


Abstract
Colloid cysts are cystic lesions that are usually located in the anterior portion of the third ventricle near the foramen of Monro. Rarely, hemorrhagic cysts can lead to acute obstructive hydrocephalus or sudden death. We herein report 2 cases and a review literature. We examine a 47-year old male who presented with progressive headache and a 55-year old male who presented with progressive memory disturbance and unsteady gait. Both cases demonstrated typical imaging features of hemorrhagic colloid cyst, and were histopathologically confirmed. Total excision was achieved in both cases with good outcomes. Hemorrhagic colloid cysts are rare; however, bleeding tendencies should be carefully considered in patients with these cysts. The degree of rapidity with which clinical deterioration occurs may play a major role in the preferred treatment approach and subsequent outcomes.
Colloid cysts are benign, thin-walled, cystic lesions that arise from the brain’s endodermal embryonic remnants, and they are usually located in the anterior portion of the third ventricle near the foramen of Monro; these cysts contain colloid material.1 The clinical presentation of these cysts ranges from incidental findings on brain images to sudden death. The clinical presentation of these cysts is largely dependent on the mass’ effect on the foramen of Monro.1 Rarely, hemorrhagic cysts can lead to acute obstructive hydrocephalus or sudden death.2,5 We herein report 2 cases of hemorrhagic colloid cysts.
Case Report
Case 1. Patient’s information
A 47-year old male presented with progressive morning headaches for a total of 10 days, which was associated with nausea and vomiting. He had no history of trauma or loss of consciousness.
Clinical findings
On examination, he had an intact level of consciousness. Funduscopic examination revealed bilateral papilledema. The patient’s cranial nerves, as well as his motor and sensory examinations, were normal without any signs of neurological deficits.
Diagnostic assessment
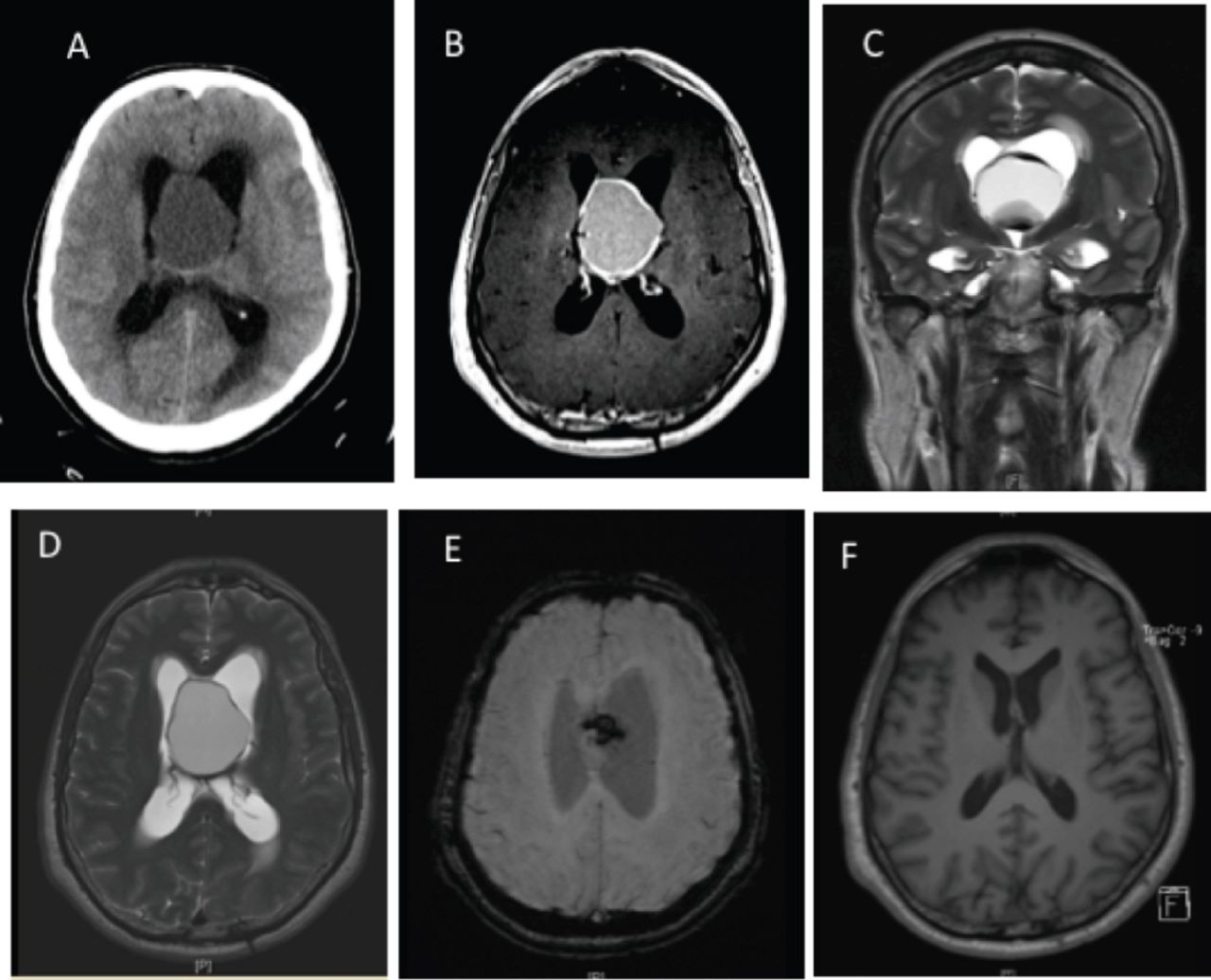
The patient’s initial computed tomography (CT) scan showed a large cystic lesion with peripheral hyperdensities causing acute hydrocephalus. Magnetic resonance (MR) images showed a large intraventricular mass at the foramen of Monro measuring 4.3cm×4.0cm×3.2cm, pushing the septum pellucidum to the right and causing acute lateral ventricular dilatation. The mass was largely cystic and had a thick wall and solid