


Abstract
Fahr’s disease (FD) is a neurodegenerative disorder characterized by symmetric calcifications in the bilateral basal ganglia and dentate nuclei. Mutations in six genes are known to cause FD. In the present case, a 44-year-old woman was admitted because of bradykinesia that had started developing 3 years ago. Brain CT and MRI revealed severe calcification in the bilateral basal ganglia, thalamus, dentate nuclei, and subcortical white matter. Whole-exome sequencing revealed two previously described compound heterozygous mutations within the MYORG gene. About one year later, the patient developed sudden-onset left-sided hemiparesis. The MRI revealed a small infarction in the right internal capsule. Therefore, the present case findings expand the clinical spectrum of FD. Importantly, the association between ischemic stroke and FD needs to be further studied.
Fahr’s disease (FD), is a rare neurodegenerative disorder which is characterized by symmetric calcium deposits in the basal ganglia, globus pallidus, putamen etc.1 In patients with these imaging characteristics, FD may be diagnosed after other causes of secondary calcification are ruled out. Clinically, FD shows a wide spectrum of neurologic and psychiatric symptoms including parkinsonism, tremor, dystonia, ataxia, seizures, migraine, cognitive impairment, and psychosis, among others.
The clinical symptoms and severity of FD are variable even between members of the same family, and some family members may be asymptomatic. The FD shows an autosomal dominant or recessive pattern of inheritance.1 Dominantly inherited forms of FD have been well identified by former studies, while recent studies have shown that the myogenesis-regulating glycosidase (MYORG) gene and junctional adhesion molecule 2 (JAM2) gene are associated with recessive forms of FD.1-3 In the present report, we have described a rare case of a female patient diagnosed with FD who carried biallelic mutations in the MYORG gene and presented with parkinsonism and acute ischemic stroke.
Case Report
Patient information
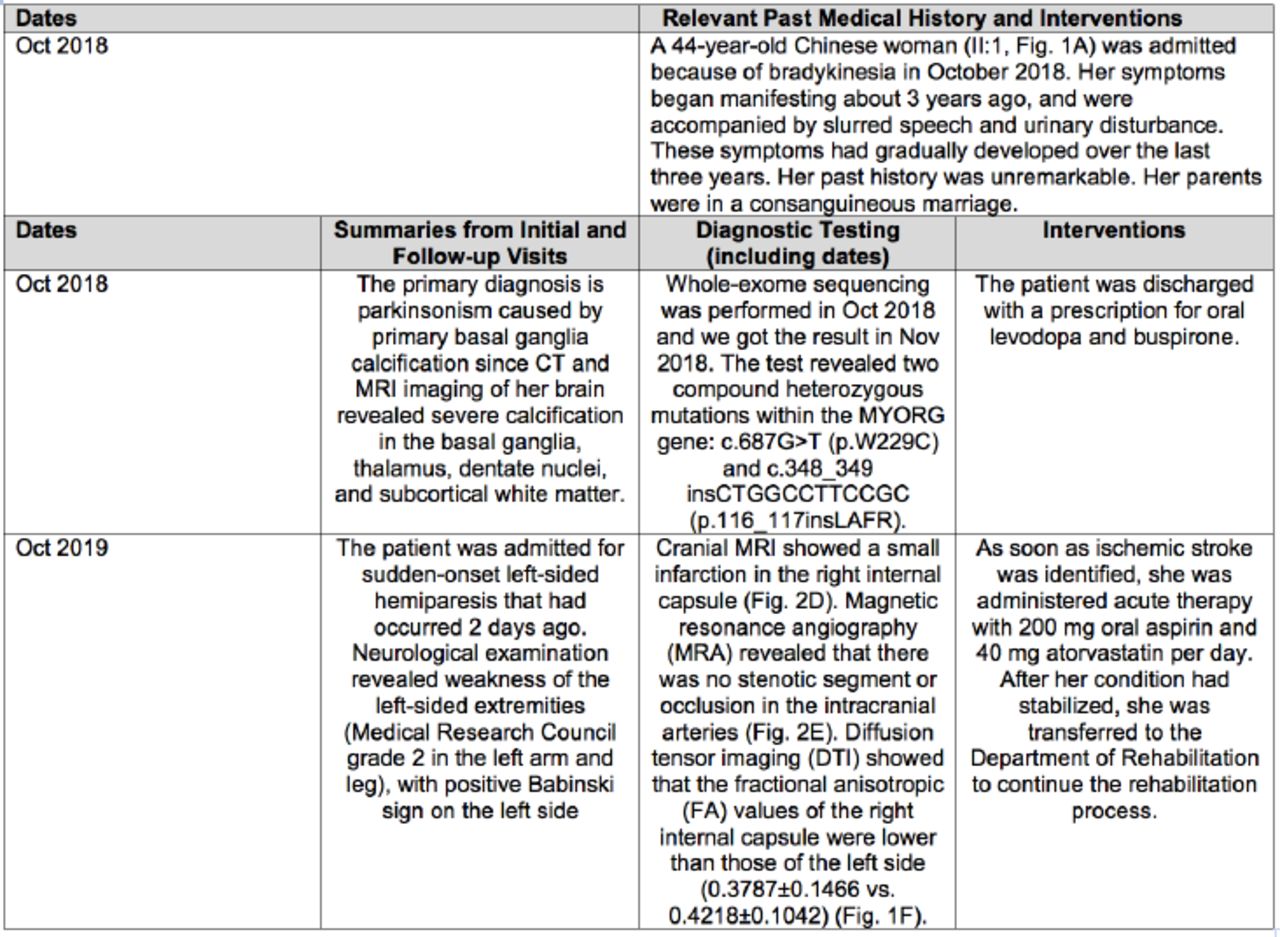
