


Abstract
It is estimated that 6.6%-9.3% of stroke patients have unruptured cerebral aneurysms. The safety of recombinant tissue plasminogen activator (r-tPA) for stroke patients with these aneurysms is uncertain. We report the case of a 58-year old male presented with an acute ischemic stroke within 2 hours of symptom onset and was treated with r-tPA. Further investigation showed that the patient had 2 unruptured cerebral aneurysms. He recovered completely from the stroke and was discharged home in a few days with no deficits. Although cerebral aneurysms are considered a relative contraindication for r-tPA, our case provides evidence that it can be safely administered to these patients.
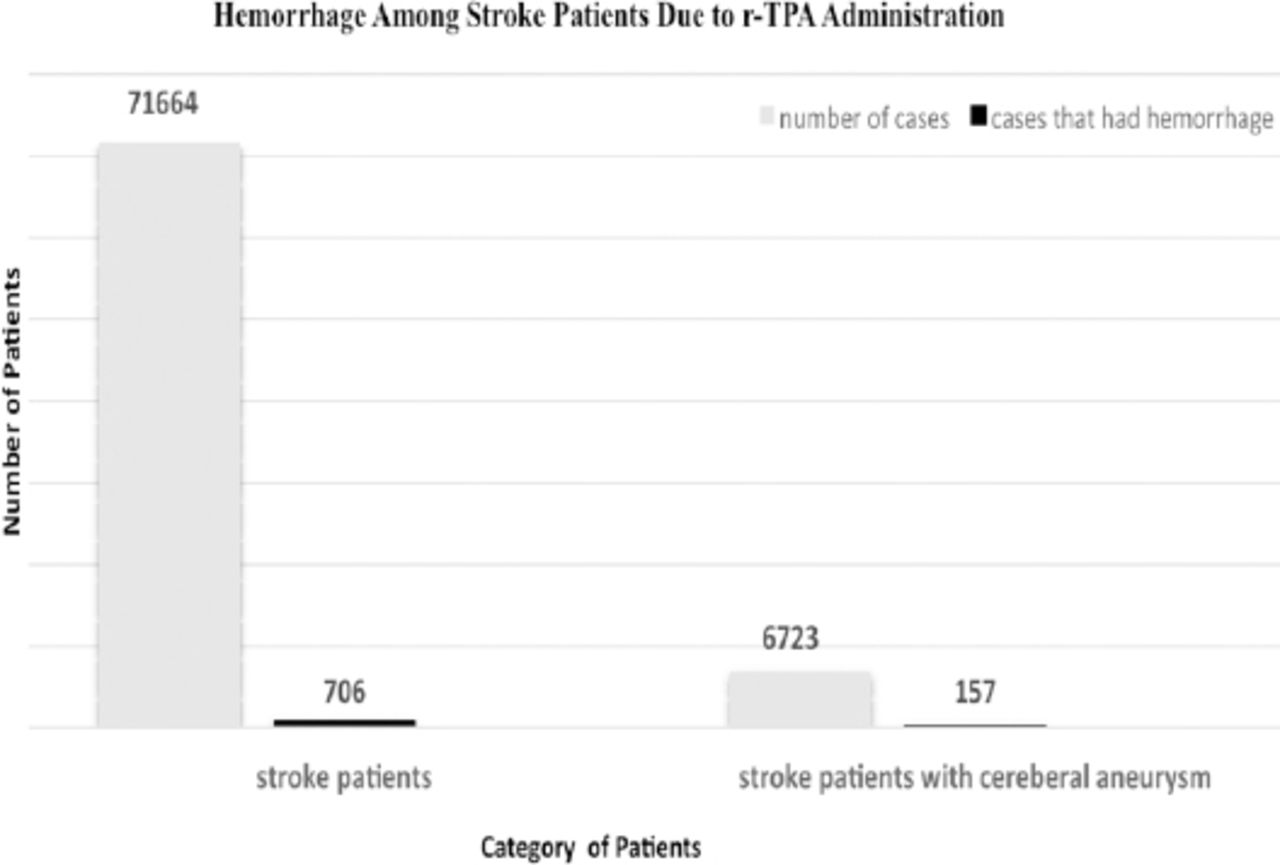
The use of thrombolytic agents in treating stroke patients with incidental cerebral aneurysms is controversial. The number of stroke patients described as having unruptured intracranial aneurysms ranges from 6.6-9.3%.1 Reports and studies suggest that thrombolytic agents such as recombinant tissue plasminogen activator (r-tPA) are safe in these patients.2,3 