


Abstract
Schwannomas are benign encapsulated tumors of Schwan cells that grow slowly along the peripheral myelin nerve fibers. Sacral spinal schwannomas are very rare, and the incidence of sacral schwannoma ranges from 1-5% of all spinal schwannomas, and only around 50 cases are reported in the literature. There are 3 defined types of sacral schwannomas. These are retroperitoneal or presacral, intra osseous, and spinal schwannomas. Patients commonly present with complaints of pain and paresthesia due to the spinal schwannoma extending to extra spinal tissues. Direct x-ray, CT, MRI, and scintigraphy are used for preoperative diagnosis and treatment planning. Local recurrence and transformation to malignancy is very rare. For this reason, the frequently preferred treatments are subtotal removal of the mass or simple enucleation. In our article, we discuss the clinical features and the surgical treatment we performed without the need for stabilization in an incidentally determined giant invasive schwannoma case.
Primitive sacral and presacral tumors are very rare. Spinal schwannomas constitute approximately 25% of vertebral tumors. They most commonly tend to settle in the thoracic region. They are very rarely seen in the sacral region and constitute 1-5% of all spinal schwannomas, and only around 50 cases are reported in the literature.1-3 Schwannomas are mostly benign lesions. Malignant ones are either malignant from the beginning or become malignant due to degeneration of benign schwannomas, such as is the case in neurofibromatosis type II patients. There are 3 defined types of sacral schwannomas; retroperitoneal or presacral, intra osseous, or