


Abstract
Leptomeningeal cysts, which are cystic collections filled with cerebrospinal fluid, are rare complications following pediatric head trauma and surgical correction of craniosynostosis. These cysts develop due to cerebrospinal fluid pulsations and brain growth that cause expansion of the dural tears. Although primary repair of the dural defect is the definitive treatment, the risk of cyst recurrence remains. Factors that increase this risk include syndromic craniosynostosis, hydrocephalus, increased intracranial pressure, and inadequate duraplasty/cranioplasty. Here, we report the successful treatment of a child with a complex leptomeningeal cyst on one hemisphere, Crouzon syndrome, and hydrocephalus who showed no cyst recurrence over 2 years of follow-up. We have also reviewed the literature for predictors of post-repair cyst recurrence and preventive surgical techniques in patients with high risk of recurrence.
Leptomeningeal cysts are cerebrospinal fluid (CSF)-containing cysts that develop after traumatic dural tear. They develop due to the normal physiological CSF pulsations and brain growth rather than an increase in the intracranial pressure (ICP) and may be accompanied by gliotic brain tissue. The most common cause of leptomeningeal cysts is trauma, particularly in<1-year-old children in whom these cysts develop due to the rapidly growing brain.1 Other identified causes are craniofacial surgery and craniosynostosis reconstruction, including simple suturectomy and extensive calvarial vault remodeling.2 Recently, endoscopic repair has also been reported as a cause of leptomeningeal cysts.3 Three pathophysiological conditions associated with its formation after craniosynostosis repair have been identified: dural tear, deficient overlying bone, and pulsatile growing brain.4 Primary