components inferiorly, demonstrating hyperintensity on T1-weighted images and multilayered hypointensity on T2-weighted images with remarkable susceptibility artifacts in the wall and in the inferior part, indicating hemosiderin deposition (Figure 1). The solid component in the inferior part of the lesion demonstrated mild diffusion restriction, which likely represented bleeding at different ages. The wall of the cystic component of the lesion demonstrated thick enhancement, which was irregular in some places; the solid component did not show enhancement. The perfusion scans did not show increased perfusion. Furthermore, the MR arteriogram study showed normal intracranial arteries with no displacement or occlusion.

Radiological images of case 1. A) Axial preoperative CT scan showing a large cystic lesion with peripheral hyperdensities causing acute hydrocephalus. B) An axial T1-weighted image showing a large, hyperintense, intraventricular mass, with a thick wall and a solid component in the inferior part, C and D) which demonstrates multilayered hypointensity on coronal and axial T2-weighted images, E) with a remarkable susceptibility artifact on susceptibility-weighted imaging (SWI), F) Axial postoperative T1-weighted image.
Therapeutic intervention
The patient then underwent a frontal craniotomy and an interhemispheric, transcallosal transventricular approach to resect the cyst, as well as left frontal external ventricular drain (EVD). The patient recovered and tolerated the surgery. Pathological examination confirmed a hemorrhage within the colloid cyst.
Follow-up and outcomes
At the one month follow up visit, the patient exhibited enhanced cognitive function and complete resolution of the headaches (figure 2).
A 47-year-old male (Case 2) presented with progressive morning headaches for a total of 10 days, which were associated with nausea and vomiting. He had no history of trauma or loss of consciousness.
Case 2. Patient’s information
A 55-year-old male presented with progressive memory disturbance and unsteady gait for 8 months, which became more profound at the time of presentation.
Clinical findings
A higher cognitive function examination revealed impairments in short-term memory. A fundoscopic examination revealed bilateral papilledema. The patient’s cranial nerve, as well as his motor and sensory examinations, were normal except for bilateral extensor plantar reflexes. Cerebellar examination revealed impaired tandem walking.
