


Article Figures & Data
Figures
- Figure 1
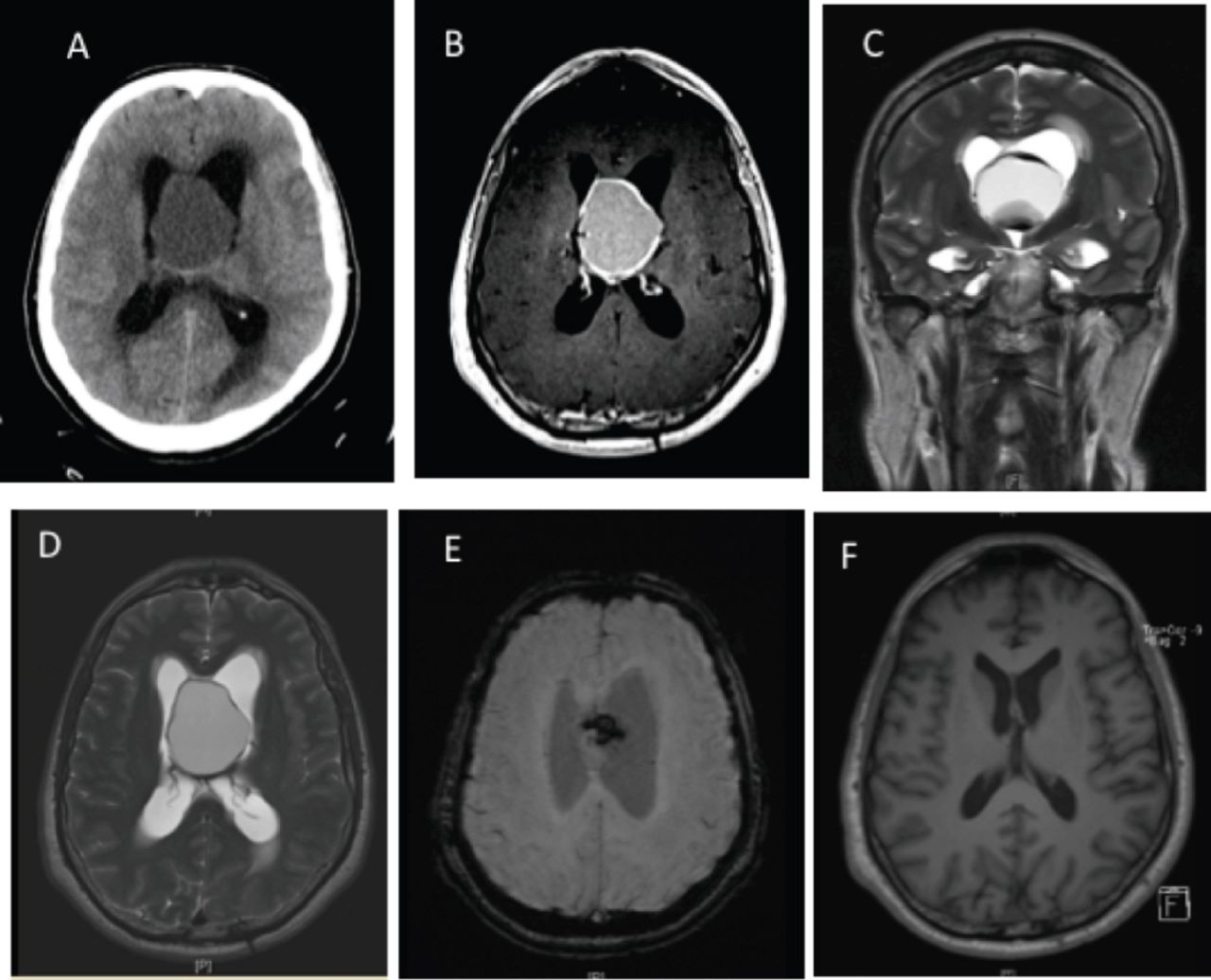
Radiological images of case 1. A) Axial preoperative CT scan showing a large cystic lesion with peripheral hyperdensities causing acute hydrocephalus. B) An axial T1-weighted image showing a large, hyperintense, intraventricular mass, with a thick wall and a solid component in the inferior part, C and D) which demonstrates multilayered hypointensity on coronal and axial T2-weighted images, E) with a remarkable susceptibility artifact on susceptibility-weighted imaging (SWI), F) Axial postoperative T1-weighted image.
- Figure 2
A 47-year-old male (Case 2) presented with progressive morning headaches for a total of 10 days, which were associated with nausea and vomiting. He had no history of trauma or loss of consciousness.