Based on the available literature, the historical risk estimation for aneurysmal bleeding after receiving intravenous thrombolytics for acute ischemic stroke with cerebral aneurysm is approximately 5.7% (Figure 1).4 Most of the studies focused on the treatment methods and outcomes, but not on the presence of aneurysmal risk factors such as hypertension, smoking, or a family history of aneurysm or subarachnoid hemorrhage.1,5,6 In addition to chronic diseases, these factors can play a role in aneurysmal rupture and hemorrhage after using r-tPA. Our objective is to report the case of an acute ischemic stroke patient who safely received intravenous r-tPA and was later found to have 2 incidental cerebral aneurysms, demonstrating the safety of r-tPA among these patients. We also aim to review the literature to explore the safety of r-tPA and how clinicians can estimate the risk of an aneurysmal rupture hemorrhage.
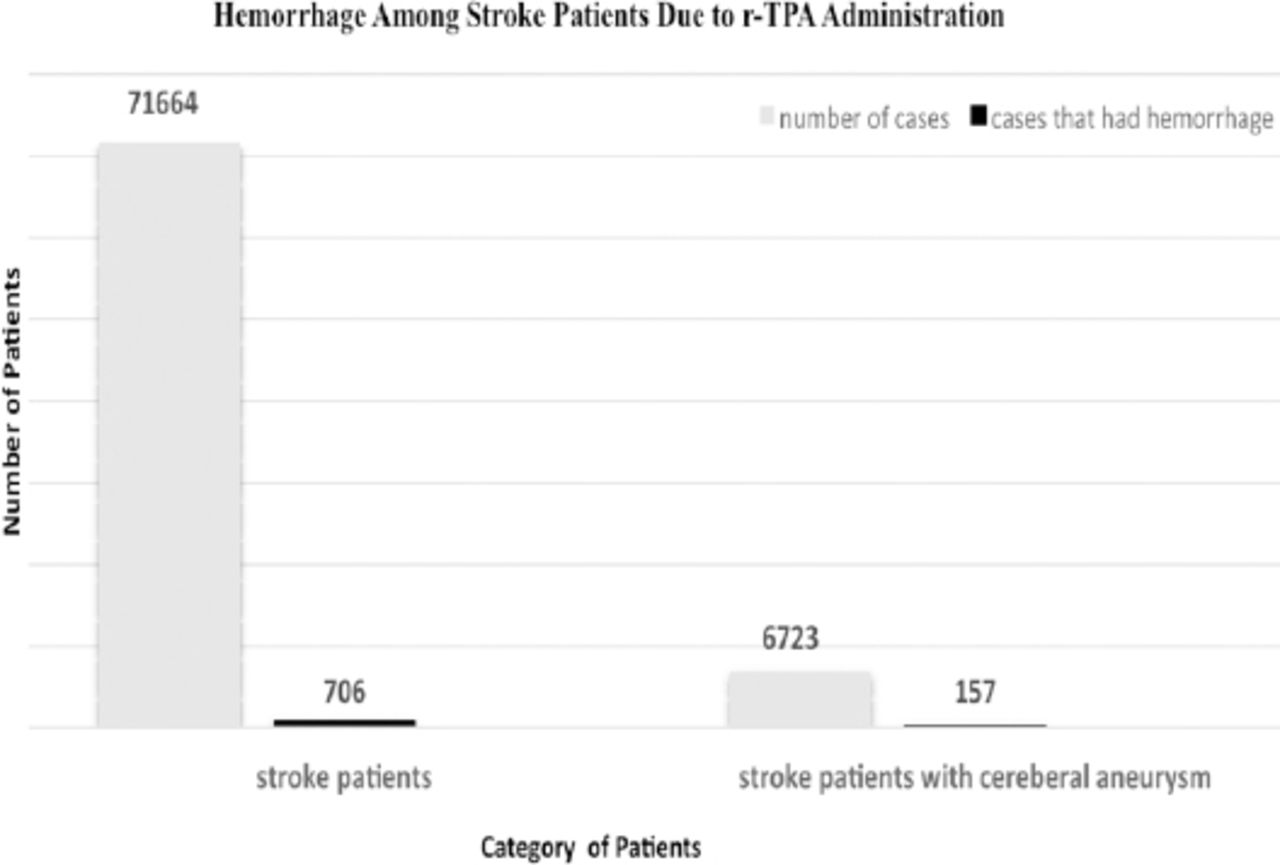
The total number of stroke patients who had hemorrhages after administration of r-tPA, including those who had cerebral aneurysms.