spinal schwannomas. According to the definition by Sridhar et al,2 giant invasive spinal schwannomas are masses that invade more than 2 vertebral levels, invade vertebral bodies, and by extending posteriorly, reach the myofascial regions. For this reason, the clinical and surgical results of giant invasive type spinal schwannomas (GISS) differ slightly from typical schwannomas. The clinical diagnoses of these tumors are made by direct x-ray, CT, and MRI. The ideal treatment of GISS would be to totally remove the tumor by decompression and surgery without creating any neural complications or spinal instability, which would relieve the pressure on neural organs created by the mass and regress symptoms.3-5 Our objective in presenting this particular case is to highlight an interesting and rare presentation for incidentally diagnosed giant invasive schwannoma of the sacrum.
Case Report
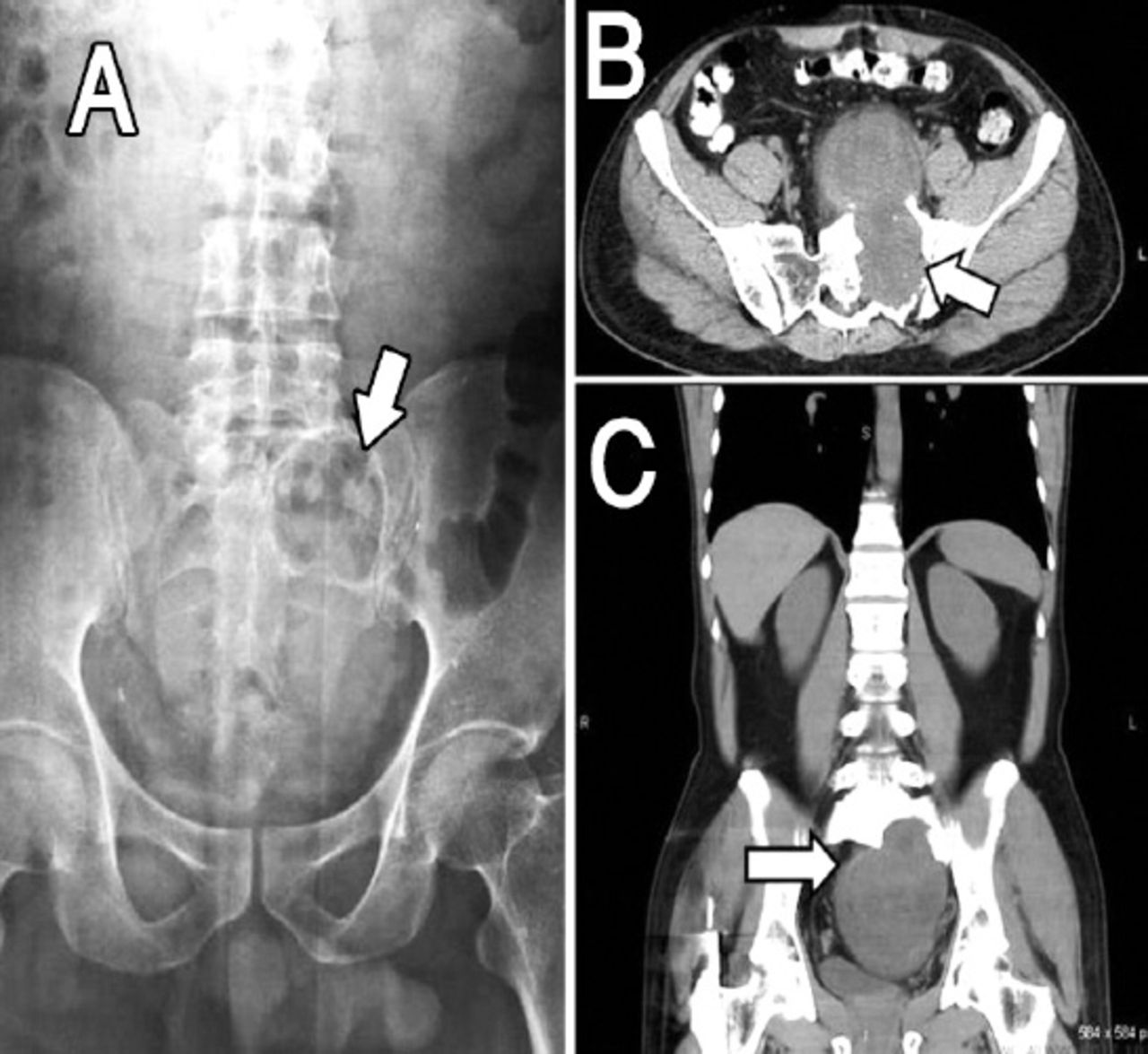
A 42-year-old male patient presented to the general surgery polyclinic with the complaint of left upper quadrant pain that had been present for 3 months. On the incidental detection of a mass in his abdominal ultrasonography, and as he had been pre diagnosed with cholelithiasis, abdominal CT, and pelvic MRI were requested. A hyper dense sclerotic lobular contoured mass lesion that was destructing the left half of the sacrum was detected on x-ray and CT (Figure 1). On MRI, there was a heterogeneous, hypo-intense mass lesion found at the level of the S1-2 vertebra in T2 sequence of bone marrow in the heterogeneous hyper-intense T1 weighted images that originated from the left lateral side, and that had grown into the extraperitoneal