- Figure 3
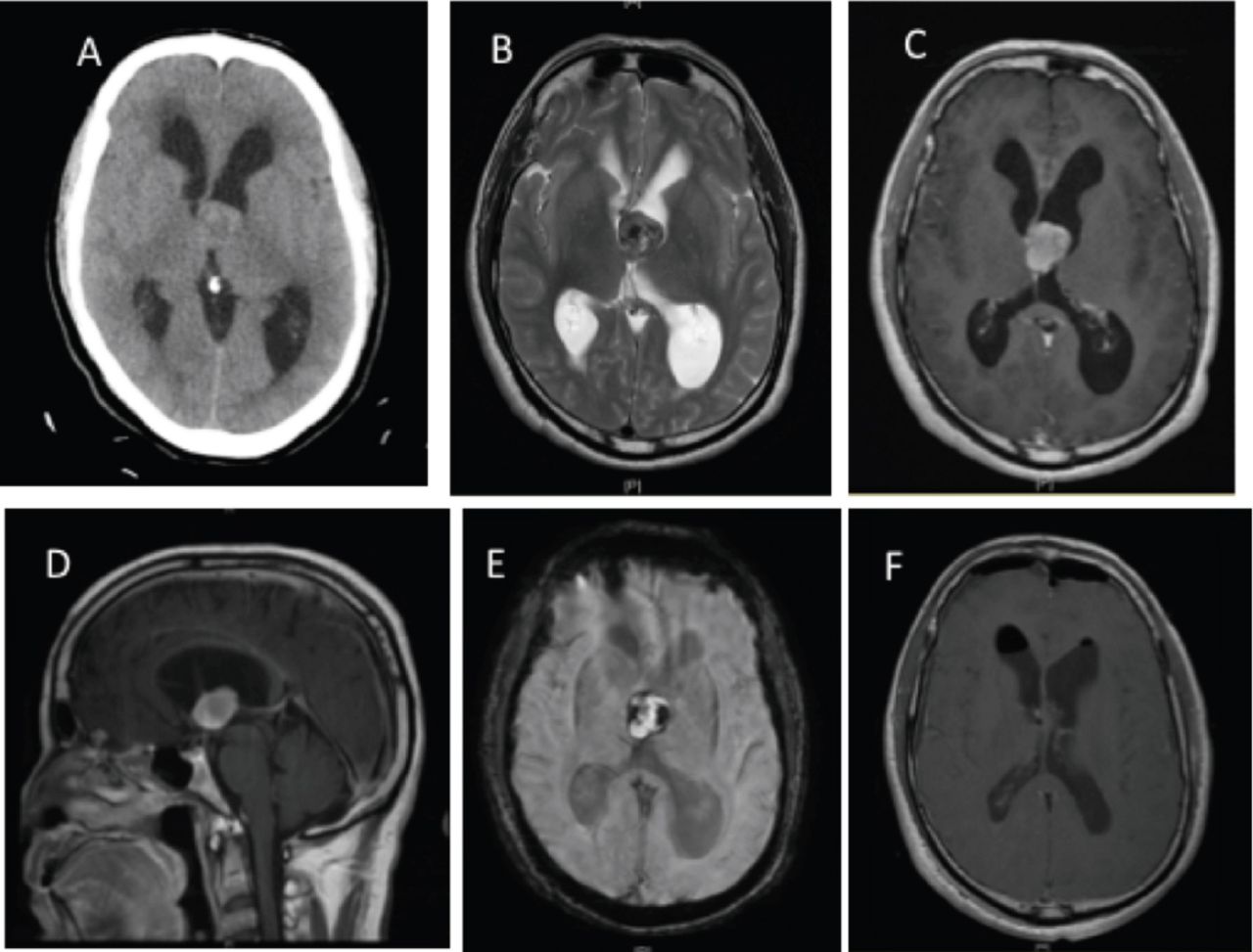
Radiological images of case 1. A) Axial CT scan showing a heterogeneous mass adherent to the septum pellucidum at the level of the foramen of Monro associated with bilateral ventricular hydrocephalus laterally and a mild midline shift. B) An axial T2-weighted image showing an intermediate to hypointense heterogeneous intraventricular cystic lesion resulting in obstructive hydrocephalus of the lateral ventricles. C and D) Axial and sagittal T1-weighted images showing hyperintensity of the lesion. E) An axial SWI demonstrating multiple peripheral, hemorrhagic susceptibility artifacts. F) An axial postoperative T1-weighted image showing complete excision of the colloid cyst, improvements in hydrocephalus, a small intraventricular hemorrhage, and a small amount of air.