Case Report
Patient information
A 58-year old Eritrean African black man was known to be hypertensive and dyslipidemic and had undergone a coronary artery stenting 3 weeks prior to his presentation. He presented to the Emergency Department complaining of weakness and aphasia.
Clinical findings
The patient had significant sudden onset weakness for the past 2 hours on the right side of his body, more so in his face and arm than in his leg. He had expressive aphasia but was able to follow simple commands. He was rated an 11 on the National Institute of Health Stroke Scale.
Diagnostic assessment
An emergency computed tomography (CT) scan was performed which showed no evidence of hemorrhage or other acute changes.
Therapeutic intervention
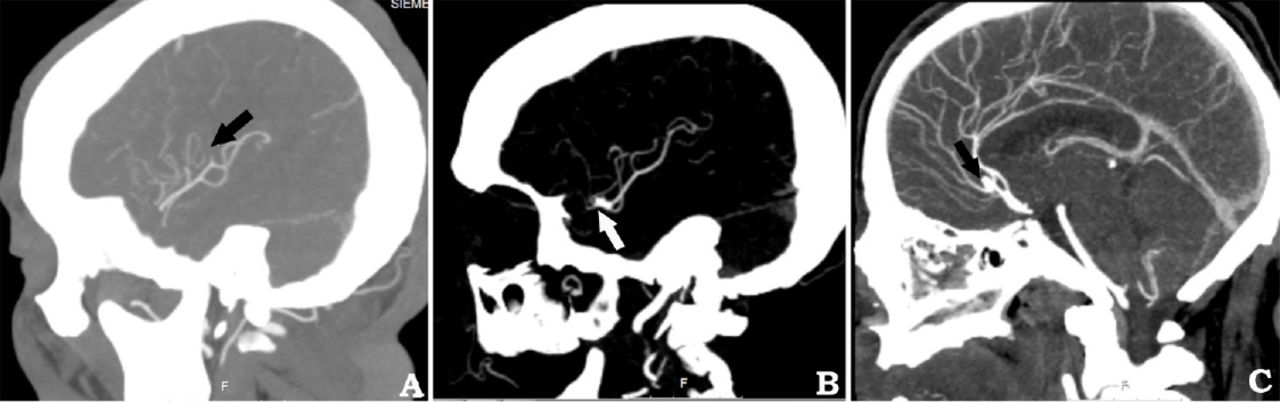
After discussing with the patient’s family and receiving consent, 65 mg of intravenous r-tPA was administered at the beginning, 3 hours after the time of onset. After starting the r-tPA, the patient was rushed for a CT angiogram that showed a distal branch occlusion of the left middle cerebral artery (Figure 2A). In addition, there were 2 cerebral aneurysms: one 5-mm pericallosal aneurysm (Figure 2B) and one 2-mm middle-cerebral artery bifurcation aneurysm (Figure 2C). Because these were believed to be incidentally discovered, r-tPA was continued and the patient was admitted to the intensive care unit.

