


Article Figures & Data
Figures
- Figure 1
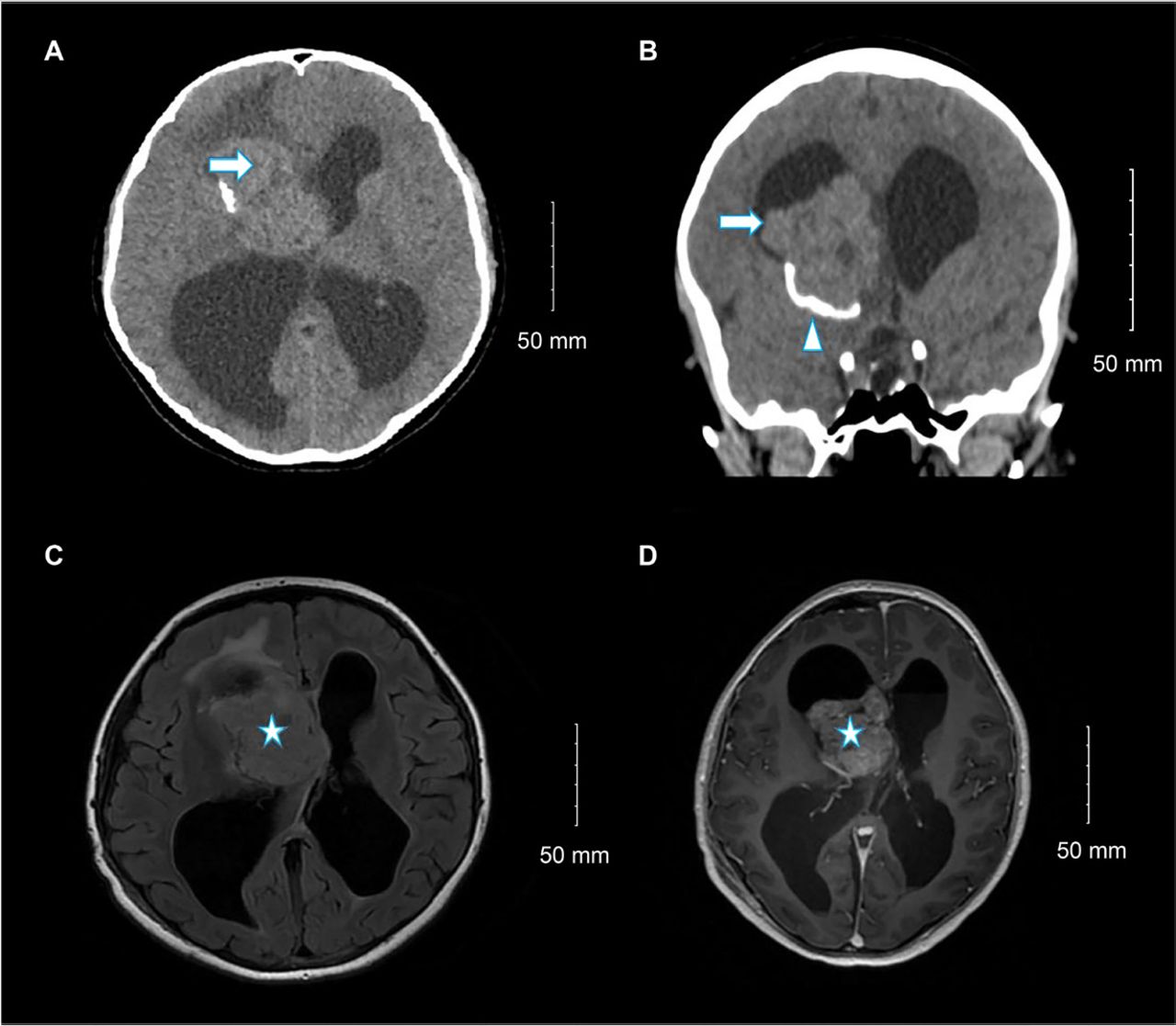
- Selected (A) axial and (B) coronal images of unenhanced brain computed tomography show a large right lateral ventricle frontal horn dense mass (arrow) associated with peripheral calcification (arrowhead) causing marked hydrocephalus. Selected (C) axial fluid-attenuated inversion recovery and (D) axial T1 post-contrast brain magnetic resonance imaging show large, well-defined, lobulated intraventricular mass lesions within the right lateral ventricle at the region of foramen of Monro with heterogeneous moderate enhancement (star) and hydrocephalus.
