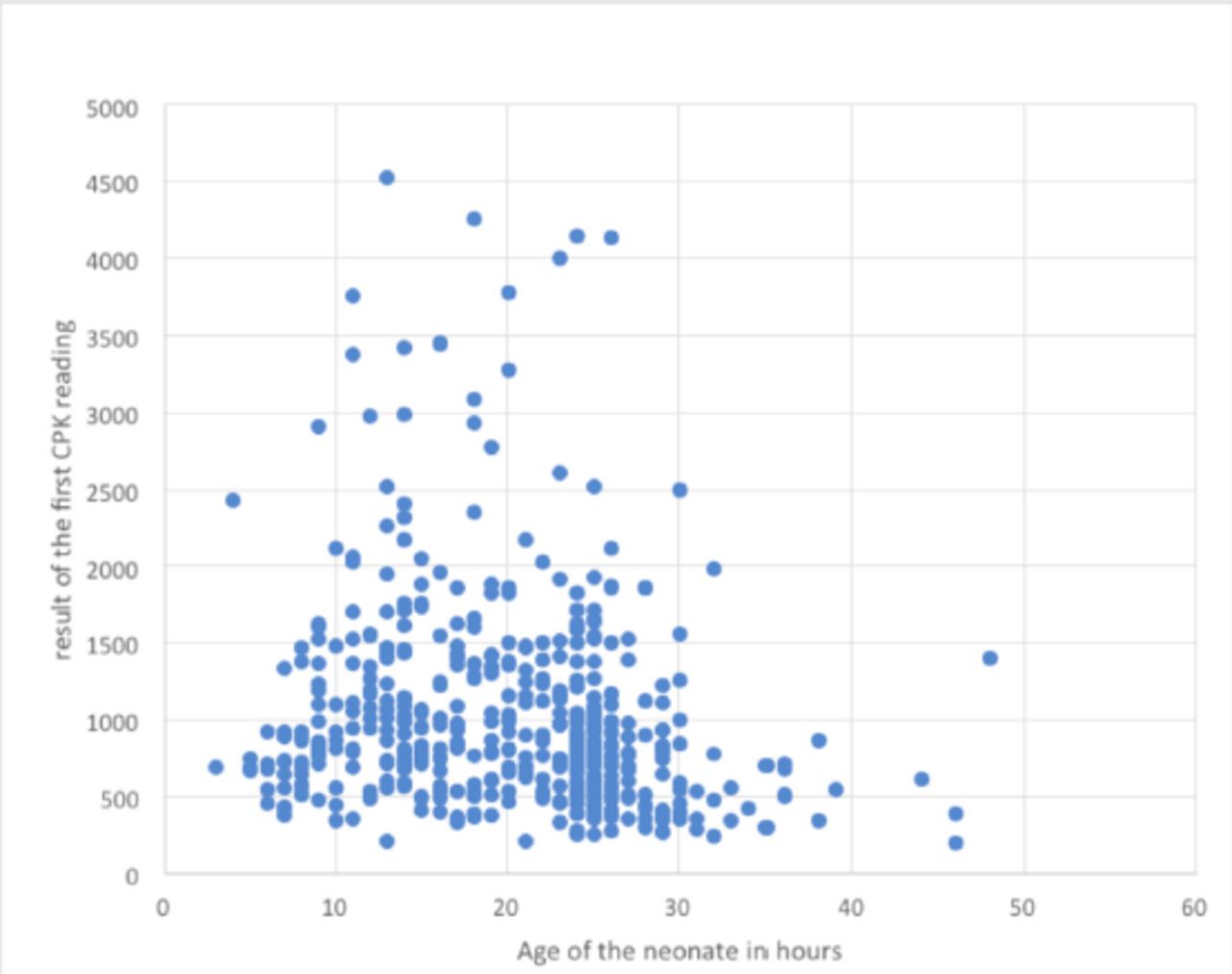
- Correlation between the age of the neonate and the first CPK value
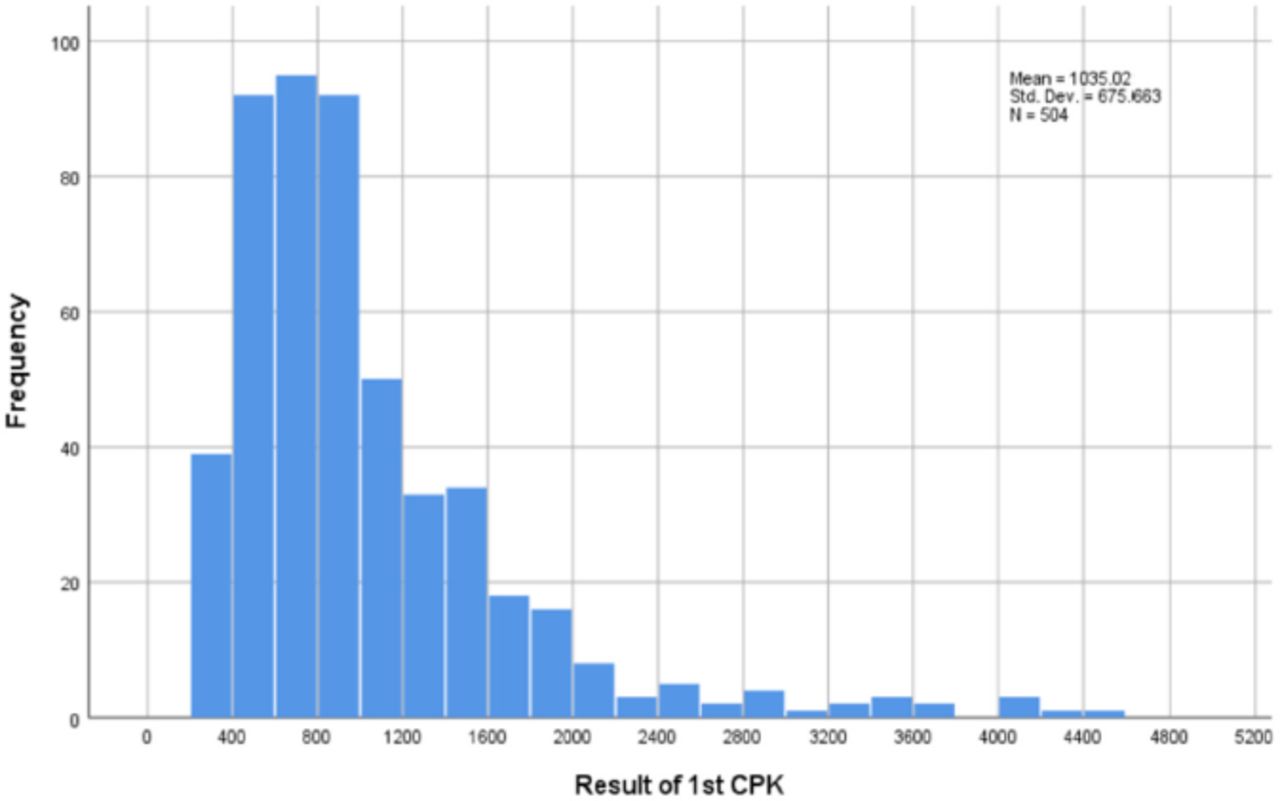
- Distribution of the first CPK value.

- Distribution of the log value of the first CPK measurement.
From the log values we established the normal ranges for each delivery type to be 334 U/L-2667U/L for NSVD, 265U/L-1182U/L for the elective cesarean section, and 223U/L-3082 U/L for the emergency cesarean section. The means for each mode of delivery are 1098.3±673.2 for NSVD, and 805.8±465.2 for the elective cesarean section, and 1067.4±867.2 for the emergency cesarean section.
Discussion
Labor and delivery require a tremendous amount of muscular activity from the mother as well as the newborn. The extensive fetal physical effort that occurs during labor is influenced by multiple factors related to both the mother and the fetus.9 The mother regulates voluntary abdominal pushing, the contraction of the uterus, and the supra-umbilical diastasis; fetal factors include the position of the fetus, the fetal presentation during labor, and the fetal cephalic circumference. These can all lead to increased CPK levels in newborns.9
Here, we found additional factors that significantly correlate with CPK levels in newborns. A positive correlation between the second stage of labor and CPK (r=0.197) was seen, thus suggesting that the muscular contraction that happens during the second stage of labor compresses the newborn and causes an increase in CPK levels. Minini et al10 showed that neonates who have vaginal delivery rather that a caesarean section and a prolonged second stage of labor have higher CPK levels. On the other hand, a significant negative correlation was found between age in hours and CPK levels (r=-0.234) post labor. The CPK levels decrease perhaps due to the reduction in muscle stress. Unfortunately, we were unable to find a study that supports our findings and that investigates the correlation between CPK levels and newborn age.
The findings suggest elevated CPK levels in all neonates in all 3 modes of delivery: spontaneous vaginal delivery, emergency cesarean section, and elective cesarean section. Moreover, the CPK levels returned to normal after 7 days of birth in 97% of the neonates. The remaining 3% showed significant declines as well. Moreover, we ordered a third test for the remaining 3% to check specifically when their CPK levels will return to normal, but they were unfortunately lost to follow-up.