treatment for small-to-moderate-sized cysts involves exposure of the entire dural defect, followed by dural closure with/without duraplasty and cranioplasty overlying the defect. Here we present a case of a leptomeningeal cyst that was successfully treated as well as a literature review on the predictors of leptomeningeal cyst formation and recurrence after craniosynostosis reconstruction with technical notes.
Case Report
Patient information
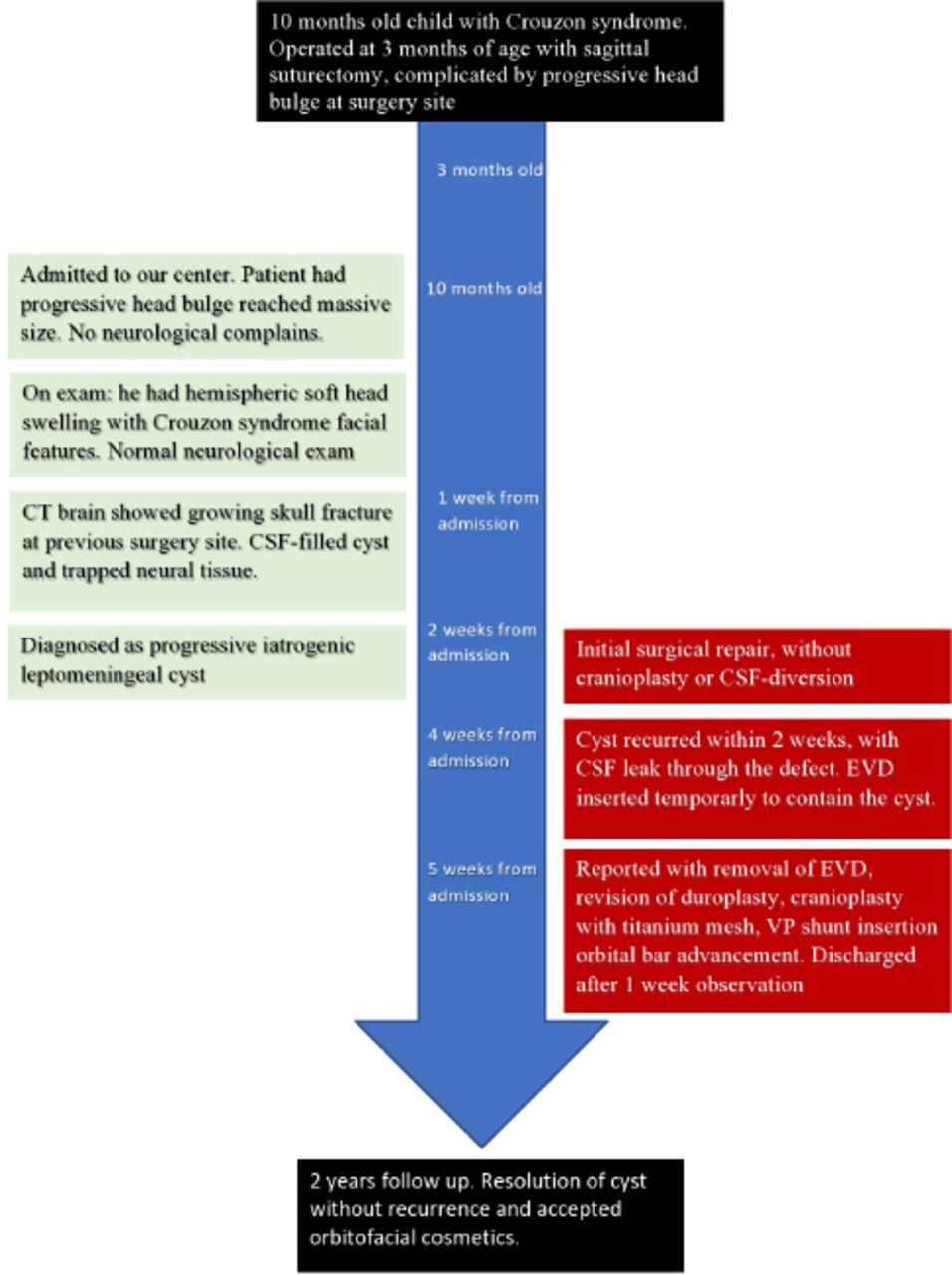
We are reporting a unique case of traumatic leptomeningeal cyst after consenting the patient’s family. A 10-month-old male infant diagnosed with Crouzon syndrome and bilateral coronal craniosynostosis was referred to our neurosurgery center because of a large progressive bulge on his head after suturectomy that was performed in another center at 3 months of age. Initial surgery was uneventful except for the bulge formation that was noticed postoperatively (Figure 1). The patient had a small-sized cyst and was kept under observation without surgery. The cyst increased to a huge size on the entire right cerebral hemisphere, but the patient was completely asymptomatic, with no symptom of increased ICP or pain (Figure 2).

Frontal view of the patient showing typical Crouzon facies with swelling emerging from the vertex.

Timeline showing the chronological presentation, management and outcome of the patient.
Clinical findings
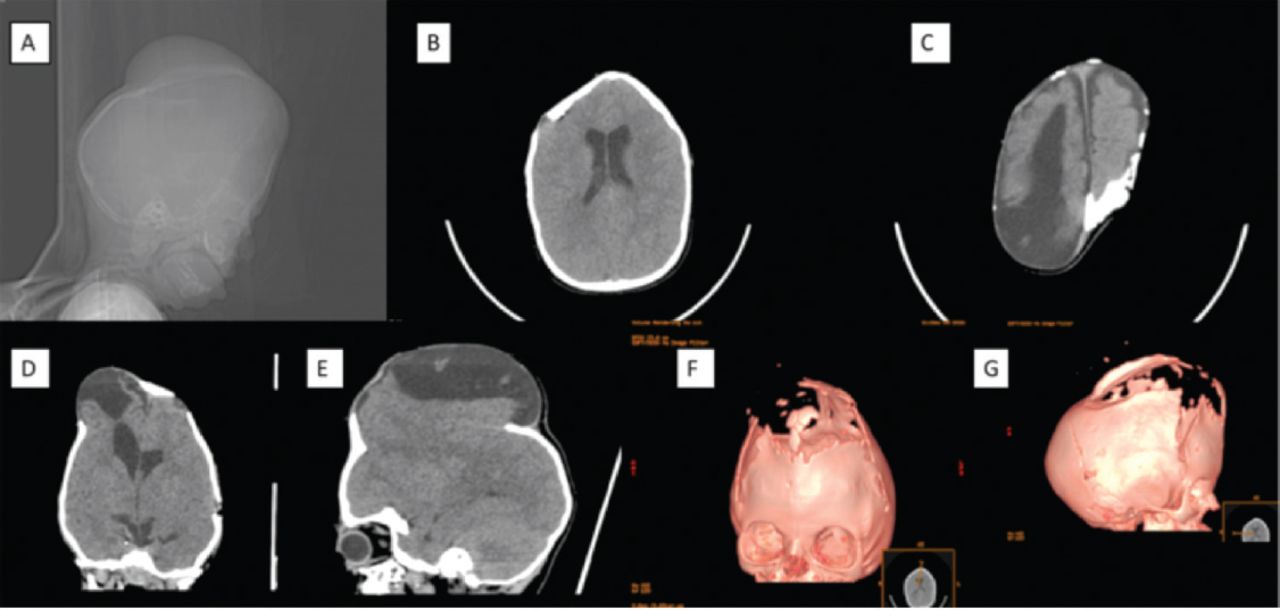
Examination findings were unremarkable, except for Crouzon features with a mild delay in developmental milestones but no major neurological deficits. Computed tomography scan of the brain showed a large bone defect in the right fronto-temporo-parieto-occipital region with brain parenchyma herniation and subgaleal CSF collection without ventriculomegaly (Figure 3).