- Figure 2
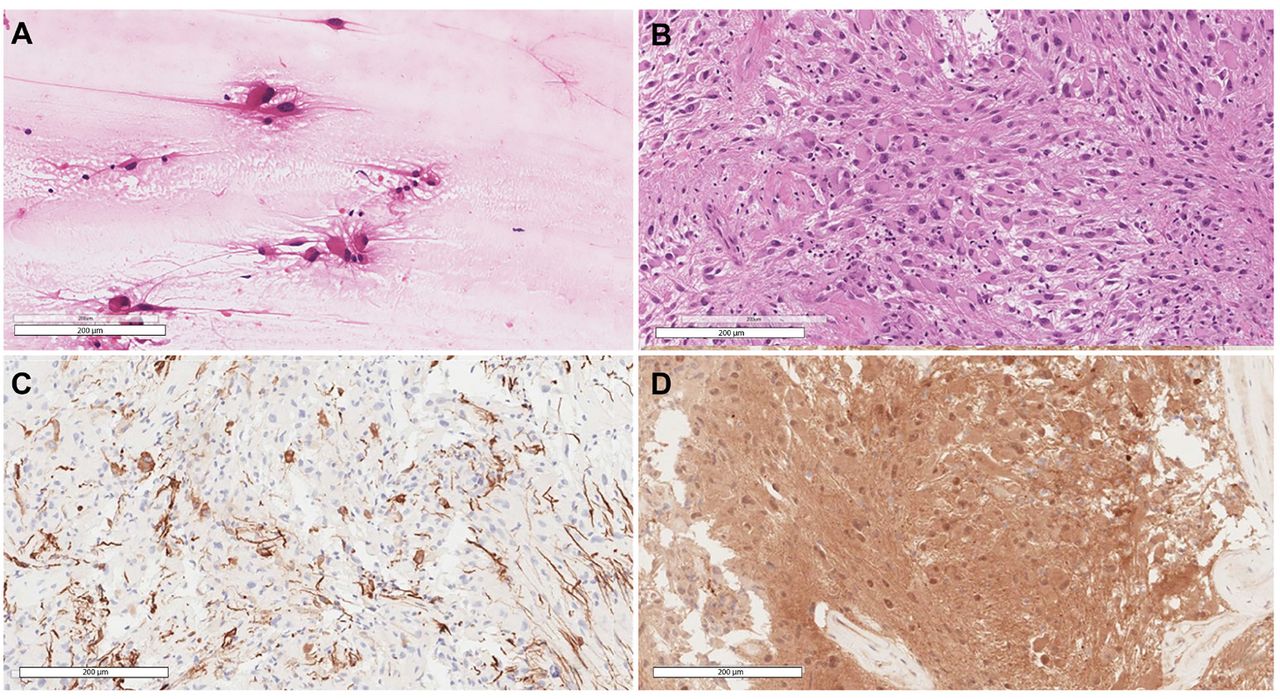
- Selected views of A) Smear slide at 20× showing the large eosinophilic tumor cells with processes emanating from them. B) Hematoxylin and eosin-stained section at 20× power reveals the classic histomorphology of subependymal giant cell astrocytoma with some of the cells showing well-defined borders while others show elongated cytoplasmic processes. C) Glial fibrillary acidic protein stain highlighting scattered positive tumor cells. D) Positive immunohistochemical staining for S100.
- Figure 3
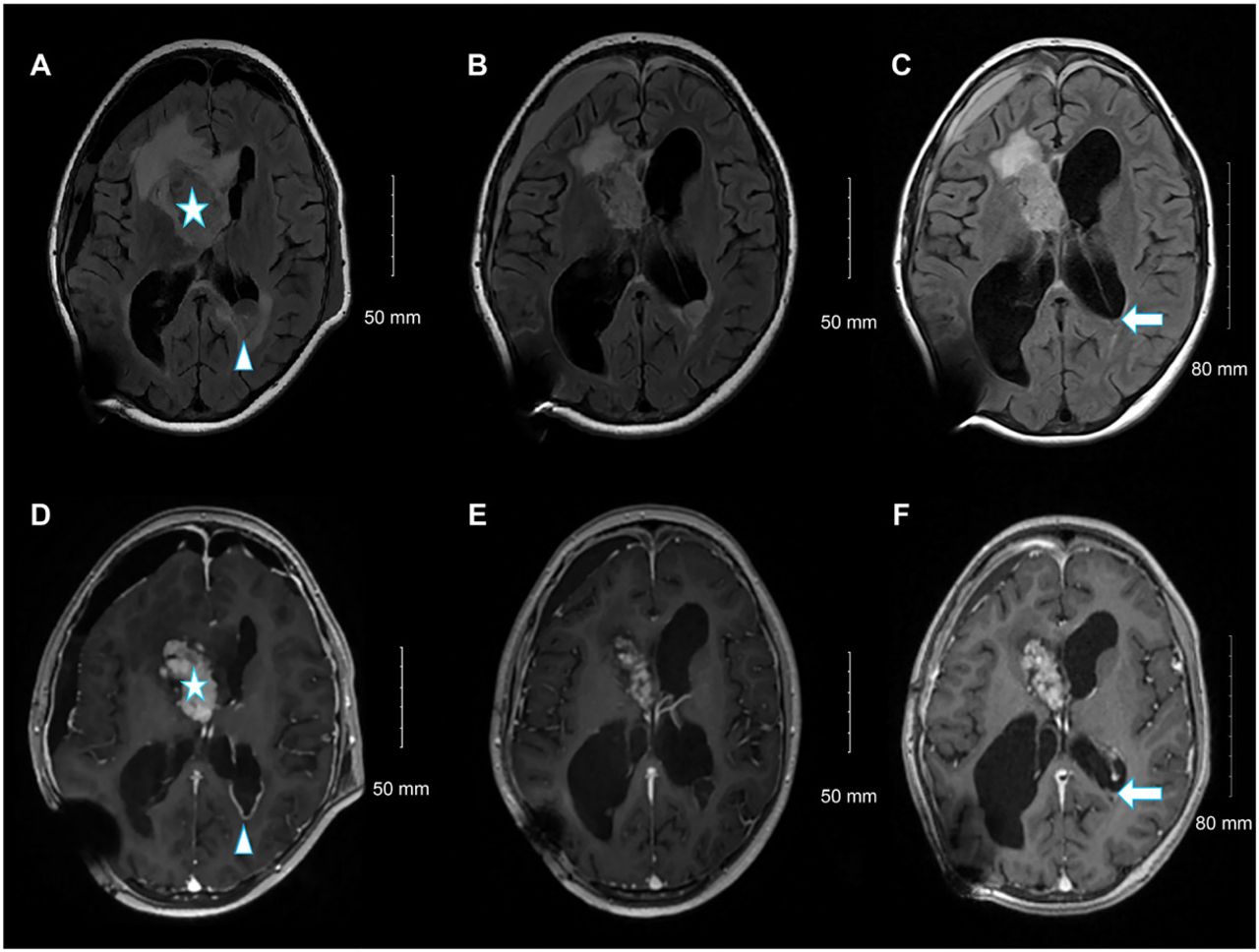
- From left to right, selected fluid-attenuated inversion recovery magnetic resonance images (A, C, and E), and selected axial T1 post-contrast images at the same level (B, D, and F). Upon admission (A, B), the residual heterogeneously enhanced the right lateral ventricle frontal horn component (star). A new left occipital ependymal/subependymal nodule with peripheral enhancement (arrowhead) is visible. Follow-up examination at 3 months (C, D) revealed an interval reduction in the size of the left occipital ependymal/subependymal nodule, with peripheral enhancement. Follow-up examinations at 6 months (E, F) showed a further reduction in the size of the left occipital ependymal/subependymal nodule (arrow).



Tables
Dates Relevant past medical history and interventions 6 months earlier Intermittent morning headaches with on/off nausea and vomiting over six months diagnosed as sinusitis in a private clinic Date Summaries from initial and follow-up visits Diagnostic testing (including dates) Interventions 23 Mar 2022 Presented to emergency department with increasing early morning headaches with nausea and vomiting over last one month. Physical examination revealed decreased sensation in the left V2 maxillary branch of the trigeminal nerve. Also bilateral papilledema and optic disc pallor. Otherwise, intact power, other sensations, and no cerebellar signs. Eye ultrasound showed 10 mm optic sheath diameter Non-contrast brain computed tomography (CT) demonstrated active hydrocephalus and right lateral ventricular mass