A 44-year-old Chinese woman (II:1, Figure 1A) was admitted because of bradykinesia in October 2018. Her symptoms began manifesting about 3 years ago, and were accompanied by slurred speech and urinary disturbance. These symptoms had gradually developed over the last three years. Her past history was unremarkable.

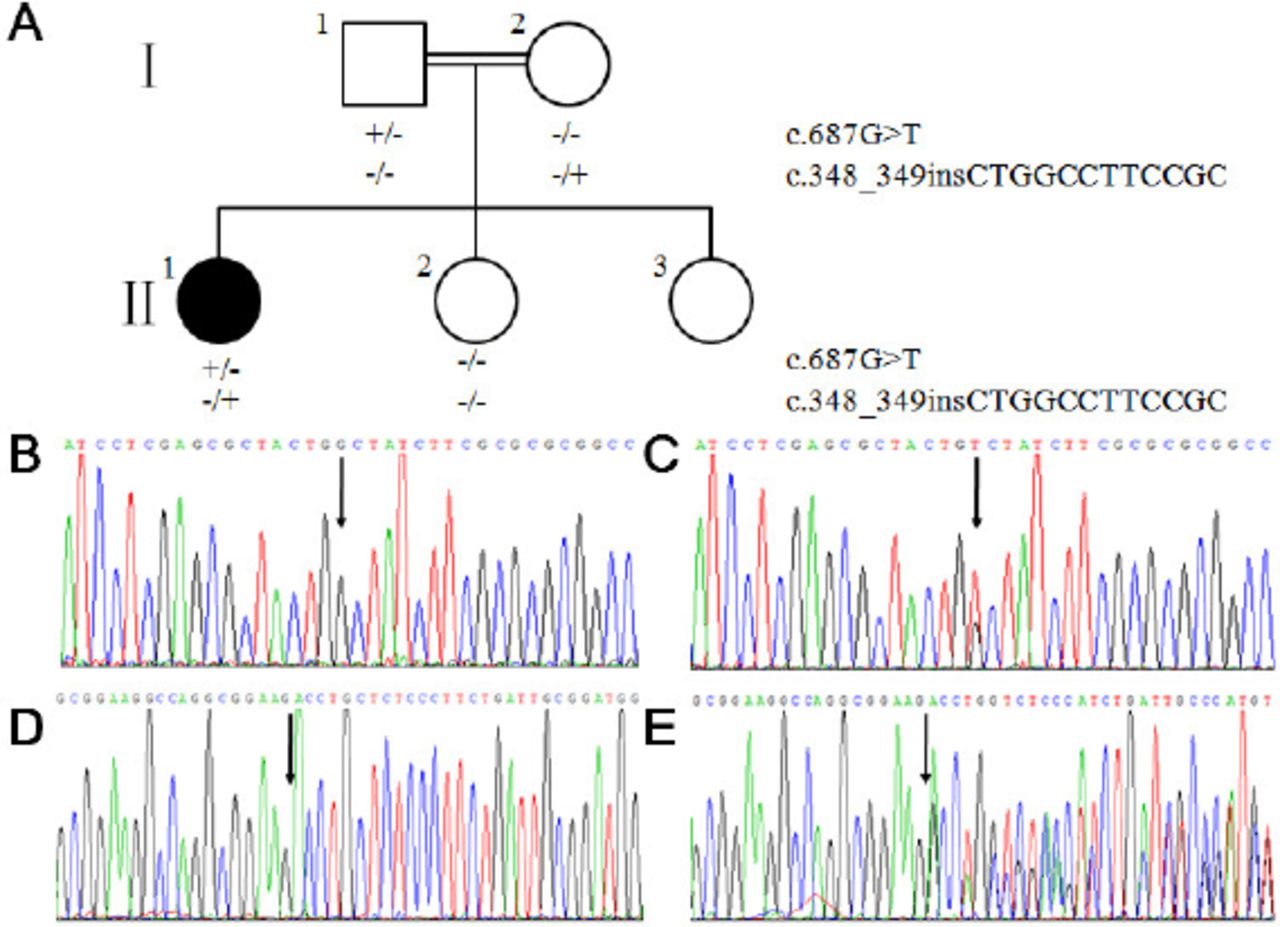
- Genetic analysis results for the patient and her family. A) The pedigree of the patient’s family with compound heterozygous MYORG mutations. B &D) Normal control sequences. C) The c.687G>T variant. E) The c.348_349insCTGGCCTTCCGC variant. Family members I:1 and II:1 were carriers of c.687G>T, and family members I:2 and II:1 were carriers of c.348_349insCTGGCCTTCCGC.
Clinical findings
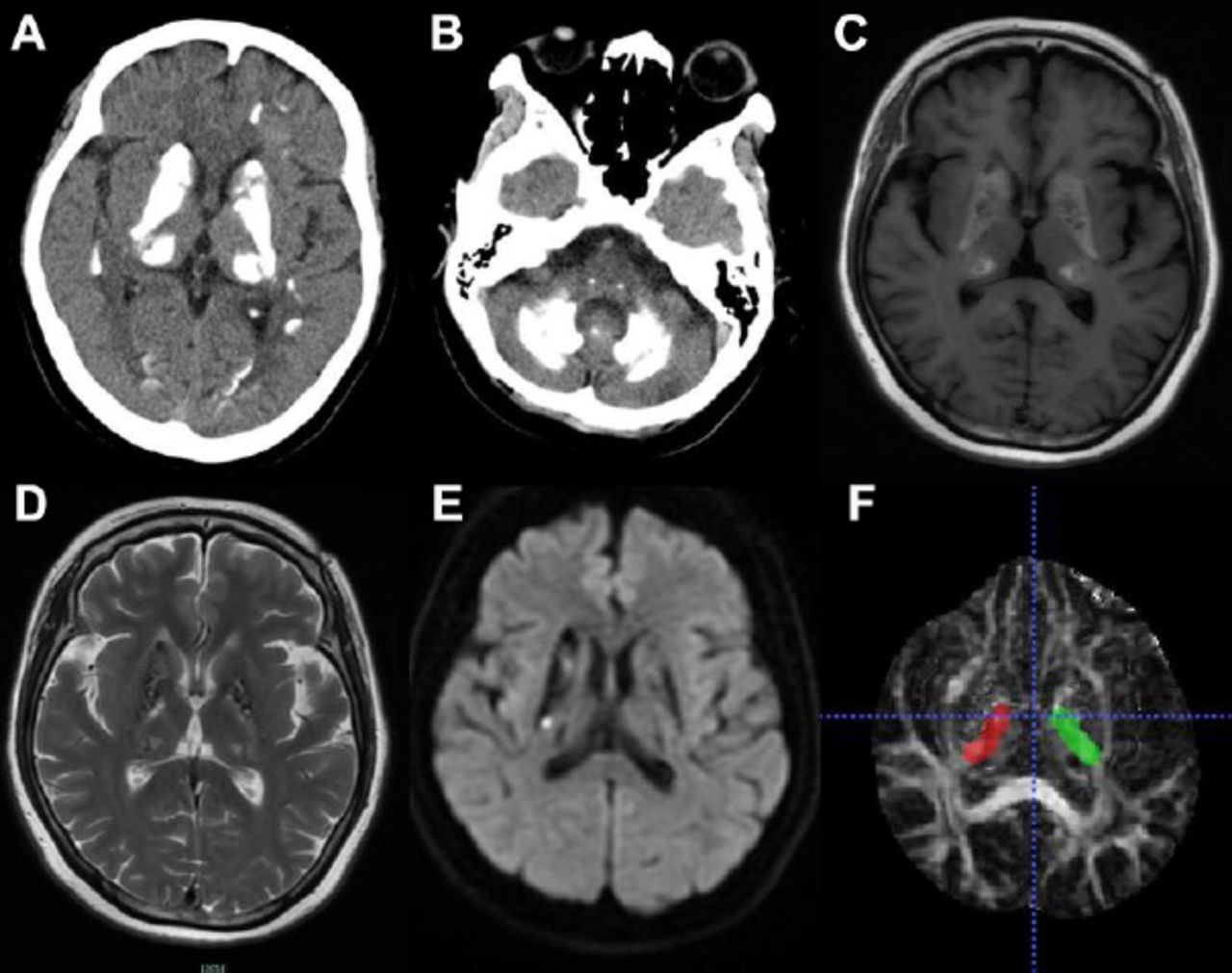
Neurological examination revealed hypomimia, bradykinesia, and festinating gait. Paroxysmal forced laughter or crying was also observed. Computed tomography (CT) and MRI imaging of her brain revealed severe calcification in the basal ganglia, thalamus, dentate nuclei, and subcortical white matter (Figure 2 A, B, C). The results of