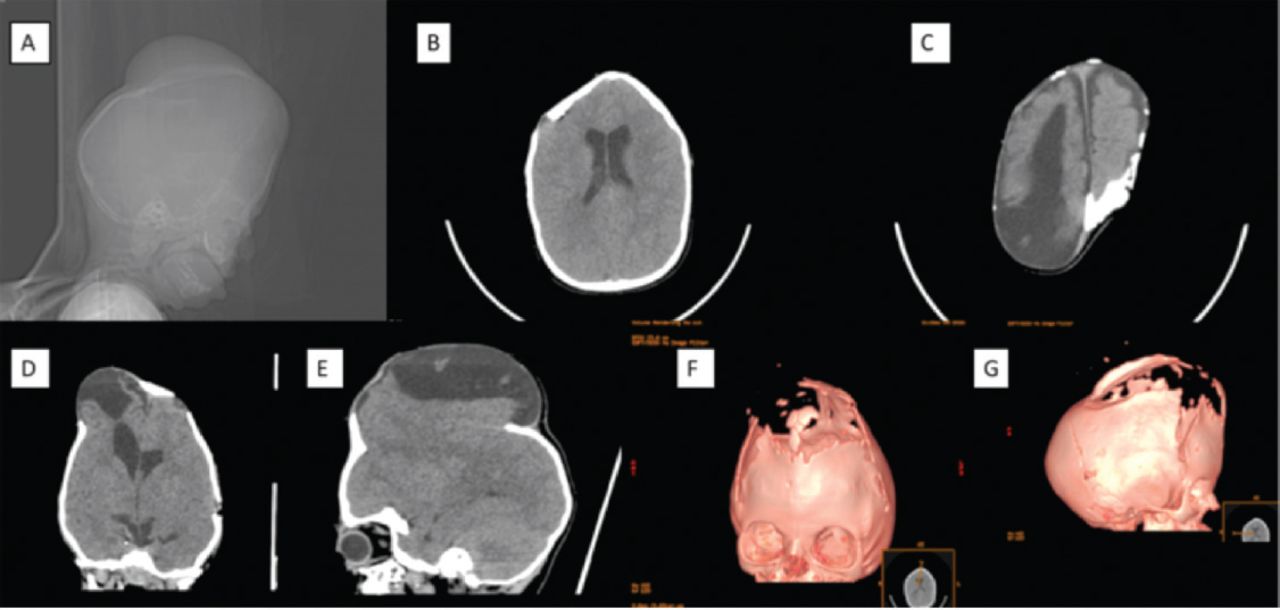
Pre Operative CT brain without contrast: (A) scout image showed large extra-cranial swelling with features of bicoronal cynostosis. (B) Axial view showed tight brain with trigonocephaly. (C) upper cut with leptomeningial cyst (D&E) coronal & Sagital view showed large leptomeningeal cyst with brain herniation. (F&G) 3D images with signs of craniocynostosis and bone remodeling after the suturectomy.
