


Abstract
Penetrating craniocerebral injuries from nail gun use are rare. We describe a case of 10 self-inflicted nail gun injuries with intracranial penetrations. We also review the literature and discuss management strategies of such craniocerebral trauma. A 33-year-old male with a long-standing history of severe depression took a nail gun and sustained 10 penetrating intracranial injuries. Initial neuroimaging revealed 10 penetrating nails, all sparing the major cerebral vasculature. Immediate surgical removal was undertaken in the surgical suite using a combination of craniotomies, craniectomies, and blind removal. Intracranial injuries from self-inflicted nail gun misuse is becoming increasingly more frequent. Initial appropriate clinical decision-making are critical in preventing further cortical or vascular damage.
Intracranial nail gun injuries, although unusual, are a well-described form of penetrating cranial trauma. This mechanism of injury presents unique problems for the patient and the treating physician. The increasing availability and consequent use of compressed air driven nail guns has increased the likelihood of craniocerebral penetrating trauma associated with these devices. In the United States, the Centers for Disease Control report, on average, around 37,000 patients with injuries related to nail gun use treated annually in emergency departments between 2001 and 2005, with 40% involving home consumers.1 Overall, self-inflicted nail gun injuries are less common than accidental discharges, which occur mostly on the construction site and involve injury to an extremity. Treating these penetrating brain injuries presents a number of clinical challenges to the surgeon. Nonetheless, a sound rational management strategy should permit most of these patients to be discharged with no additional injury. In this case report, we report a unique case of self-inflicted craniocerebral penetrating injuries, due to a pneumatic nail gun, involving 10 nails. Based on a literature review, this is largest number of penetrating foreign objects removed from the cranium and cerebral parenchyma in a patient that survived and made a full complete recovery. Our objective in presenting this particular case is to demonstrate that although nail gun injuries are often impressive on radiographic imaging, they often produce a very limited local injury with very little neurologic devastation.
Case Report
History and physical examination
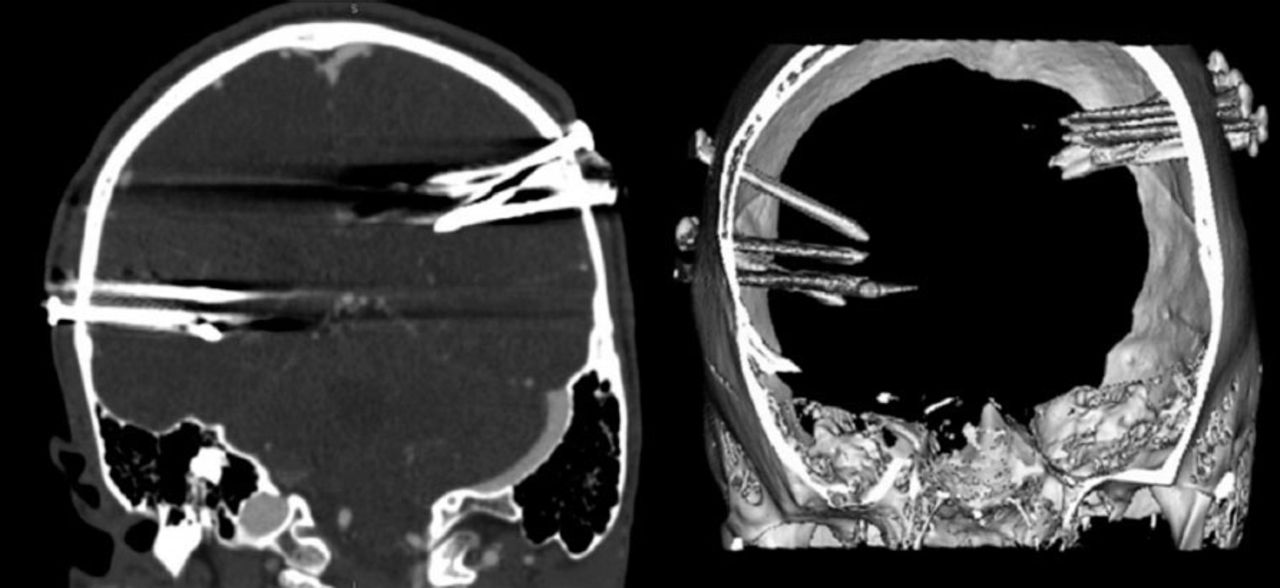
A 33-year-old right-handed male took a pneumatic nail gun and shot himself 10 times in the head: 5 times on the right, and 5 on the left. He reportedly suffered no obvious immediate sequelae: he was found well and watching television by his parents who compelled him to attend an emergency room when he informed them what he had done. He was subsequently transferred to our tertiary care hospital for definitive neurosurgical management. On the way, he had a focal seizure. On arrival, he was immediately assessed by the neurosurgical service where his initial neurological examination revealed that he was oriented in all 3 spheres, with a Glasgow Coma Scale score of 15. His pupils were equal and reactive to light bilaterally, and he had full visual fields. Examination of his extraocular movements revealed a left abducens palsy. In addition, a left facial droop, left tongue deviation, right uvula deviation, mild dysarthria, subtle left sided motor weakness, and questionable decreased sensation over the left side were also noted. Due to the history of a focal seizure, he was loaded with 1g of phenytoin IV, and treated subsequently with a 7-day course of the anti-epileptic medication. His medical history included psoriasis, depression, and smoking. There was no history of prior suicide attempts or psychiatric admissions. The initial skull x-ray and non-contrast enhanced CT imaging revealed 10 metallic foreign bodies with a nail appearance projected over the temporal and occipitoparietal area bilaterally (Figures 1 & 2). This was associated with a small distal left parietal subarachnoid hemorrhage of traumatic nature. A CT angiogram did not reveal any convincing evidence of cerebral vasculature compromise.