routine laboratory tests including blood sugar, HbA1c, lipid profile, erythrocyte sedimentation rate (ESR) and D2 dimers were unremarkable, and her serum calcium, calcitonin, thyroid hormone, and parathyroid hormone levels were normal. Based on these findings, other diseases that cause secondary intracranial calcification were ruled out.
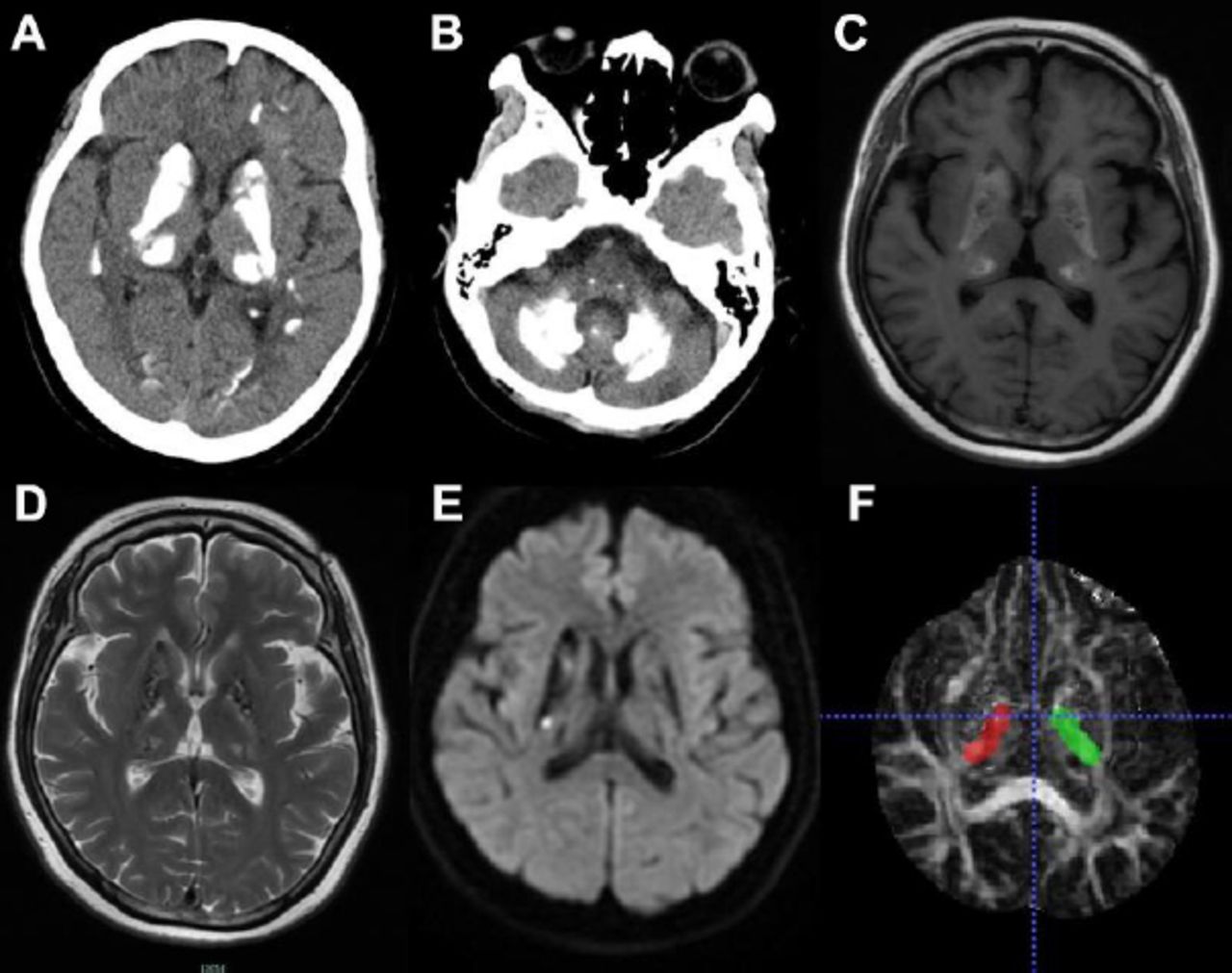
- Imaging findings from October 2018 and October 2019. Axial non-contrast CT (A & B) and MRI (C) scans of the brain taken in October 2018. Extensive symmetric calcifications can be observed in the bilateral basal ganglia, thalamus, dentate nuclei, and subcortical white matter. MRA (D) showed that there was no stenotic segment or occlusion in the intracranial arteries. DWI (E) of the brain taken in October 2019 showing hyperintense spots in the right internal capsule. DTI (F) showing the region of interest.
Diagnostic assessment
Her parents were in a consanguineous marriage. Neither her parents nor her younger sisters had experienced the same symptoms. We collected peripheral blood samples from the patient, her parents, and a sibling (II:1, I:1, I:2, and II:2) with their written informed consent. Genomic DNA was extracted using a standard method. Whole-exome sequencing was performed in the proband and revealed 2 previously described compound heterozygous mutations within the MYORG gene: c.687G>T (p.W229C) and c.348_349insCTGGCCTTCCGC (p.116_117insLAFR).4 She had inherited the c. 687G>T variant from her father and the c.348_349insCTGGCCTTCCGC variant from her mother (Figure 1 B, C, D, E). This variant was absent in 500 controls with normal chromosomes and was not included in the HGMD, Clinvar, ExAC, dbSNP, 1000G, and gnomAD databases. Then, the patient was considered as FD.
Therapeutic intervention
The patient was discharged with a prescription for oral levodopa and buspirone. At the time this manuscript was being prepared, we found that the clinical and genetic information of the family had been reported in February 2019.4 The ethical committee of the Fourth Affiliated Hospital, Zhejiang University School of Medicine, had approved of the study.