Gilboa et al11 studied the blood sample of 70 newborns and showed a ten-fold increase in CPK levels in all newborns versus the normal range in adults. All returned to normal at the fourth day of age. Another study measured the CPK level of 101 newborns on the first day of life and showed a significant raise in CPK levels in all newborns and again on the fourth day. There was a significant decline in CPK levels, but this was still three-fold higher than the normal range of an adult.12 These studies demonstrate similar results to our study.11,12
Our samples were from venous blood. Other methods of sampling techniques such as capillary sampling can give overestimated values and can be less accurate than venous sampling. Oliveira et al13 showed that capillary samples overestimated venous samples by 130 U/L (61%) with some moderate variance and low bias. Amato et al14 reported CPK measured in cord blood and capillary blood samples. The CPK-MB type was missing in the cord blood samples, and the CPK-bb type was significantly lower in cord blood versus the others, thus indicating that cord blood sampling is not as reliable as other techniques—especially venous sampling.
All modes of delivery had a significant increase in CPK levels. Emergency cesarean section had the highest followed by vaginal delivery and then elective cesarean section. This suggests that delivery mode stresses on the musculoskeletal tissue of the neonate results in elevated CPK levels. Thus, the normal range of CPK in neonates needs to be recalculated. We calculated and set a normal range for each type of delivery. The emergent cesarean section ranged from 223 to 3082, the vaginal delivery ranged from 334 to 2667, and the elective cesarean section ranged from 265 to 1182. Any value less or more than the mentioned ranges is considered abnormal and needs further study.
The CPK levels tend to be high in the first few days of the neonatal period and are related to the mode of delivery. Torab et al15 demonstrated that CPK levels in neonates born vaginally were higher than those born through elective cesarean section. Malamitsi-Puchner et al16 found that high CPK levels were positively correlated with vaginal delivery versus cesarean section. Similarly, Bodemesteiner et al17 noted postpartum CPK levels were higher in subjects delivered vaginally versus cesarean section, thus suggesting that the mechanism of natural birth has a role in elevated CPK levels in infancy. This supports our first theory.
Our study showed that emergency cesarean section had the highest levels of CPK, which leads us to our second theory: Elevated CPK levels are caused by the muscular stress during vaginal delivery and labor as well as additional variables: the position and the presentation of the fetus, the pressure on the fetus during pregnancy, and the fetus body measurements in relation to the size of the mother’s pelvis. This explains why CPK is also raised during cesarean sections.
Furthermore, the CPK levels were significantly higher in emergency cesarean section perhaps due to multiple factors. The physician does not need to do an emergency cesarean section unless there is an obstetric complication that can affect the blood circulation or cause extensive pressure on the fetus. The obstetric complications that lead to emergency cesarean section include placenta abruption, vasa previa, and hypertensive disorders. These complications can alter the normal mother-fetal blood circulation, thus leading to blood insufficiency and hypoxia to the fetus, thus resulting in fetal brain injuries and likely raising CPK levels.18-19 On the other hand, obstetric complications like prolonged labor due to the small size of the pelvis floor of the mother or malposition of the fetus will cause extreme pressure on the fetus—this will also lead to elevated CPK levels versus uncomplicated labor.
A prior study compared modes of delivery and their relation to CPK: CPK levels were the highest in neonates born via emergency cesarean section.20 They suggested that this could be due to anesthesia or tissue injury caused by surgery.20
The study outcomes and findings should be approached and interpreted considering strengths and limitations. This study included many patients. Most prior work included fewer than 200 patients 8,12,16,17 but ours included 504 patients. We obtained blood samples using venous sampling technique, which is more accurate than capillary heal puncture for serum CPK levels.13,14 In addition, most prior work did not include emergency c-section,16,17 but we included all types of delivery. Limitations include limited follow-up in the second CPK test. Most patients were lost to follow-up.
Conclusion
The CPK is an important and sensitive test for muscle injury and an important biomarker for many muscular diseases. It also increases due to some physiological effects. This study demonstrates that the mean total CPK levels in all neonates were significantly high in all modes of delivery with emergency C-section having the highest levels followed by vaginal delivery and then elective C-section. Thus, elevated CPK levels post-labor is normal and does not need further investigations.
Acknowledgment
We would like to acknowledge Ms. Layla Alharbi and Ms. Sarah Alhajaj for the consent form collection from the guardians, and for arranging the dates of the newborns blood withdrawals. In addition we would like to thank American Manuscript Editors for the English language editing.
Footnotes
Disclosure. This study was funded by King Abdullah International Medical Research Center’s (KAIMRC), Riyadh, Kingdom of Saudi Arabia.
- Received May 9, 2022.
- Accepted August 9, 2022.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.