CT angiography scans of patient’s brain performed after starting the r-tPA A) Computed tomography (CT) angiography of a distal branch occlusion of the middle cerebral artery; B) CT angiography of a 2-mm middle cerebral artery bifurcation aneurysm; C) CT angiography of a 5-mm pericallosal aneurysm.
Follow-up and outcomes
The neurological examination on the next day showed complete resolution of the initial deficits, with no complaints by the patient of headache or other neurological symptoms. A 24-h CT scan of the head showed no hemorrhagic transformation or subarachnoid hemorrhage. He was discharged home on Day 3 in a normal state with an elective plan for follow-up.
Discussion
Because it affects the outcome, time is extremely sensitive in the management of acute ischemic stroke patients. The most feared complication of administering r-tPA is intracranial hemorrhage, which is estimated to occur in 0.3%-6.4% of cases.5,7,8 In the majority of cases, the benefits of therapy outweigh the risks when given within 4.5 hours of onset or last-seen well time. However, there are circumstances in which r-tPA use poses a significant risk and is thus contraindicated. These include the presence of an intracranial hemorrhage or large subacute stroke and uncontrolled hypertension at the time of presentation that is not responding to intravenous blood pressure-lowering agents. However, there are perceived absolute contraindications that have not actually been proven with data.9 One of these is the presence of incidental unruptured brain aneurysms.
There is a good body of literature reporting on the safety of r-tPA in patients with incidental brain aneurysms. However, there are variations among the case reports (Table 1) and analytic reviews (Table 2) such as the thrombolytic agent, aneurysm size and site, and the existence of co-morbidities and risk factors of intracerebral hemorrhage that is related to thrombolysis. These risk factors include hypertension, smoking, alcohol consumption, a family history of aneurysm or subarachnoid hemorrhage, advanced age of the patient, thrombolytic dosage, hyperfibrinogenemia, increased prothrombin time, thrombocytopenia, hyperglycemia, and delayed treatment.1,5,6
Analysis of previous case reports.
Analysis of previous systemic studies.
Thrombolytic therapy may provoke aneurysm rupture by one of the following mechanisms: (1) increasing turbulence within the sac though hemodynamic changes or (2) increasing the flow within the aneurysm by dissolving a clot in the aneurysm dome.5 Yet, the use of r-tPA is an effective method for acute ischemic stroke treatment.5 Some of the r-tPA-related hemorrhages in patients with brain aneurysms were at the site of infarction but not due to aneurysmal rupture.4 A careful evaluation of the aneurysm’s size and site must be made to assess the risk of rupture. In addition, other medical conditions can be associated with an increased risk of rupture that are independent of the presenting stroke or r-tPA usage.1 The presence of co-morbidities plays a major role in aneurysmal rupture, first because they have an impact on the pathological vascular changes, and second, in the absence of stroke, the co-morbidities will be under consideration while evaluating the aneurysm for its risk of rupturing. Most of the reported cases with a ruptured aneurysm or hemorrhagic event had a co-existing chronic medical condition. Aneurysms can only be diagnosed by a CT angiogram, and the majority of stroke patients in Kingdom of Saudi Arabia do not receive them. Despite that, subarachnoid hemorrhage after r-tPA administration is very rare, which means that r-tPA is safe in these patients.