Follow-up and outcome
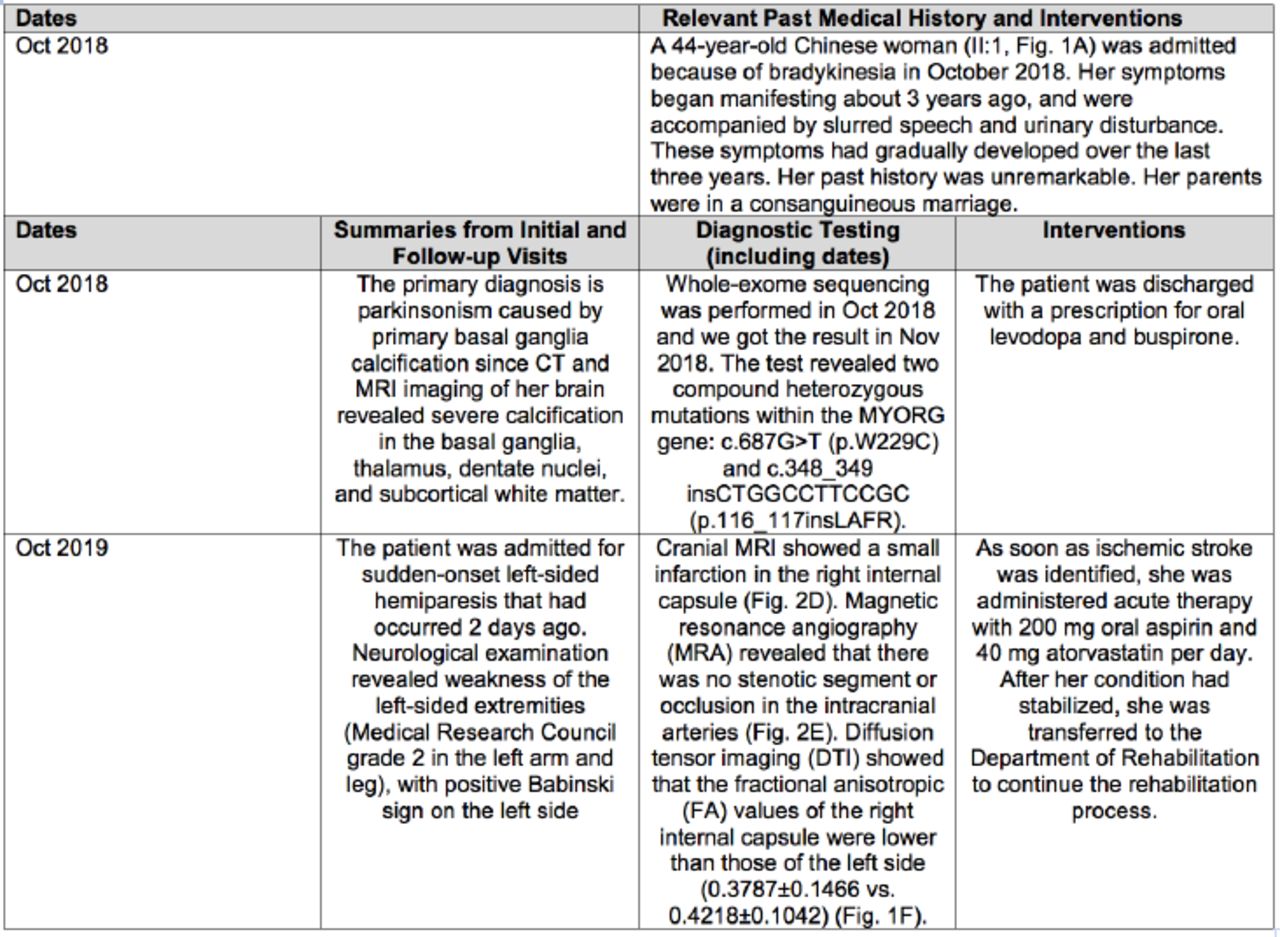
About one year after her last hospitalization in October 2019, the patient was admitted for sudden-onset left-sided hemiparesis that had occurred 2 days ago. Neurological examination revealed weakness of the left-sided extremities (Medical Research Council grade 2 in the left arm and leg), with positive Babinski sign on the left side. There were no changes in the results of the other neurological examinations compared with the results obtained during the previous hospitalization. Her brain CT findings were unremarkable, with the exception of severe calcification, and MRI showed a small infarction in the right internal capsule (Figure 2D). Magnetic resonance angiography (MRA) revealed that there was no stenotic segment or occlusion in the intracranial arteries (Figure 2E). Diffusion tensor imaging (DTI) showed that the fractional anisotropic (FA) values of the right internal capsule were lower than those of the left side (0.3787±0.1466 vs. 0.4218±0.1042) (Figure 1F). Routine laboratory tests, ambulatory blood pressure, dynamic electrocardiogram, heart ultrasound and CT angiography of neck were all normal. As soon as ischemic stroke was identified, she was administered acute therapy with 200 mg oral aspirin and 40 mg atorvastatin per day. After her condition had stabilized, she was transferred to the Department of Rehabilitation to continue the rehabilitation process. About 2 years after the stroke, the patient was still not able to ambulate independently (Medical Research Council grade 3 in the left arm and 4 in the left leg) (Figure 3).
- The timeline table of the case in this study.