area of the abdomen. The mass was visualized up to the left lateral aspect of the L5-S1 vertebra, and its widest axial diameter was 138 × 91 mm. There was post contrast intensive opaque agent uptake and no calcification or necrosis was observed in the lesion. The lesion progressed inside the left lateral sacral spinal canal and was narrowing the canal diameter (Figure 2). The complaints of abdominal pain, paresthesia, and motor weakness, which are very common in these patients, were not present in our patient. He had no history of trauma. There were no defecation and urinary system complaints. There was sensorial loss in the S1-3 regions. Bilateral deep tendon reflexes at both knees and ankles were normal. There were no signs of fasciculation, muscle atrophy, and upper extremity motor neuron dysfunction on his physical examination. There were no dermatologic signs of neurofibromatosis. The mass was palpable on rectal examination since the tumor was creating a pressure effect and was pushing the rectum. Since the Tru-cut biopsy result was spindle cell mesenchymal neoplasm (nerve sheath origin), he was scheduled for surgery.
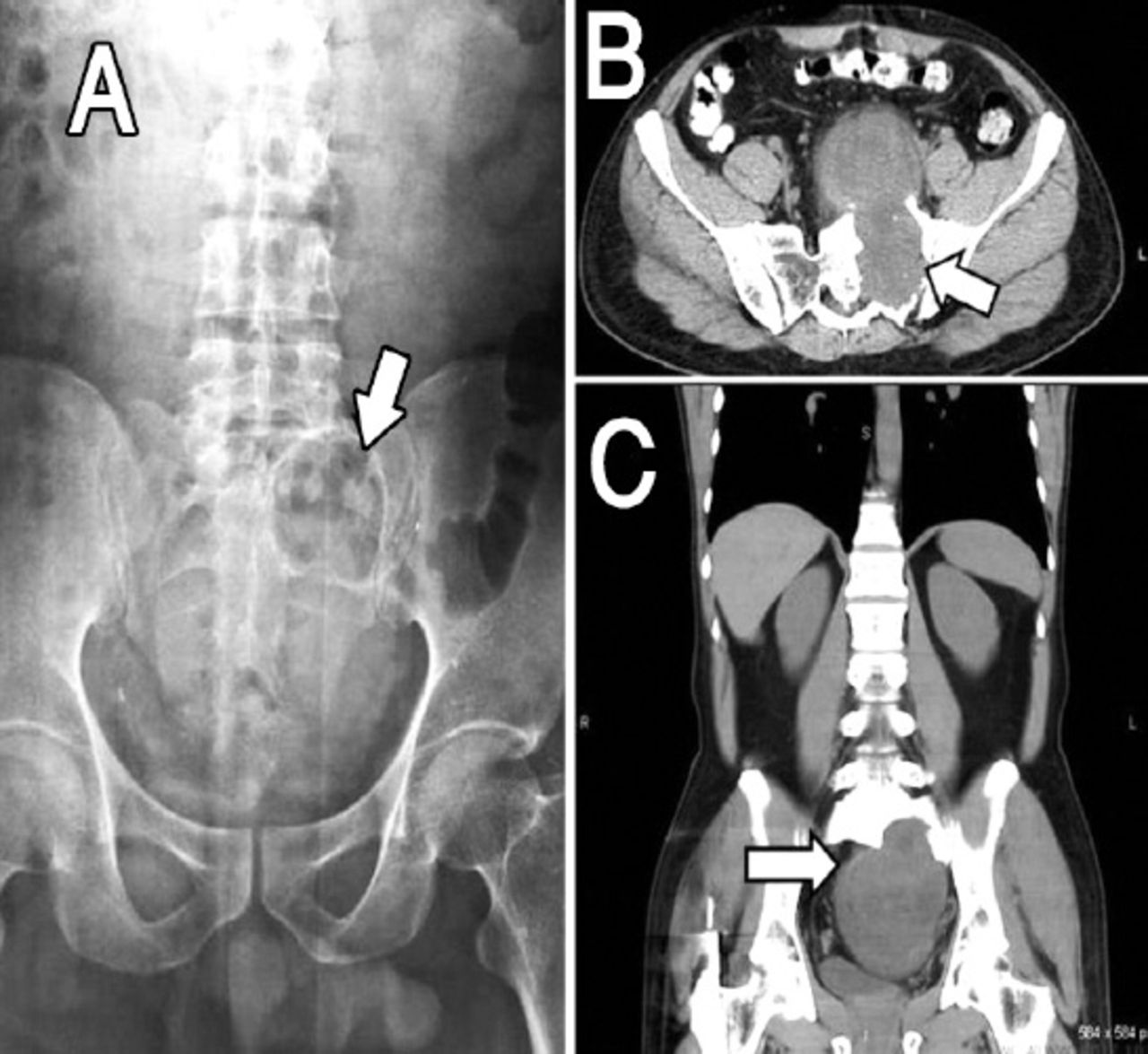
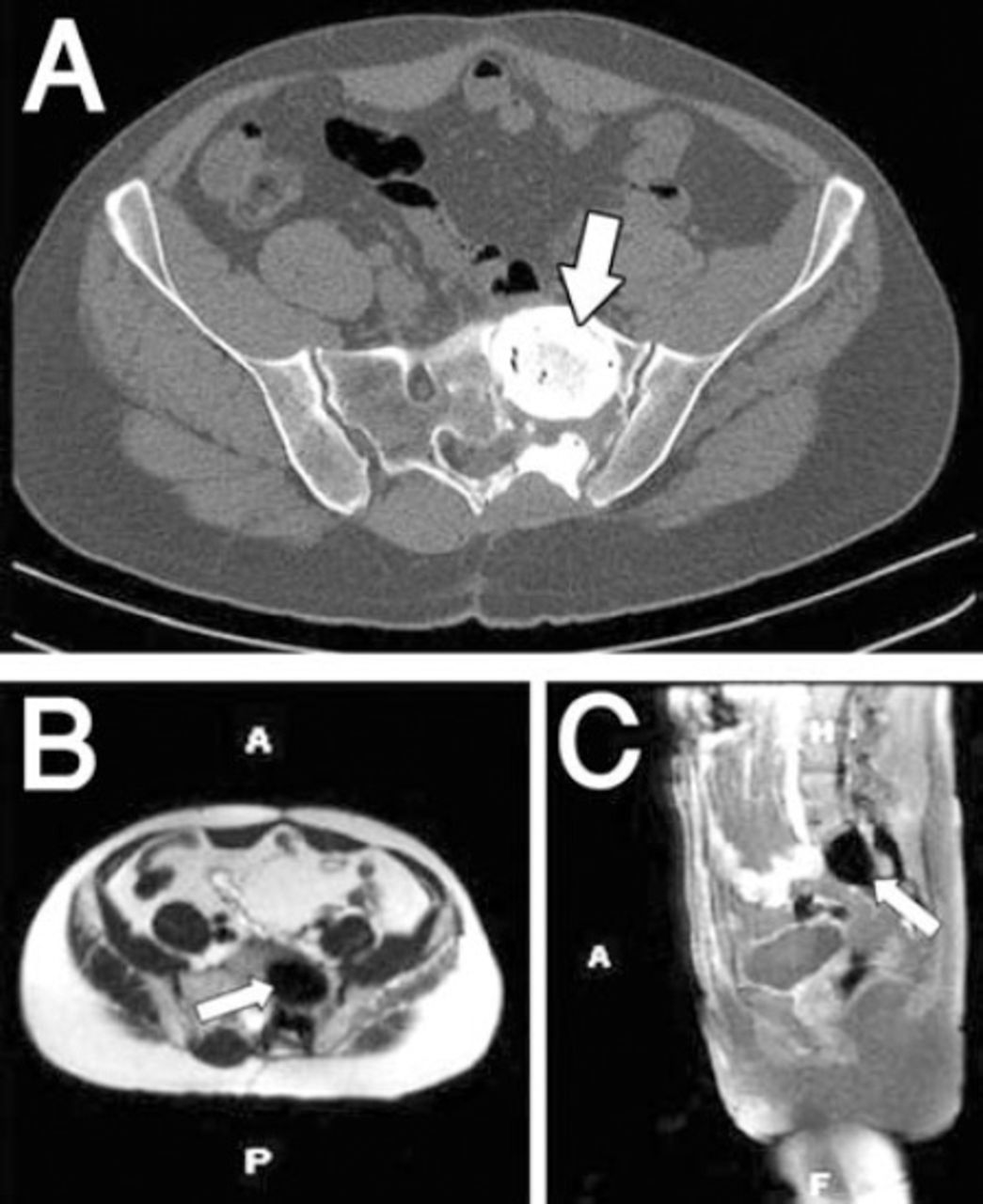
Preoperative images showing: A) Patient x-ray showing a sclerotic margined, smooth contoured cavity lesion invading the left half of the sacrum. B) Axial CT showing lobulated contoured hypo dense heterogeneous mass that has destructed the neural foramens, filling the pelvis and displacing the bladder anteriorly. C) Coronal CT cross section showing a hyperdense sclerotic lobulated contoured mass, from the left half of the sacrum and filling the pelvis.