Therapeutic intervention
The patient underwent surgery for dural defect repair in our institute. Briefly, a large curvilinear incision was made over the medial bone margin to expose the entire defect. Upward elevation of bone edges was noticed, indicating the outward driving force of the growing brain and pulsating CSF. The dural defect was identified laterally, anteriorly, and posteriorly. However, because the defect was large, the medial dural edges under the bone near the superior sagittal sinus could not be evaluated. Gliotic brain tissue was resected, and everted bone edges were shaved with a drilling burr. Dural substitute was inserted bilaterally under the dural edges. Cranioplasty was planned as a future surgery after the swelling decreased. Skin was sutured in a continuous fashion. Postoperative reduction in the bulge size was observed, but fluid collection accompanied by cyst recurrence was noted during follow-up (Figure 4). Therefore, total cranial remodeling was performed, and ventriculoperitoneal (VP) shunt was inserted. The patient was suspected of harboring hydrocephalus, which likely contributed to the initial bulge and rapid cyst recurrence. Duraplasty was reinforced, and a titanium mesh was placed over the defect. Orbital bar advancement was also performed in the same surgery (Figure 5).
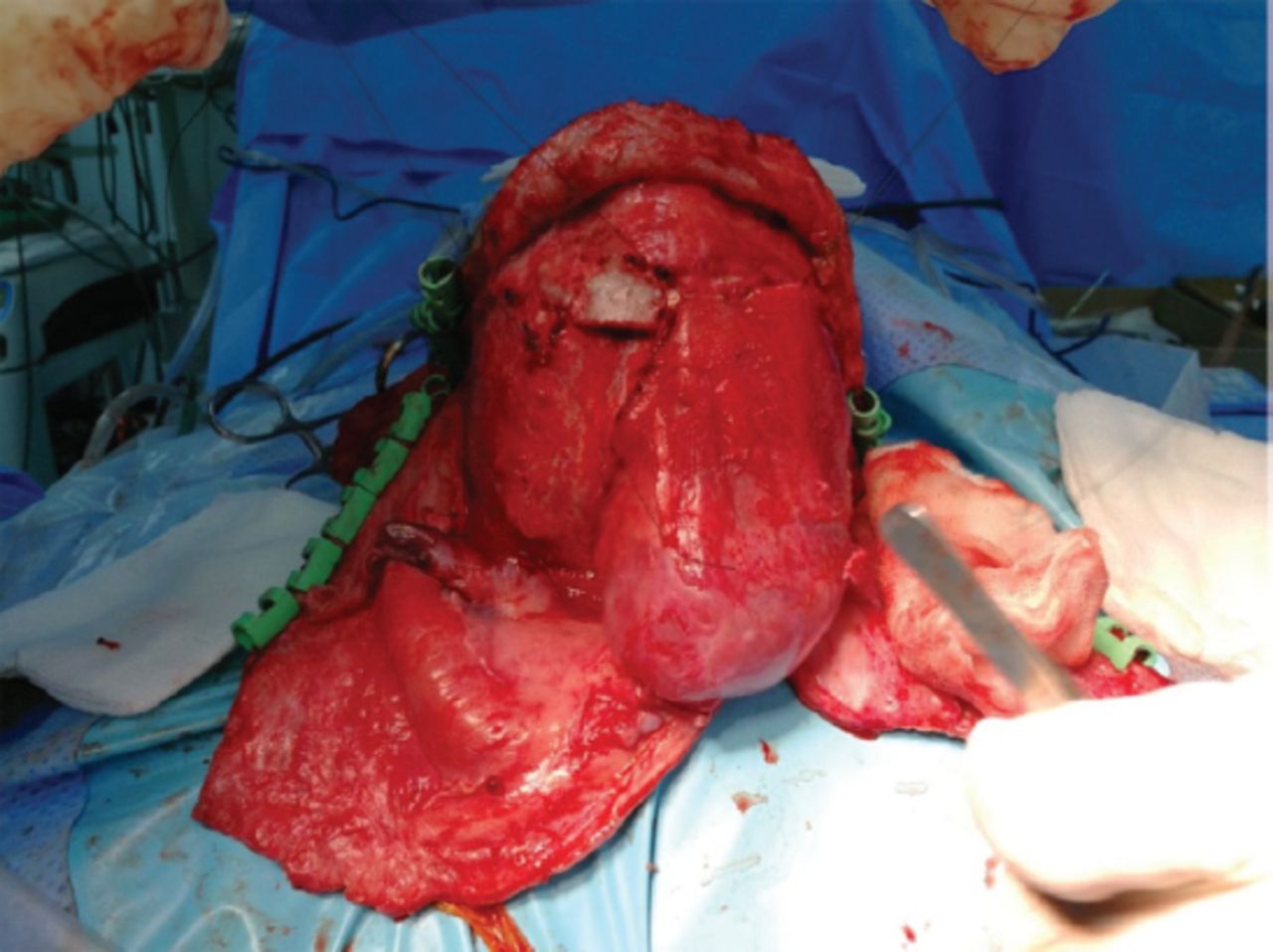
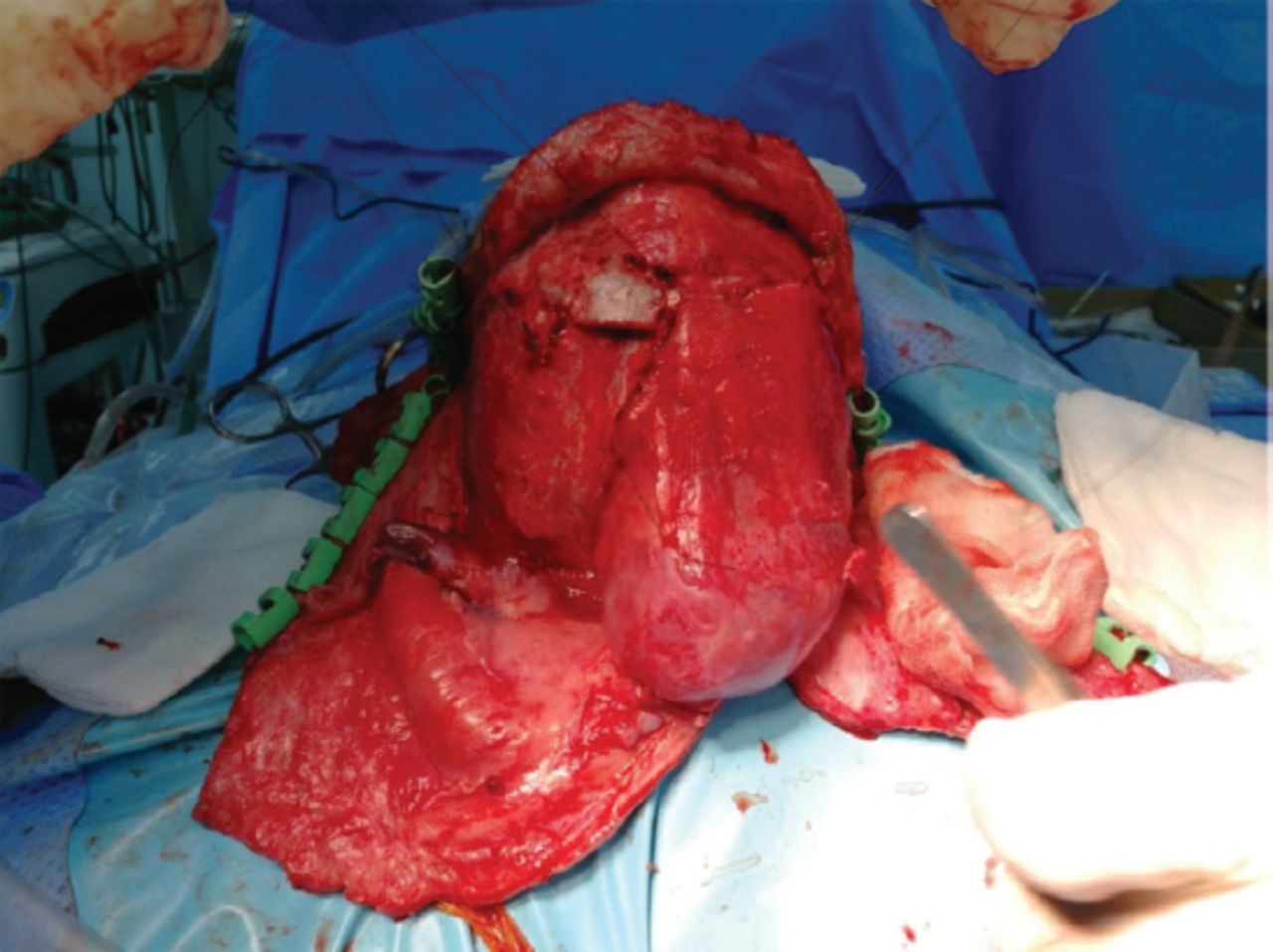
Intraoperative picture of the second repair showing the recurrent cyst with dural substitute overlying the defect. The cyst recurred with adequate duroplasy.