Plain posterior-anterior skull x-ray demonstrating the foreign bodies.
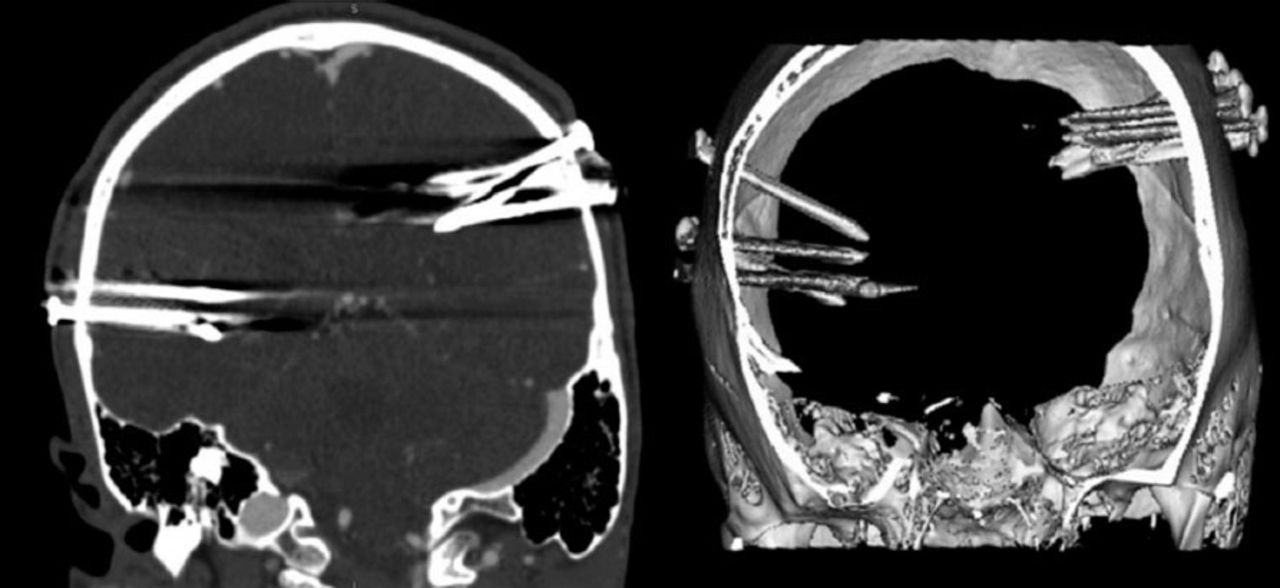
Plain CT demonstrating the intracranial nails with 3D reconstruction.
Operation
A decision was made by the neurosurgical service to bring him to the surgical suite on an emergent basis where he underwent bilateral small craniectomies and craniotomies for removal of each of the foreign bodies. Each nail measured 10 cm in length (Figures 3 & 4). There were no perioperative complications. Post-operative CT imaging revealed only small multiple foci of intraparenchymal hemorrhage and associated subarachnoid hemorrhage. In addition, CT angiogram carried out on post-operative day 2 did not reveal any post-traumatic pseudoaneurysms or vasospasm. He was subsequently transferred to the inpatient psychiatry service in stable medical condition.

Intraoperative image demonstrating the penetrating foreign bodies.

Intraoperative image of foreign bodies.
Post-operative course
He was seen in the neurosurgery clinic for follow-up after one year. Physical examination revealed full extraocular movements, and resolution of all neurological deficits. There was no history suggestive of any seizures. A repeat non-contrast CT scan demonstrated complete resolution of all of the intracranial hemorrhages.