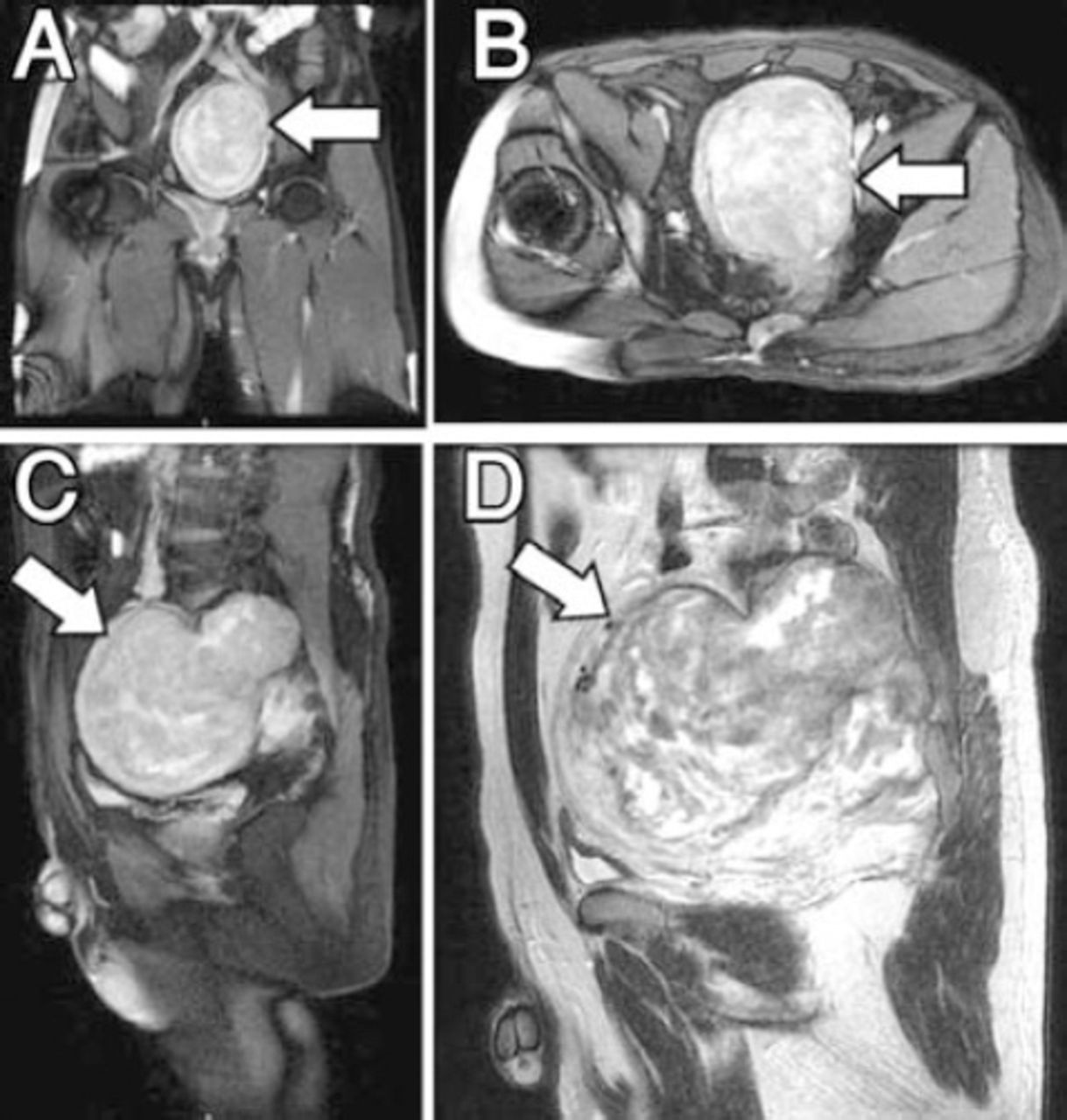
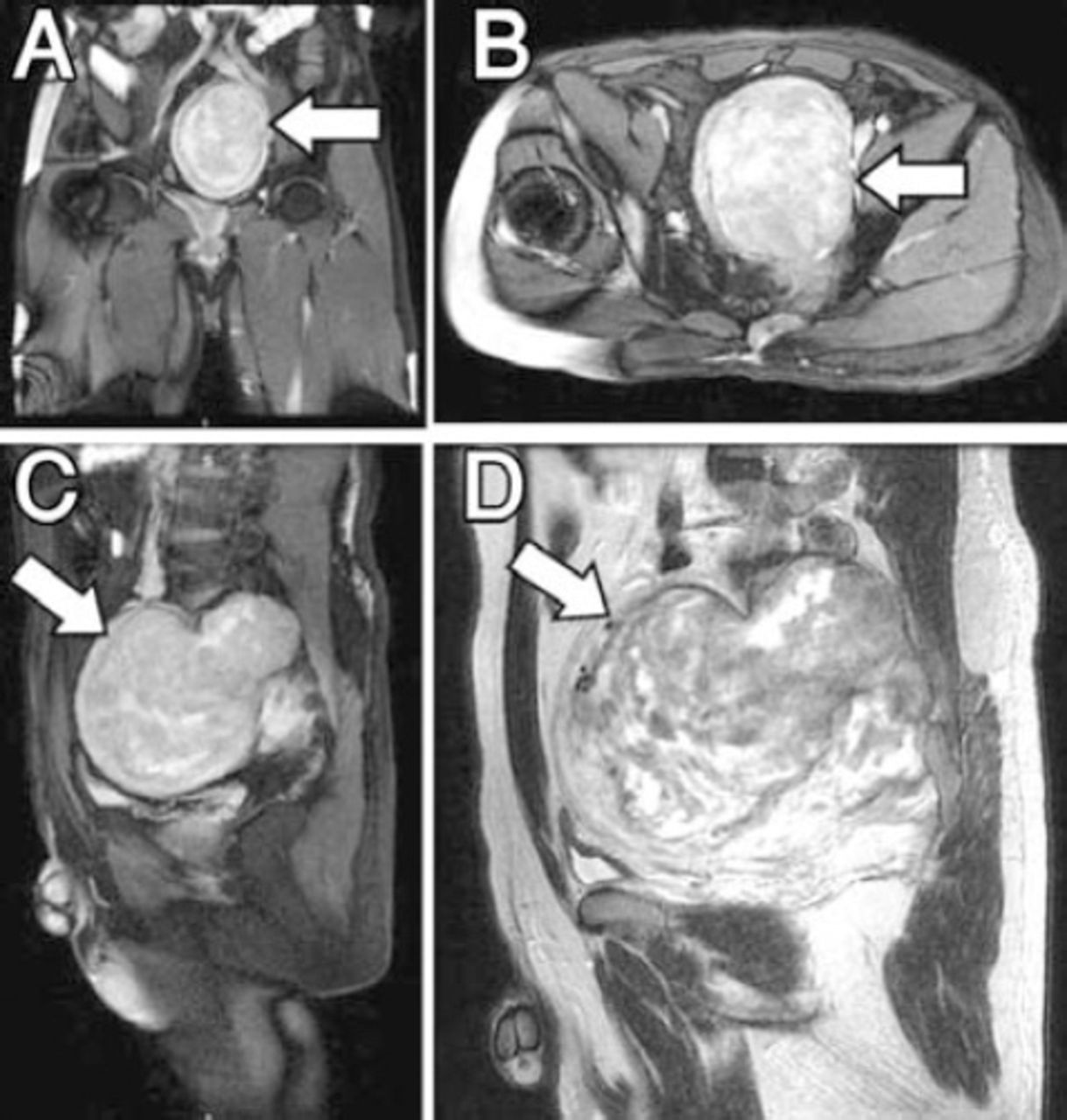
Preoperative MRI sections showing: A) T2 weighted coronal MRI showing hyperintense lobulated mass filling the pelvis. B) T2 weighted axial MRI showing hyperintense mass with its largest diameter 138 × 91 mm. C) T2 weighted sagittal MRI showing a dense heterogeneous opaque mass with agent uptake, sagittal 146 × 114 mm sized mass invading the left sacral spinal canal. D) T1 weighted sagittal MRI showing opaque involvement belonging to calcified and necrotic areas inside the lesion.
Surgery was performed with an anterior and posterior combined approach. During the operation, first we entered the abdomen with an anterior longitudinal midline incision. With the aid of a general surgeon, the mass was reached by advancing with a retroperitoneal dissection. The rectum was separated from the tumor. During the operation, while the tumor was separated from the surrounding tissues with dissection, the left sacral nerve roots were preserved as much as possible with the assistance of a neuro-monitor system. The left internal iliac artery and vein were tied. The mass was partially removed, with preserving the capsule, up to the anterior area of bone involvement. In the same session, he was turned to the prone position, and with a posterior approach, by passing through the posterior sacrum cortex; the intraosseous part was removed piece by piece. The walls were cleaned with a curette. Since the sacroiliac joint was stable and the tumor was benign, the intraosseous space was filled with 80 grams (2 boxes) of bone cement. The duration of the operation was approximately 210 minutes. Bleeding was approximately 850 ml. He had no signs of postoperative wound site infection and was mobilized on the fourth day. Histopathological examination revealed schwannoma. On microscopic examination, there was a spindle cell neoplasm that was morphologically consistent with classical schwannoma. Focal nuclear palisading was observed. The nuclei were oval blunt-ended or elongated, and focally epithelioid morphology was observed. There were hyalinized thick walled blood vessels (Figure 3). He had no prominent neurologic deficits, and had no complaints of stool and urine incontinence. Although he had no problems with penile erection, he had developed insensitivity on the penile skin surface that recovered 4 months postoperatively. Following the surgery, weakness of the left thigh and leg muscles, loss of strength, numbness, and motor deficit of the foot plantar flexors developed. These complaints were observed to continue during the postoperative first year follow up examination. There was no recurrence detected in the MRI performed one year after surgery (Figure 4).