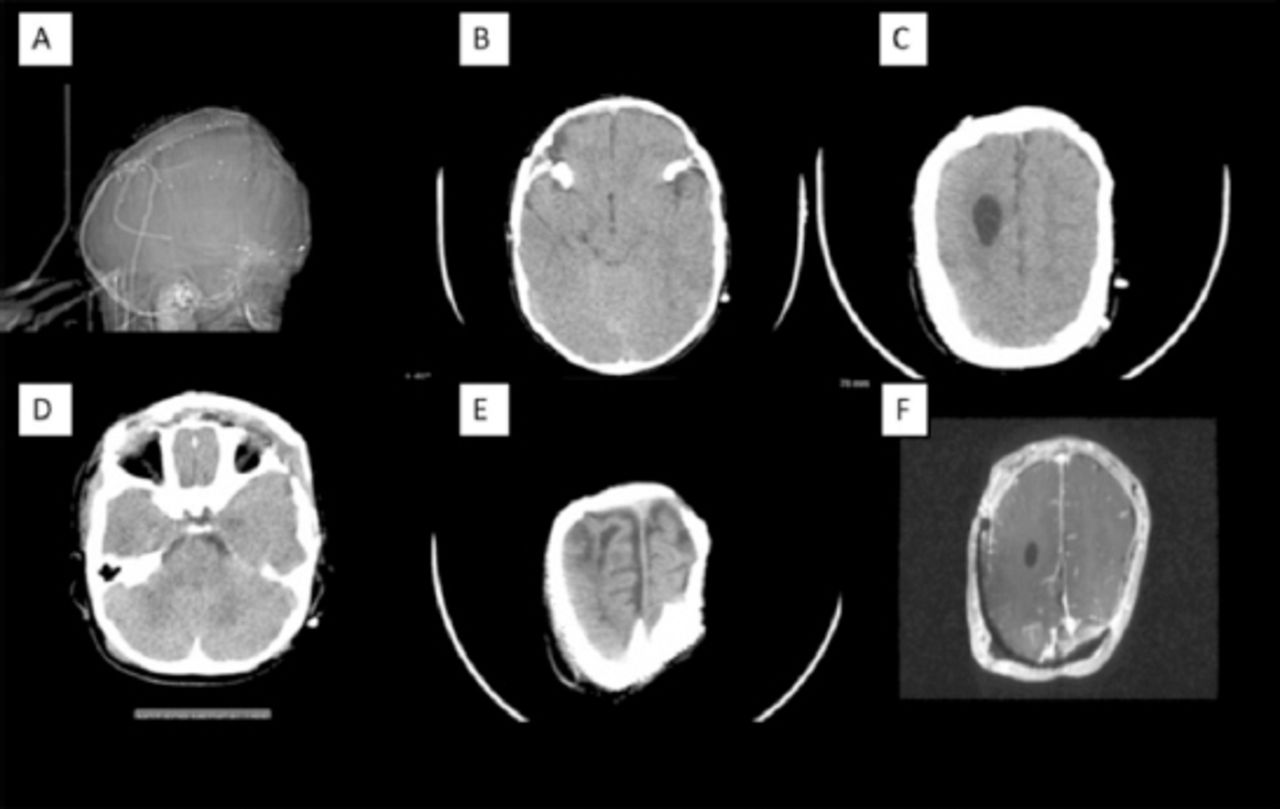
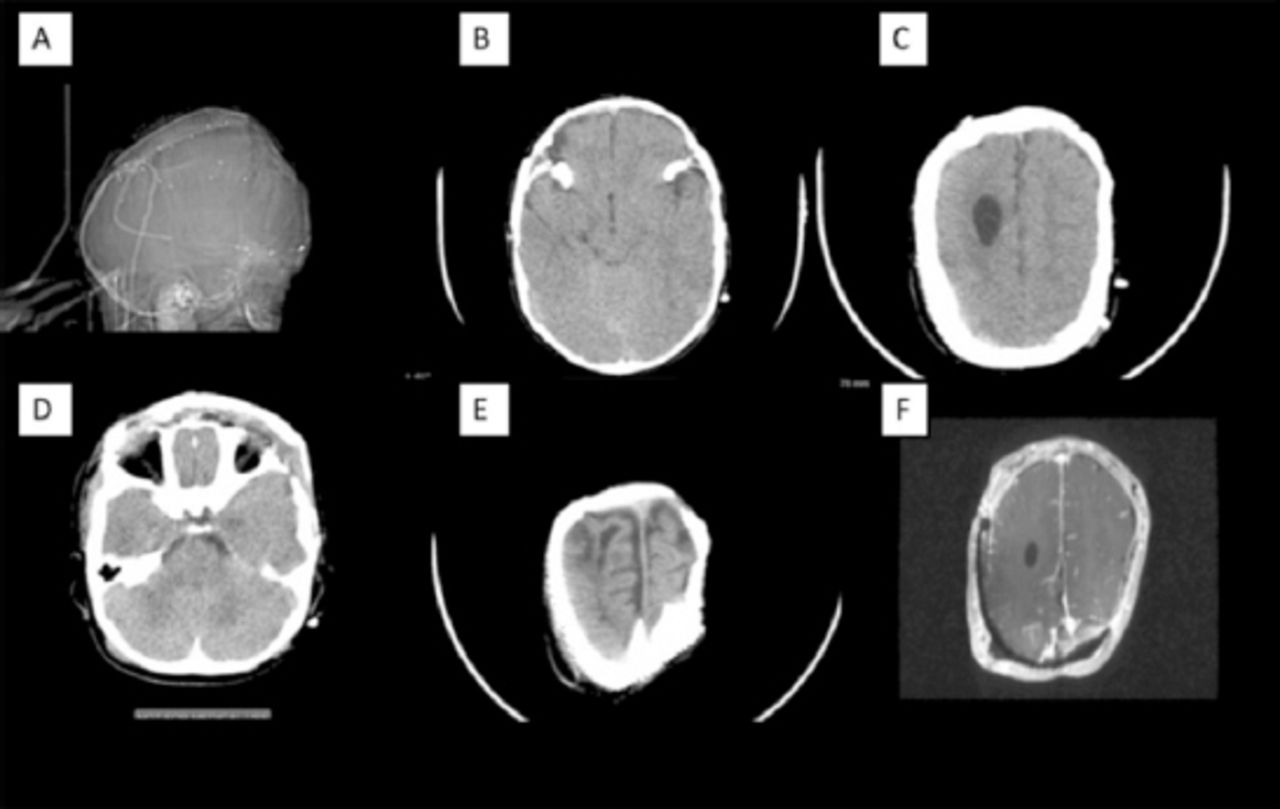
Post operative imaging: (A) Scaut image showed fronto-orpital advancement with cranioplasty and Mish repair as well as disappear of extra-cranial collection. (B, C&D) Axial view showed brain relax after fronto-orbital advancement and trigonocephaly repair (E) Upper cut after leptomeningial cys resection and cranioplasty. (F) MRI brain with contrast showed duraplasty without signs of cyst collection.
Follow ups and outcomes
Postoperatively, the wound healed, and the family were satisfied with the fronto-orbital appearance of the patient. Head swelling disappeared after applying the mesh. The patient was neurologically intact postoperatively and showed no cyst recurrence over 2 years of follow-up (Figure 6).

Photo taken few months after discharge showing the cosmetic result of orbital bar advancement and the disappearance of the swelling without recurrence.