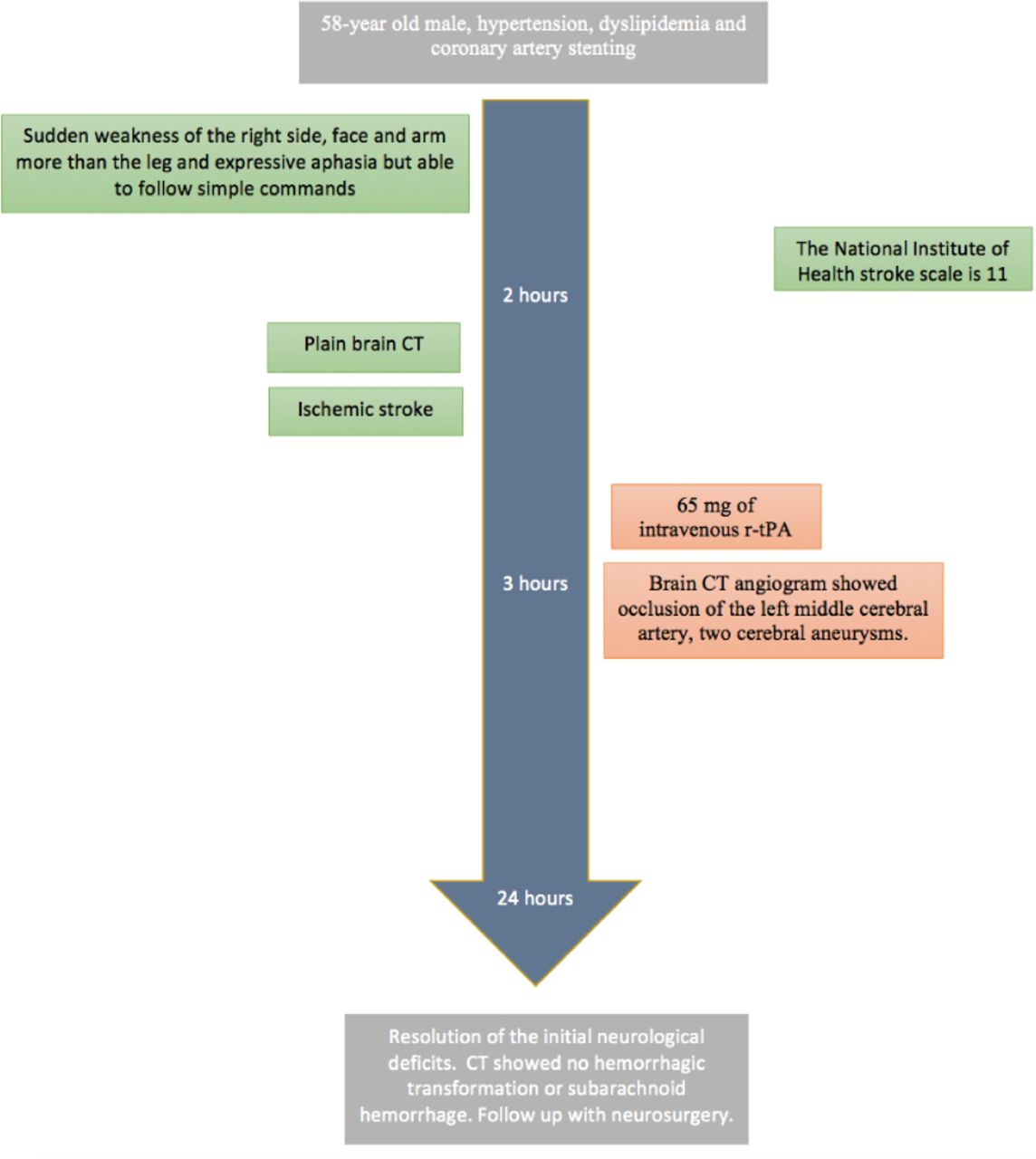
In conclusion, According to the available evidence, treating acute ischemic stroke patients with incidental unruptured aneurysms by r-tPA appears to be safe. A careful CT-scan assessment of stroke patients and an evaluation of the risk of aneurysmal rupture is important when CT angiography reveals brain aneurysms in the acute-stroke setting as in our case that is summarized in a timeline (Figure 3).

Case report timeline.
Footnotes
Disclosure. The authors declare no conflicting interests, support or funding from any drug company.
- Received January 29, 2018.
- Accepted June 20, 2018.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.