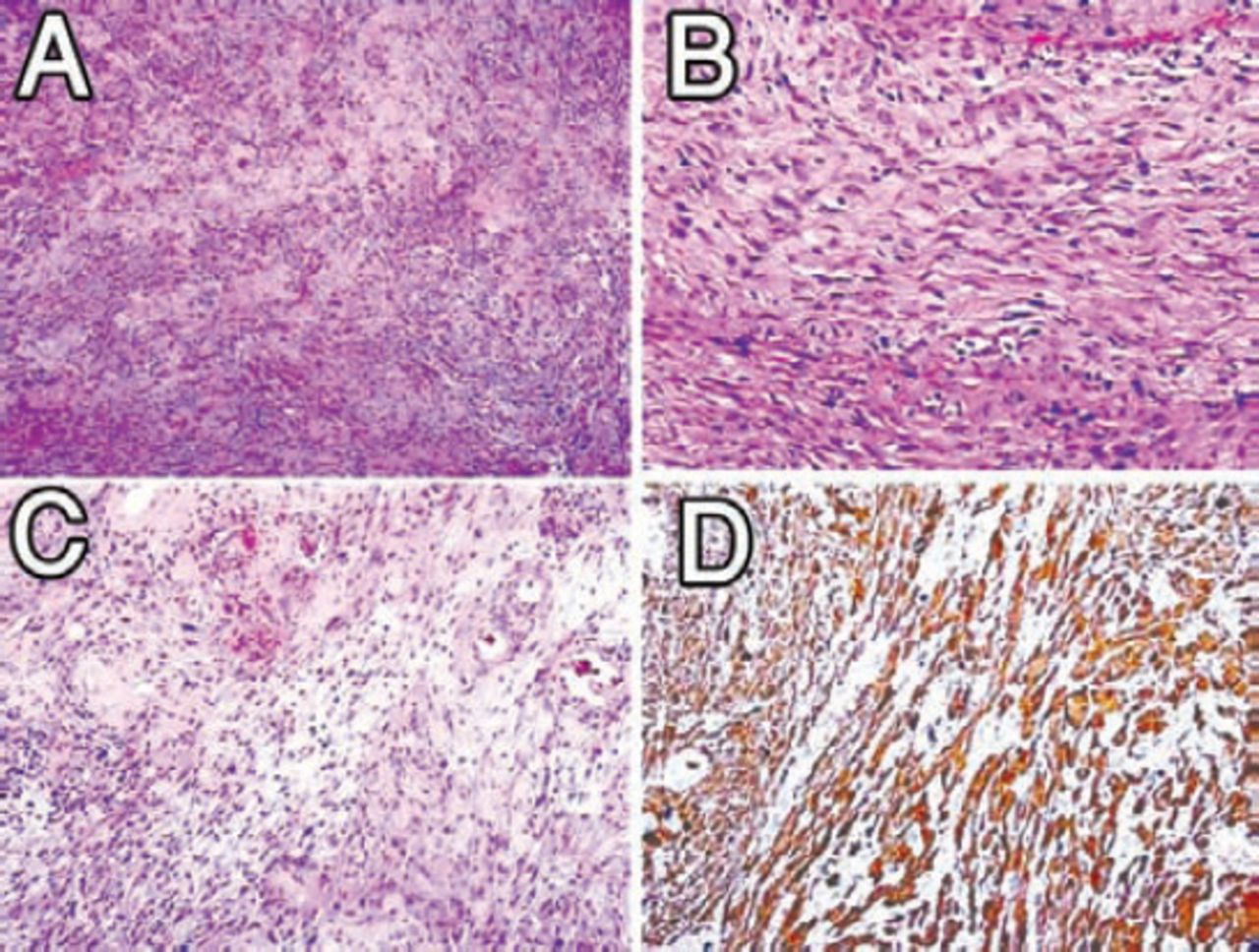
Histopathological examination of specimens: A) Irregular fascicles of spindle cells, nuclear palisading, Hematoxylin & Eosin (HE) × 100. B) Cellular detail. Oval blunt-ended or elongated nuclei, HE × 400. C) Hyalinized blood vessels and relatively myxoid stroma, HE × 200. D) Diffuse S100 protein positivity, HE × 400.