Discussion
Leptomeningeal cysts, which are associated with dural laceration, commonly occur after skull fractures and reconstructive craniofacial surgeries. If the dural defect is left unrepaired, it may lead to brain herniation, headache, increased skull swelling, and seizures.5,6 However, the risk of cyst recurrence (2%) after surgical repair remains.7 Zemann et al reviewed 14 patients who developed these cysts after craniosynostosis repair and identified multiple risk factors for cyst development following intraoperative dural lacerations; these include clinical or radiological signs of increased ICP, coronal craniosynostosis, syndromic craniosynostosis, repeated surgical interventions, and endoscopic repair.4 Seven of their 14 patients had coronal craniosynostosis. Mannitol can be used in initial craniosynostosis repair to achieve brain relaxation and avoid damage to the dura.4 In our present case, all factors for cyst development, except endoscopic repair, were present. Coronal synostosis repair is reportedly a major risk factor in pediatric patients.4,8 Interestingly, the cyst in our patients increased to a huge size without causing any major neurological deficits. This supports the significance of intraoperative identification of dural injury, followed by its early repair, which is proven to be most effective for preventing future cyst formation.8 Multiple surgical repair techniques have been described. For instance, a skin incision large enough to expose the entire bony defect and allow dural closure without tension should be made, followed by the identification of retracted dura under the bone and duraplasty with pericranial or fascia lata graft as a synthetic dural substitute. In most cases, primary dural closure is impossible due to retraction of the dura under bone edges.8 In the present case, we used a non-suturable dural substitute to slide under the medial bony margin as the dura under the superior sagittal sinus could not be visualized because of limited exposure. Herniated brain tissue resection should be avoided unless the tissue is abnormal/gliotic and its resection may not cause any deficits. In our case, the tissue was intraoperatively confirmed to be nonfunctional, and its resection caused no noticeable deficits postoperatively. Managing high ICP in such patients is crucial to prevent cyst recurrence. Increased ICP can be surgically managed by resecting herniated brain tissue and treating hydrocephalus. Delayed repair, namely, repair only after herniated brain tissue is visible on brain imaging, is advised. It is suggested to delay repair until the edema resolves and brain tissue retracts from the defect. However, resection of the nonfunctional tissue is necessary if the herniated tissue persists despite adequate observation, which is typically 2 months. After this period, the cyst is unlikely to regress spontaneously and will continue to expand without surgical treatment.7 Ventriculoperitoneal (VP) shunting in such patients is advised if they show signs of high ICP or external hydrocephalus, as performed in our case.4 This is particularly important as a reinforcement as the dural repair may fail to contain the cyst with hydrocephalus. In fact, CSF diversion alone can successfully treat recurrent leptomeningeal cysts in patients with hydrocephalus.9 Cranioplasty should ideally be performed with a bone graft fixed with rigid absorbable screws and plates or absorbable sutures, and a split-thickness graft is also an acceptable option.2 In the present case, these options were not feasible due to unavailability of absorbable mesh in our institute and the presence of the large bony defect. We performed only duraplasty and skin closure initially and planned to perform craniosynostosis reconstruction in the future. These techniques with appropriate skin closure were insufficient to effectively contain the cyst, thus leading to cyst regrowth and CSF leakage through the wound. Increased ICP and skipped cranioplasty could be the main reasons for quick cyst recurrence. These issues were addressed in the subsequent surgery with the insertion of VP shunt, implantation of standard temporary titanium mesh over the defect, and orbital bar advancement. These techniques sufficiently sealed the defect and effectively prevented cyst recurrence. The titanium mesh used was temporary; therefore, a future cranioplasty is needed for appropriate skull growth. Initial placement of absorbable material has the benefit of allowing appropriate cranial remodeling with skull growth; however, this technique may increase the risk of cyst recurrence in patients <3 years old; using temporary rigid material or postoperative helmet may decrease this risk.10 The main surgical repair steps needed to prevent cyst recurrence are as follows: full exposure of dural defect, duraplasty, cranioplasty, and management of increased ICP with CSF diversion if needed. Aggressive treatment from the beginning to address all factors that may lead to future cyst recurrence is required in selected patients.
In conclusion, leptomeningeal cysts are rare complications following craniofacial surgery. Early recognition and repair are indispensable regardless of the initial cyst size to avoid potential neurological complications and continuous increase in swelling to a size that may complicate surgical correction. Ventriculoperitoneal shunting in patients with high ICP and cranioplasty in all such patients is required to avoid cyst recurrence. Observation without surgery may lead to increased swelling, especially in patients with high ICP that goes unidentified in the initial repair attempt.
Case Reports
Case reports will only be considered for unusual topics that add something new to the literature. All Case Reports should include at least one figure. Written informed consent for publication must accompany any photograph in which the subject can be identified. Figures should be submitted with a 300 dpi resolution when submitting electronically. The abstract should be unstructured, and the introductory section should always include the objective and reason why the author is presenting this particular case. References should be up to date, preferably not exceeding 15.
Footnotes
Disclosure. The authors declare no conflicting interests, support or funding from any drug company.
- Received June 11, 2018.
- Accepted July 4, 2018.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.