- Figure 4
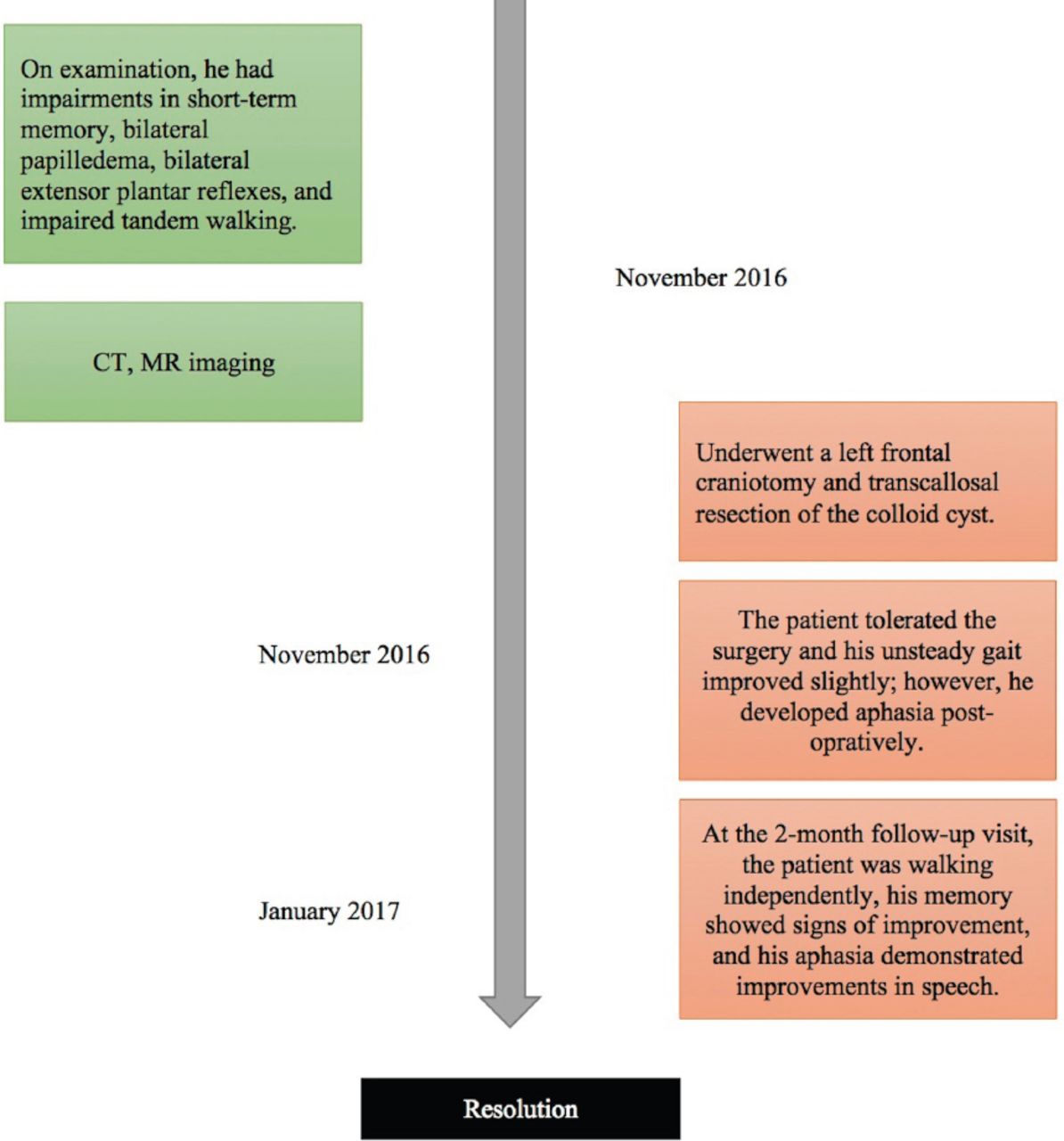
A 55-year-old male (case 2) presented with progressive memory disturbance and unsteady gait for 8 months, which became more profound at the time of presentation.



Tables
- Table 1
The characteristics, clinical presentation, imaging features, pathological confirmation, treatment methods, and outcomes of all clinically reported cases.