Discussion
With the growing use of pneumatic nail guns both in the construction industry and by home consumers, penetrating craniofacial injuries caused by these devices are on the rise. Most of these injuries are primarily work related accident,2-4 but they are also well-reported as intentionally self-inflicted.5 Preoperative evaluation should always include thin cut CT scans allowing for multiplanar reconstruction. In addition, assessment of the cerebral vasculature is prudent especially if the nail appears to traverse a major vessel although the incidence of vascular injury secondary to nail gun injury is low. Trauma to the cerebrovascular system has been associated with a wide variety of pathologic consequences including: arterial dissection, pseudoaneurysm, arteriovenous fistula, arterial or venous rupture or thrombosis,6 vessel perforations, carotid-cavernous fistula, and even fatal epistaxis.2
While catheter angiography has been the primary radiographic modality for diagnosing the extent of cerebrovascular trauma,7 CT angiography is an attractive screening imaging modality owing to the ease and rapidity of obtaining these images in the trauma setting. However, its sensitivity due to scatter artifact from the metallic foreign bodies is unclear.8 Nonetheless plain CT scan as well as CT angiograms are well-reported initial imaging modalities before surgical removal.7,9 Most of these injuries usually have relatively favorable neurological outcomes as long as the major cerebral vasculature and brainstem are not disrupted by the path of the penetrating nail.10
The primary and most commonly described vascular injury is the formation of a traumatic intracranial pseudoaneurysm, which necessitates both preoperative and follow-up cerebral angiography.8 Traumatic intracranial aneurysms are rare and they tend to manifest clinically within 3 weeks after the time of injury, associated with a 50% mortality rate.11 Because of the delayed visualization of traumatic pseudoaneurysms and the high risk of their formation in the setting of a nail gun injury, routine angiography should be performed in all patients between one to 2 weeks post injury.11
Infectious complications of penetrating head trauma are high, and include local wound infection, the formation of cerebral abscess, ventriculitis, and meningitis. However, the use of broad spectrum antibiotic prophylaxis is only recommended in penetrating neurotrauma although without established guidelines.12 In our patient, after discussion with our infectious disease colleagues, the patient received broad spectrum antibiotics for 5 days. Surgical treatment should be performed within 12 hours of the injury to decrease the risk of infectious complications.13 However, the technique to use is still debatable. No statistically significant advantage of one technique over the other has been described in reports of morbidity and mortality rates associated between a craniotomy or craniectomy.14 Whichever technique used, the mainstay of these injuries is the treatment goal of removal of the foreign object whether by removal under local anesthetics with the patient awake or emergent craniotomy under general anesthesia. Many single nail gun injuries were removed under local anesthetics with the patient awake.8 Blind removal is usually uneventful, however there have been complications arising such as subdural hematomas and even intraparenchymal hemorrhage. This has lead to the suggestion that all penetrating foreign bodies must be removed under direct vision.15 While most would proceed with a standard craniotomy around the foreign object, Spennato and colleagues16 describe the use of a double concentric craniotomy allowing for removal under direct visualization, without transmitting any undue forces to the underlying structures. This technique also facilitates hemostasis. In those situations when blind removal without formal craniotomy is judged appropriate, the availability of locking pliers (of the “Vise Grip ®” style) can be extremely helpful as their strong grip even with purchase limited to the edges of the nail head can permit extraction despite the usual firm implantation in the bone. The use of general anesthetic during removal is recommended for patients with more than 2 nails, high risks areas, or those in whom vascular injury is evident on preoperative imaging. Should there be evidence of injuries involving vascular structures, preoperative therapeutic embolisation should be considered. This allows angiographic visualization with endovascular control of the proximal injured vessel if needed, and immediate follow-up angiography post-removal. In addition, this is a feasible sole treatment technique where surgical management promises to be technically difficult or poorly tolerated by the patient, or when poor neurological condition does not warrant craniotomy.
Many patients presenting with intracranial injuries from nail gun misuse have an associated psychiatric disturbance, usually schizophrenia or major depressive disorder.17 As such, not only is it important to involve other surgical specialties for combined intracranial and extracranial injury, successful treatment requires the additional collaborative expertise of colleagues from psychiatry.
In conclusion, while most intracranial penetration from the use of a nail gun is single entry, here we present a case with 10 penetrating nail gun injuries. A careful clinical and radiologic examination is needed followed by extraction of the foreign body. Appropriate imaging includes CT scans with or without angiography and/or therapeutic embolisation. Most patients survive with good neurological outcome despite the dramatic appearance of the radiographic images.
Footnotes
Disclosure
This study was funded by the College of Medicine Research Center, Deanship of Scientific Research, King Saud University, Riyadh, Saudi Arabia.
- Received February 2, 2015.
- Accepted March 30, 2015.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.