with associated calcification Dexamethasone 8 mg STAT then 4 mg q6hrs 24 Mar 2022 Patient was admitted to pediatric intensive care unit (PICU) in stable condition MRI revealed a heterogeneously enhancing well-defined right lateral intraventricular mass measuring 6×5.3×3.3 cm. Emergency right septostomy with insertion of external ventricular drain (EVD) 30 Mar 2022 Patient intubated and ventilated after surgery. The preoperative symptoms markedly improved after tumor debulking, however, she developed three episodes of tonic-clonic seizures. Pathological diagnosis is subependymal giant cell astrocytoma Tumor genomic analysis showed pathogenic TSC2 mutation No clinical or radiological TSC stigmata Right frontal craniotomy and maximum safety resection of about 70% of the intraventricular tumor Levetiracetam 500 mg BID 12 Apr 2022 Patient extubated successfully but found to have buccofascial apraxia and mild left sided weakness which improved a lot with PT and OT White blood cell count in the cerebrospinal fluid normalized after 2 weeks of broad spectrum antibiotics High white blood cell count in the cerebrospinal fluid without clinical signs of infection Broad spectrum antibiotics for two weeks Removal of EVD and insertion of right occipital ventriculoperitoneal (VP) shunt 21 Apr 2022 Discharged in good condition with no deficits 19 May 2022 Re-admitted for evacuation of post-operative subdural hemorrhage. Patient complained of headache and facial asymmetry MRI brain revealed stable residual tumor but there was a new left occipital subependymal 2.7 cm nodule with peripheral enhancement Everolimus (mTOR inhibitor) was administered at a starting dose of 4.5 mg/m2 per day then increased to 5 mg daily for two weeks, followed by a further increase to 7.5 mg daily 4 Sep 2022 Outpatient visit The patient was asymptomatic and reported no adverse effects Follow-up brain MRIs at three and six months intervals showed a reduction in the residual tumor size and occipital nodule Continue Everolimus treatement until it fails or the side effects become intolerable
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.