Diagnostic assessment
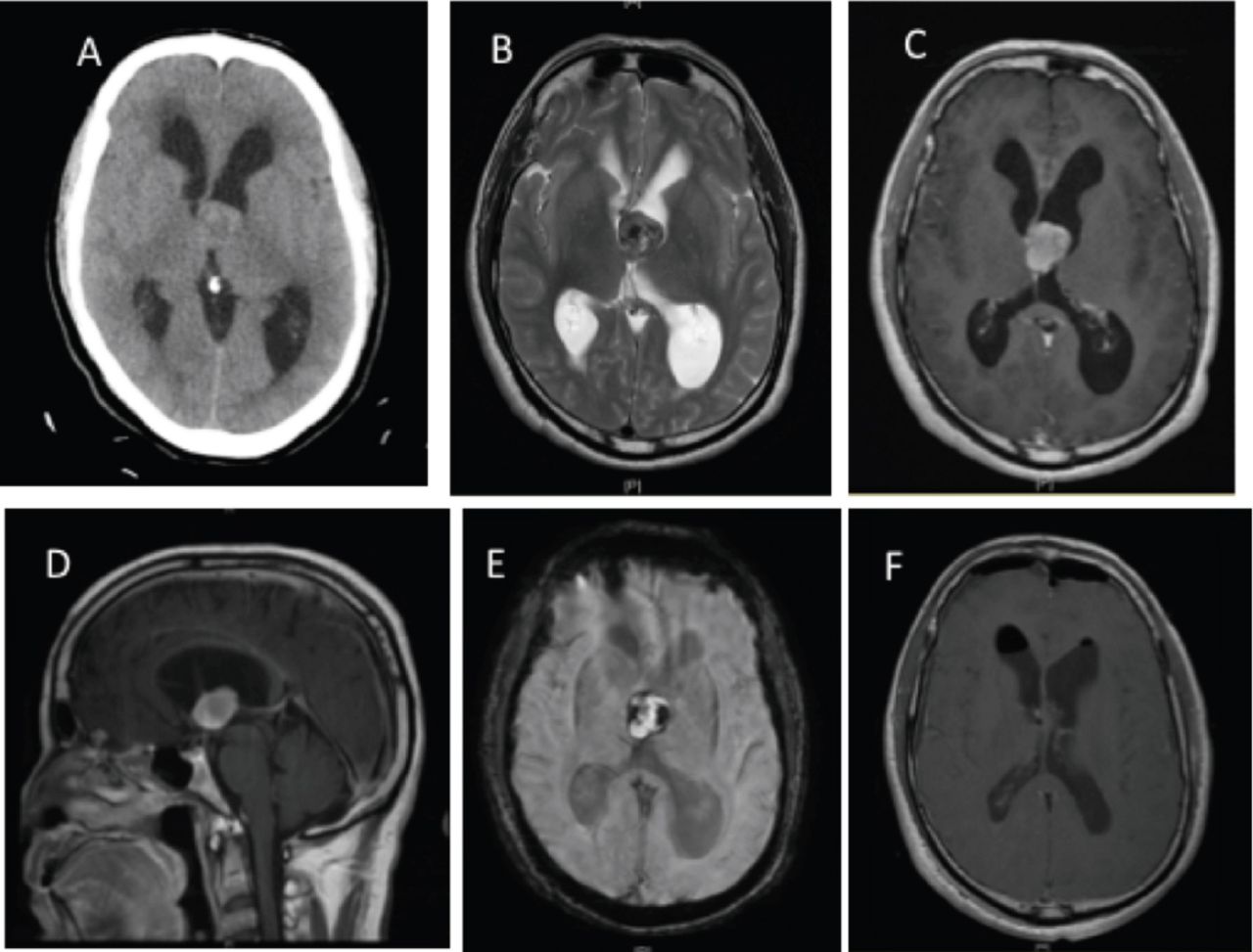
The patient’s initial CT scan showed a heterogeneous mass that adhered to the septum pellucidum at the level of the foramen of Monro; this was associated with bilateral ventricular hydrocephalus laterally and a mild midline shift. Magnetic resonance images showed a heterogeneous, rounded, intraventricular cystic lesion within the dilated left foramen of Monro and with extension into the third ventricle, causing a shift of the septum pellucidum to the right by 9.4 mm. There was also an obstruction of the ipsilateral foramen of Monro, resulting in obstructive hydrocephalus of the lateral ventricles. The lesion was hyperintense on T1-weighted images, intermediate to hypointense on T2-weighted images with peripheral hemorrhagic susceptibility artifacts, and it did not show any signs of diffusion restriction (Figure 3).

Radiological images of case 1. A) Axial CT scan showing a heterogeneous mass adherent to the septum pellucidum at the level of the foramen of Monro associated with bilateral ventricular hydrocephalus laterally and a mild midline shift. B) An axial T2-weighted image showing an intermediate to hypointense heterogeneous intraventricular cystic lesion resulting in obstructive hydrocephalus of the lateral ventricles. C and D) Axial and sagittal T1-weighted images showing hyperintensity of the lesion. E) An axial SWI demonstrating multiple peripheral, hemorrhagic susceptibility artifacts. F) An axial postoperative T1-weighted image showing complete excision of the colloid cyst, improvements in hydrocephalus, a small intraventricular hemorrhage, and a small amount of air.
Therapeutic intervention
The patient subsequently underwent a left frontal craniotomy and transcallosal resection of the colloid cyst. The patient tolerated the surgery and his unsteady gait improved slightly; however, he developed aphasia postoperatively.
Follow-up and Outcomes
At the 2-month follow-up visit, the patient was walking independently, his memory showed signs of improvement, and his aphasia demonstrated improvements in speech. A pathological examination of the excised lesion confirmed the presence of a hemorrhage within the colloid cyst (figure 4).

A 55-year-old male (case 2) presented with progressive memory disturbance and unsteady gait for 8 months, which became more profound at the time of presentation.