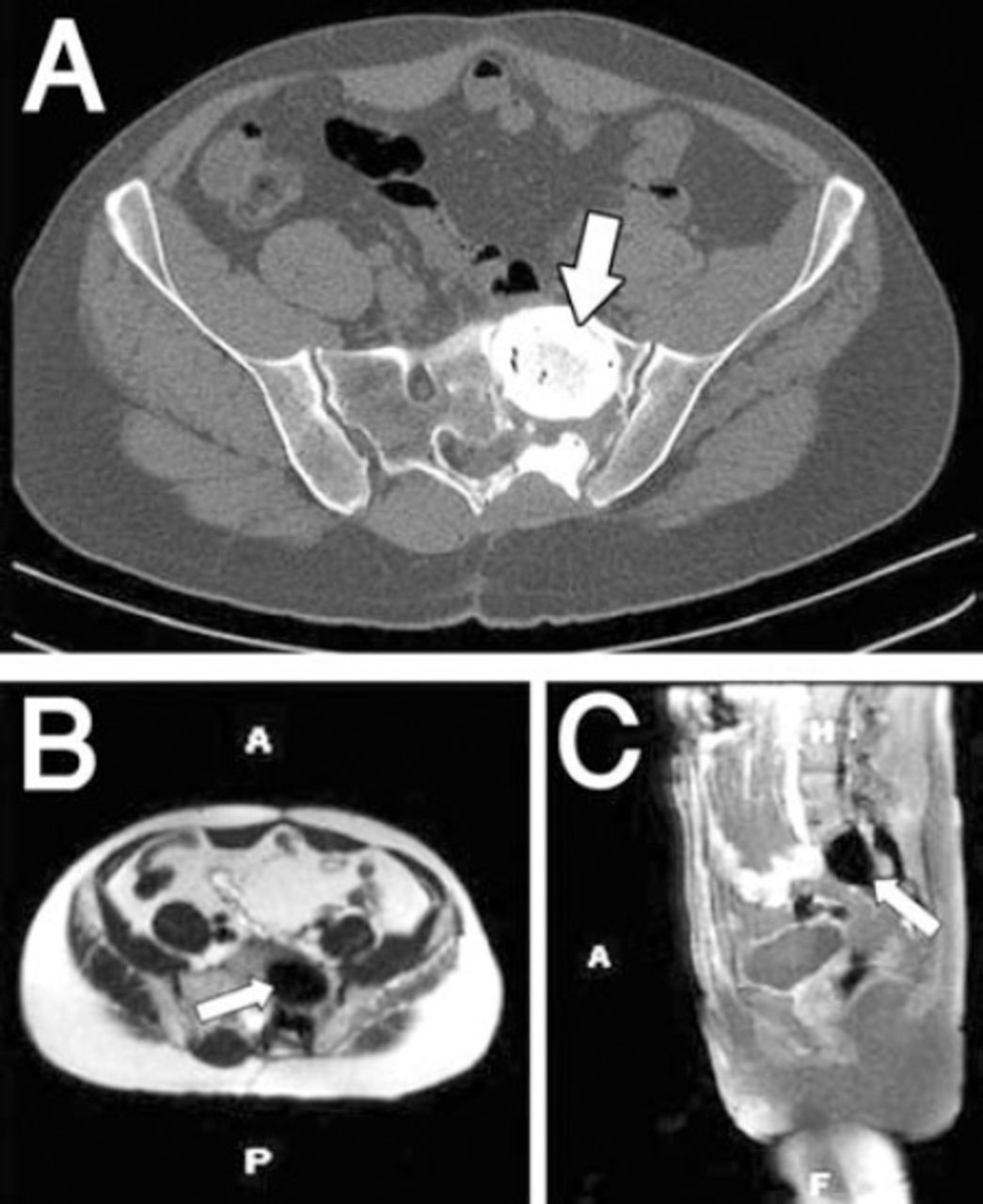
There was no recurrence detected on MRI in the postoperative first year. A) Axial CT, B) Axial MRI, C) Sagittal MRI. A - anterior, P - posterior, H - head, F - foot
Discussion
Sacral region tumors are diverse, including chordomas, chondrosarcomas, giant cell tumors, plasmacytomas, lymphomas, aneurysmal bone cyst, inflammatory, and congenital lesions.1,3,4 Schwannomas are benign encapsulated tumors of Schwann cells that grow slowly through the peripheral myelin nerve fibers. Schwannomas are seen at very small percentages in the sacrum. Most of the spinal schwannomas are intradural. However, 30% of them extend out from the dural roots and also include extradural components.6,7 Usually, the patients present with pain or paresthesia, with complaints caused by the extension of spinal schwannomas into extra spinal tissues. These tumors are large, heterogeneous in character, slow growing, and can display a combined abdominal and posterior extension. The term giant invasive schwannoma has not been completely clarified. Sridhar et al2 defined GISS as a tumor that invades 2 or more vertebral levels, extends more than 2.5 cm extraspinally, causes erosion of the spinal body, and tends to displace to the posterior or lateral myofascial plane.2,8 They are usually asymptomatic until they reach a large size. Lumbar radicular pain is the most common symptom. Frequently, there is sacral paresthesia and dysesthesia. There may be urinary retention or incontinence complaints. There may be constipation, rectal fullness, motor weakness, and decrease of the deep tendon reflexes. In our case, there were no prominent complaints except for mild pain in the left upper abdominal quadrant.1,4,6 Direct x-ray, CT, MRI, and scintigraphy are used for preoperative diagnosis and treatment planning. In pelvic CT, while it defines the densities of present fluid or fat, it also visualizes the relationship of anatomic structures (sacrum-coccyx-rectum) and calcification content (chordoma). Benign schwannomas are isointense with muscle on MRI T1 weighed sequences, and give a hyperintense image in T2 weighed sequences. Cyst formation calcifications can also be seen. Whereas in malignant peripheral nerve sheath tumors, there is heterogeneous contrast uptake accompanied with a pseudo capsule. Pelvic MRI is important because it demonstrates tumor type with size, the actual localization, and its relationship with other vital intrapelvic organs. The MRI is also important for the demonstration of tumor capsule with high sensitivity.1,6,8 The tumor was classified by its localization according to the modified Sridhar classification (Table 1).5 Klimo et al6 divided sacral nerve sheath tumors into 3 groups according to their localizations. Type 1 tumors are limited to the sacrum and can be removed by the posterior approach. Type 2 tumors extend to the anterior and posterior bone limits of the sacrum and a combined approach (anterior and posterior) is required for its removal. In type 3, the tumors are localized to the presacral region and the anterior approach is sufficient for its removal.6,7 Our case was compatible with type 5, according to the modified Sridhar classification, and type 2 according to the Klimo classification.