Authors Age/Gender Comorbidities Clinical course Radiological features of CC Pathology confirmation Treatment Outcome/Follow-up period (2) 35/F A known case of a colloid cyst, as well as progressive headaches and memory disturbances, followed by progressive deterioration and 2 seizure episodes. + + Emergency ventriculostomy followed by endoscopic subtotal excision of the cyst. Poor; after few months post-op, was still fully dependent on others. (3) 9/F Headache, nausea, and sudden deterioration in mental status. + + Emergency ventriculostomy, followed by craniotomy and cyst excision. Tolerated the procedure well and was discharged on postoperative day 3 without any neurological complications. (9) 48/M Headaches and a memory deficit for 2 weeks, followed by sudden deterioration. + NA Stereotactic aspiration with limited evacuation. Followed by ventricular drainage due to herniation. Renewed stereotactic aspiration with endoscopic guidance and subtotal excision of the cyst. Residual cyst with a slow increase in cyst size, radiologically. (10) 29/F Mental status deterioration, Glasgow Coma Scale 4 with respiratory insufficiency. + + Emergency ventricular drainage followed by endoscopic removal. The radiological results were excellent, but there were poor clinical outcomes (vegetative state). (11) 47/M Hypertension Acute right-sided hemiparesis and speech impediment, followed by rapid deterioration of consciousness. + + Emergency EVD followed by elective total resection of the lesion via a transcallosal route. Right-sided hemiparesis (3/5) with impaired propioception and a mixed-type sensitive and motor dysphasia (1 year post-op). A neuropsychological assessment revealed bradipsychia and anosognosia, as well as attention, concentration, and memory deficits. (12) 48/M A 4-day progressive headache followed by the sudden onset of 24-hour anterograde amnesia. (Normal neurological examination without papilloedema.) + + Emergency neuro-endoscopic total excision of the cyst. The patient’s amnesia completely resolved within 24 hours post op, and he was discharged home 2 days later. Returned to full-time employment (2 months post-operatively). (13) 28/ M Known case of a colloid cyst with unilateral hydrocephalus and a right ventriculo-peritoneal shunt for 8 years. Presented with severe headache and multiple episodes of vomiting for 1 day. + + Right frontal craniotomy, with total excision of the cyst (an anterior interhemispheric, transcallosal–ransventricular approach). EVD for 3 days. At 1-year follow-up, he has no neurological deficits and the headache has resolved. (14) 77/M Type II diabetes mellitus. On warfarin for atrial fibrillation; INR: 1.2 Unsteady gait, incontinence, and gradually worsening confusion over 3 weeks. The GCS was 14, with mild right-sided weakness; power 4/5. The cranial nerves were intact. + + Right frontal craniotomy with total excision of the cyst. (transcortical approach). Ventriculoperitoneal shunt for delayed hydrocephalus. Satisfactory with rehabilitation. (15) 20/F Progressive headache, three episodes of generalized tonic clonic seizures, gait disturbances, impaired short-term memory, bilateral papilloedema, extensor plantar reflex and (+) Romberg’s sign. + + Right frontoparietal craniotomy with total excision of the cyst (interhemispheric transcallosal approach). Seizure-free and improved memory function in 3 weeks. (16) 47/ F Headache, N/V, papilledema, GCS of 13. + + Ventriculostomy followed by craniotomy and total excision of the cyst. Uneventful recovery. (17) 35/M Progressive increasing headaches over months; nausea, transient loss of consciousness, and incontinence. + + Total removal of the cyst (transcallosal approach). No neurological complications. (18) 43/M Known case of colloid cyst of the third ventricle without evidence of ventriculomegaly for 6 years; presented with sudden onset of headache. Intact level of consciousness with no neurological deficits. + + Elective endoscopic partial removal of the cyst. Resolved headache postoperatively without any neurological deficits. Follow-up imaging demonstrated a gradual reduction in the residual cyst size and normalization of the size of the lateral ventricle. (19) 45/M Headache and malaise initially, then rapid deterioration of consciousness; GCS of 3. + + EVD initially on each side. Intensive care unit admission where brain death was certified. This was followed, however, by craniotomy with excision of the cyst (transcortical frontal approach). Brain death. Case 1 47/M Type II diabetes mellitus, long-term smoker. Progressive morning headaches for 10 days associated with nausea and vomiting. Bilateral papilledema. + + Frontal craniotomy and interhemispheric transcallosal transventricular approach for cyst excision. Left frontal EVD. Resolved headache. Case 2 51/M Progressive memory disturbance and unsteady gait for 8 months. Bilateral papilledema. + + Left frontal craniotomy and transcallosal resection of the colloid cyst. Aphasia postoperatively, which improved with speech therapy. Unsteady gait demonstrated slight improvements. M - male, F - female, EVD - external ventricular drain, ND - no data.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.