Discussion
Only a few case reports have described acute ischemic stroke or transient ischemic attack-like episodes in FD,5-9 so this makes the findings in this case valuable in terms of prediction and management of stroke in patients with FD in the future.
Brain CT is a sensitive, economical, and rapid tool for detecting excessive intracranial calcification. The MRI using susceptibility-weighted imaging (SWI) is useful for detecting calcifications in FD patients, and some scholars have found that SWI can reveal calcium deposition in areas that cannot be observed by CT.5 In the present case, CT and MRI were adequate, as they revealed calcification patterns that are typical of FD. In addition, based on the other routine laboratory parameters, other causes of secondary calcification could be eliminated.
Former studies have identified only autosomal dominant FD, including those associated with mutations in the SLC20A2, PDGFRB, PDGFB, and XPR1 genes.1-3 In 2018, Yao et al1 reported the first gene responsible for a recessive FD—the MYORG gene. Recently, Cen et al2 identified biallelic mutations of the JAM2 gene in individuals with primary familial brain calcification. The present patient had 2 compound heterozygous mutations within the MYORG gene that have been described before.4 Therefore, the patient had a recessive form of FD. The typical parkinsonism and brain CT and MRI findings in this case were characteristic of FD, and genetic testing confirmed the diagnosis.
The association between ischemic stroke and FD has not been clearly determined. Former studies have shown that calcification is seen in the walls of capillary vessels, arterioles, and the perivascular space of FD patients, so this might represent a potential causative mechanism.10 For example, Nishimoto et al5 described a case of FD associated with cerebral micro-infarcts and found impaired cerebrovascular reactivity on SPECT with acetazolamide challenge in their patient.5 Based on these findings, they speculated that the decrease in vascular diastolic capacity associated with calcification might be one of the mechanisms. Further, Zhang et al9 reported a case of a 56-year-old man with an SLC20A2 mutation (c.C344T) who had melena for 6 days and somnolence for 3 days. Blood examination showed anemia, indicated by a hemoglobin level of 73 g/L. Cranial MRI revealed bilateral acute ischemic stroke, and hypoperfusion was assumed. Grangeon et al. reported a case with compound heterozygous mutations (c.C1427A and c.T1967C) of the MYORG gene associated with a stroke-like episode but no MRI changes.6 In contrast, another patient with homozygous MYORG gene mutations (c.G191A) had both stroke and MRI changes.6 Malaquias et al7 reported three FD patients with MYORG gene mutations who presented with episodes of acute hemiparesis without any evident MRI changes.Based on the location and diameter of the infarct lesion in DWI and the normal MRA findings in the present case, we classified the infarct as a small-artery occlusion. However, we did not identify any risk factors of arteriosclerosis. In addition, based on the SWI findings and normal results of immunological tests, the possibility of cerebral amyloid angiopathy and immunologically related small vessel disease was excluded. Therefore, we postulated that the small-artery occlusion in our patient was caused by extensive calcium and mineral deposition in affected vessels because of FD. However, further investigation is needed to confirm this hypothesis. Currently, it is not clear whether stroke caused by FD requires different therapeutic approaches from stroke caused by atherosclerosis, and this requires further investigation in the future.
Interestingly, ischemic stroke did not cause severe symptoms or poor recovery in the present patient. This mismatch between the ischemic stroke lesion and clinical severity was confusing, so DTI was performed. The FA values of both sides of the internal capsule were lower than those in normal individuals. Based on this finding, it is possible that the corticospinal tract may have been damaged by calcium deposits that had not been detected at the first examination conducted before the episode of stroke. Further follow-up is needed to confirm this hypothesis.
In conclusion, based on the findings, it is possible that extensive calcium deposits in affected vessels might lead to small-artery occlusion, and subsequently, ischemic stroke. Further study is required to elucidate the relationship between FD and ischemic stroke, as well as the treatment approach for these patients.
Acknowledgement
We are thankful to the patient for providing her consent for the publication of this case report. We appreciate the technical support from Mrs. Ying Liu and the clarity and correctness of Figure 2 from Dr. Sheng Hu. We would like to thank ELIXIGEN Company for English language editing.
Footnotes
Disclosure. This work was funded by the Major Health Science and Technology Program of Zhejiang Province, Zhejiang, China (grant no. WKJ-ZJ-2208).
- Received April 24, 2022.
- Accepted August 2, 2022.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.