Modified Sridhar classification of benign nerve sheath tumors.5
Even if there is only a suspicion of schwannoma with imaging methods, biopsy should be performed to distinguish between malignant and benign lesions. Many authors disagree on the need for biopsy since it can cause bleeding and infection. However, a diagnosis such as lymphoma would completely change the whole treatment modality. Although fine needle biopsy is the golden standard, caution should be taken according to the tumors location. In pre sacral lesions, biopsy can be performed from the sciatic notch.1,3,7
During surgical treatments, spinal schwannomas should be removed without damaging the surrounding major neurovascular organs. However, it is almost always difficult, particularly in giant invasive spinal schwannomas because of the invasive structure of the tumor, compressive effects, and its invasion to surrounding neurovascular organs. In the literature, although total resection is advocated for surgical treatment, because of the varying size of the mass, this is not always successful. Other than surgical treatment; embolization, chemotherapy, and hyperthermia with chemotherapy, or cryotherapy in elective cases are the other possible adjuvant treatments.2,5,8 The treatment plan of surgical approaches can vary depending on the intrasacral and retroperitoneal extension of the mass. The posterior approach is used in cases where the tumor extends into the spinal canal or sacrum, and its presacral component is small. An anterior transabdominal or retroperitoneal approach is usually required to protect the vascular plexus and intrapelvic organs and to liberate the tumor. The postoperative reconstruction planning of bone structures depends on the destruction of the sacral bone and invasion of the sacroiliac joint. A CT is highly useful for evaluating this situation. Local recurrence and malign transformation is very rare. For this reason, piece by piece subtotal removal, or simple enucleation of the mass is a frequently preferred treatment choice. Also, there are authors that defend complete resection with an aggressive approach because spinal schwannomas can grow again, and if removed inadequately, the reoperations in these situations have higher complication risks. Although there has been no complete consensus developed regarding the benefits of total resection, some authors advocate the fact that although there is the risk of developing neurologic deficits following total resection, it can prevent recurrence.4-6 On the other hand, Pongsthorn et al8 reported that subtotal removal of the tumor piece by piece gives good results and neurological complications are thereby avoided.1,7,8 In our case, since the schwannoma was a benign and slow growing tumor with a late and low risk of recurrence; due to the existence of S1-2 invasion and prominent destruction of bone, in order not to cause severe neurologic complications that can result from total resection, we removed the tumor piece by piece with an anterior and posterior combined approach. Thinking that the sacroiliac joint was stable, we did not use instrumentation. By filling the formed space with bone cement at the same time, we aimed to benefit from the hyperthermia effect of the cement. Following the surgery, weakness of the left thigh and leg muscles, loss of strength, numbness, motor deficit of the foot plantar flexors developed. There was no severe neurologic deficit in our patient, and no recurrence was detected in the postoperative first year.
In conclusion, giant sacral schwannomas are slow growing benign tumors that frequently do not cause any complaints, until they reach a certain mass. An MRI is very helpful in diagnosis and in demonstrating the relationship of the tumor with visceral organs. A CT should be used to demonstrate the osseous damage and postoperative planning. The subtotal removal of tumors, piece by piece, with anterior, posterior or combined approaches results in good outcomes, and thus unnecessary neurologic complications can be avoided.
Acknowledgments
We would like to thank Dr. Bilgin K. Aribas for the radiological images, and Dr. Fusun Ardic Yukruk for pathological examinations.
Footnotes
Disclosure
No benefits in any form have been or will be received from a commercial party related directly or indirectly to the subject of this manuscript.
- Received January 16, 2014.
- Accepted April 29, 2014.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.