Discussion
The reported estimated incidence of third ventricle colloid cysts (TVCC) is approximately one per one million.6 Colloid cysts account for 0.5%-1% of all intracranial tumors.7,8 Generally, colloid cysts are benign and most cases are asymptomatic,1 with both genders being affected at equal rates. Symptomatic intracystic hemorrhage within these colloid cysts is rarely encountered. A PubMed search was conducted for this literature review, and the following keywords were used: “Hemorrhagic colloid cyst” and “Colloid cyst and Hemorrhage”. There were only 13 clinically diagnosed cases of these cysts reported in the literature,2,3,9-19 and 5 additional cases were reported at the time of autopsy.4,5,20-22 Of these 5 cases, only 3 had associated risk factors,4,5,11 - 2 cases had arterial hypertension and one case demonstrated bleeding tendencies. Although it is unknown whether these factors contributed to colloid cyst bleeding, arterial hypertension and coagulation abnormalities may have played a role and should be carefully considered in patients with colloid cysts in the future.14
The mechanisms underlying sudden death in patients with colloid cysts are poorly described in the literature, with several authors postulating that hydrocephalus and brain herniation serve as the direct causes of the rapid deterioration that precedes mortality.23,24 Moreover, intracystic hemorrhage should be considered as a possible mechanism for sudden deterioration in these patients as well.14 Table 1 summarizes the characteristics, clinical presentation, imaging features, pathological confirmation, treatment methods, and outcomes of all clinically reported cases.
The characteristics, clinical presentation, imaging features, pathological confirmation, treatment methods, and outcomes of all clinically reported cases.
Interestingly, the ages of the reported cases ranged from 9-77 years old, with a mean age of 39.67 years; there was only one pediatric case. In all, there were 8 males and 5 females. Most of the clinical cases reportedly presented with signs of raised intracranial pressure due to obstructive hydrocephalus.
Six of the 13 cases reportedly demonstrated rapid deterioration of the patient’s clinical picture following the initial presentation.2,3,9-11,19 Of those 6 cases, 4 had poor outcomes,2,10,11,19 illustrating that the degree of rapidity with which clinical deterioration occurs may play a role in the subsequent outcomes of these patients. All cases demonstrated the typical imaging features associated with a hemorrhagic colloid cyst, including hypointense areas along the wall of the cyst on T2-weighted images and susceptibility artifacts, which are suggestive of a bleed; these were histopathologically confirmed.2,3,9-19
The first clinically diagnosed case of a hemorrhagic colloid cyst, reported by Beems et al,2 was initially treated by an emergency ventriculotomy followed by elective endoscopic cyst removal. Additionally, Carrasco et al,11 reported a case of a hemorrhagic colloid cyst where a safe surgical strategy was employed, consisting of elective microsurgical removal following EVD.
The only pediatric case, reported by Farooq et al,3 was of a 9-year-old girl with a hemorrhagic colloid cyst; this patient had initially presented with sudden deterioration in her level of consciousness. She was treated with a similar approach with good clinical outcomes. In fact, most of the reported cases were also treated with a similar approach (Table 1).10,13-19 Only one case presented with abrupt anterograde amnesia, which was treated by direct emergency neuro-endoscopic excision of the cyst; this patient demonstrated complete resolution of the anterograde amnesia following surgical removal of the cyst. This case emphasized the importance of timely surgical excision on rapid improvements in memory disturbances.12 Similarly, one of our cases presented with the gradual onset of memory disturbances; this patient was treated with direct surgical removal and had similar outcomes.
Four out of the 13 reported cases were treated endoscopically.2,10,12,18 Only one reported case was treated by stereotactic aspiration followed by ventricular drainage, then stereotactic aspiration with endoscopic guidance and subtotal excision of the cyst.9 The rest of the cases were treated by an open approach.3,11,14,15,19 Our 2 cases were treated by an open transcallosal approach. In both of our cases, there were severe adhesions at the surgical field which can make the endoscopic approach and stereotactic aspiration very difficult. So, in theory, we suggest to go with an open approach in hemorrhagic cases.
The outcomes were poor in 4 cases,2,10,11,19 satisfactory in 3,9,14,15 and good with complete resolution in 5.3,13,16-18 All 4 cases that experienced poor outcomes tended to undergo rapid clinical deterioration following their initial presentation.
In conclusion, a hemorrhagic colloid cyst is a rare entity; however, bleeding tendencies and risk factors for bleeding should be carefully considered in patients with these cysts. The degree of rapidity in which clinical deterioration occurs may play a major role in the preferred treatment approach and in subsequent outcomes.
Footnotes
Disclosure. The authors declare no conflicting interests, support or funding from any drug company.
- Received January 29, 2018.
- Accepted June 20, 2018.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.